Introduction
Irritable bowel syndrome (IBS) is a chronic
functional bowel disorder characterized by a combination of
symptoms that have a considerable impact on the patient’s quality
of life. These symptoms include abdominal pain or discomfort and
altered bowel habits (1,2). IBS is more common in females than in
males, and is diagnosed more frequently in patients under the age
of 50 (1). The prevalence of IBS
has been calculated to range from 5–15% of the population
worldwide, as determined by diagnostic criteria, such as the Rome
criteria (1–14).
Approximately two-thirds of patients with IBS
consider their symptoms to be related to their diet (15) and therefore restrict their intake
of certain dietary agents that they perceive to be provocative. The
most commonly reported triggers are carbohydrates and fatty foods,
milk and dairy products, wheat products, caffeine, hot spices,
certain meats, cabbage, onions, peas, beans and fried and smoked
foods (16–19). Despite these reported effects,
numerous studies have demonstrated that dietary composition does
not markedly differ between patients with IBS and controls
(15–21), although patients with IBS appear to
have a low intake of calcium, potassium, magnesium, vitamin A,
vitamin B12 and riboflavin (16,18,20,21).
In a previous study by our group, dietary guidance
administered individually to patients with IBS reduced the symptoms
of the condition and improved their quality of life, in addition to
affecting their habitual diet so that their intake of minerals and
vitamins became normalized (18).
However, two groups of patients with IBS were compared in the
study; one group received individual dietary guidance, whilst the
second did not receive any dietary guidance. There were several
important factors in the investigation that may have affected the
outcome of the study, but were not able to be excluded, such as the
differences in gender distribution and social background between
the two groups. The present investigation was designed to control
for these factors, and studied the effects in the same individuals
before and 3–9 months after receiving individual dietary
guidance.
Material and methods
Patients
Patients who had been referred to the
gastroenterology department of Stord Helse-Fonna Hospital (Stord,
Norway), and who fulfilled the Rome III criteria for the diagnosis
of IBS were considered for inclusion in the study. Although both
genders were able to participate, the patients were required to be
between 18 and 69 years of age. Exclusion criteria comprised the
presence of organic gastrointestinal disease, clinically
significant systemic diseases, pregnancy or lactation, drug abuse,
serious psychiatric diseases and collaboration issues. In addition,
with the exception of appendectomy, cesarean section and
hysterectomy, patients who had undergone abdominal surgery were
excluded. This study was performed in accordance with the
Declaration of Helsinki and was approved by the Regional Committee
for Medical and Health Research Ethics West, Bergen, Norway. All
patients provided oral and written consent to participate.
Study design
In total, 46 patients were included in the study.
This included 35 females and 11 males with a mean age of 35 years
(range, 18–69 years). Of these, 21 reported diarrhea (IBS-D), 18
reported constipation (IBS-C) and seven reported a mixture of both
symptoms (IBS-M) as the predominant symptom of IBS. The patients
underwent a complete physical examination, a gastroscopy with
duodenal biopsies, a colonoscopy with segmental biopsies and
several blood tests to exclude other organic causes for their
symptoms. Each patient received three sessions of individual
guidance on dietary management from a registered nurse with a
specific education in IBS diet, with each session lasting ~45 min.
The patients were asked to complete the following questionnaires
before and ≥3 months subsequent to receiving the dietary guidance:
The Birmingham IBS symptom score questionnaire, the IBS-Quality of
Life (IBS-QOL) questionnaire, the Norwegian version of the
Short-Form Nepean and Dyspepsia Index (SF-NDI) questionnaire and
the MoBa Food Frequency Questionnaire (MoBa FFQ).
Individual guidance on diet
management
Each patient attended three 45 min sessions with a
registered nurse with special training in the IBS diet, and seven
years experience of providing dietary guidance to patients with
IBS. The sessions were scheduled with intervals of ≥2 weeks between
them. The information at the sessions was provided orally, and
using charts and illustrative drawings. Written information was
also supplied.
In the first session, the patient received general
information with regard to the importance of regular meals and
healthy eating habits, along with the effect of the diet on the
development of symptoms. Emphasis was placed on the role of poorly
absorbed, highly fermentable oligosaccharides, disaccharides,
monosaccharides and polyols (FODMAPs), although patients were also
informed of the effects of soluble and insoluble dietary fibers. It
was emphasized that milk and dairy products were not triggers for
IBS symptoms, and that the patients should consume dairy products
daily. The patient was asked to keep a diary in which they recorded
the time of eating/drinking, and the types of food and drinks they
ingested daily. In addition, they were asked to report the
occurrence of abdominal pain, abdominal distention and bloating, as
well as stool frequency and consistency. The patients were
instructed to try protein-, fat-, and carbohydrate-rich/poor diets
and report the symptoms for each in the diary. This was performed
over a 2-week period.
In the second scheduled session, the information
provided in the first session was summarized, before the diary was
examined to determine which food items may be triggering the
patient’s symptoms. The patients were then advised to avoid these
items and other items that were rich in FODMAPs and insoluble
fibers, such as onions, garlic, paprika, cabbage, carbonated
beverages, ‘lite’ products (those containing artificial
sweeteners), bananas, beans and peas. The patient was asked to
replace wheat and wheat products with spelt and spelt products,
respectively, and was provided with a list of vegetables and fruits
that contained lower levels of FODMAPs and insoluble fibers
(18). The patients were also
instructed to avoid the intake of food items supplemented with
probiotics during the course of the study.
During the third and final session, the patient’s
experience regarding the management of their diet was discussed
with the nurse, so that the patient and nurse were then able to
utilize this information to design a suitable diet for the patient
to follow.
IBS symptom assessment
The Birmingham IBS symptom score questionnaire was
developed to measure the symptoms of patients with IBS. It is
disease-specific, acceptable to patients and suitable for
self-completion. Its dimensions have been demonstrated to have good
reliability, external validity and sensitivity (22). The Birmingham IBS symptom score
questionnaire consists of 11 questions based on the frequency of
IBS symptoms. The responses to the questions are measured on a
six-point Likert scale, ranging from 0 (none of the time) to 5 (all
of the time). The questionnaire has three underlying dimensions:
pain (three items), diarrhea (five items) and constipation (three
items), with lower scores indicating improved symptoms.
Assessment of quality of life
The quality of life in patients with IBS was
assessed by the IBS-QOL and SF-NDI questionnaires.
The IBS-QOL questionnaire is a 34-item, IBS-specific
quality of life measure that assesses physical and psychosocial
functioning as a result of IBS (23,24).
The questionnaire comprises eight domains; dysphoria, interference
with activity, body image, health concerns, food avoidance, social
reaction, sexual function and impact on relations. Responses are
provided on the following five-point Likert scale: not at all,
slightly, moderately, quite a lot and extremely.
The SF-NDI questionnaire is a disease-specific
measure of the health-related quality of life (HRQoL), with 10
questions divided into five subscale scores (tension, interference
with daily activities, disruption to regular eating/drinking,
knowledge towards/control over disease symptoms and interference
with work/study). Each question has five options, ranging from 1
(not at all) to 5 (extremely); thus, the total score ranges from
10–50, as per the developer’s original calculation formula, with
higher scores indicating worse functioning or symptoms. This
questionnaire was constructed and validated primarily in patients
with dyspepsia (25). A Norwegian
translation of the questionnaire was validated and demonstrated to
perform well in patients with IBS (26).
Dietary assessment
Dietary intake was assessed using a
semi-quantitative, self-administered food frequency questionnaire
(MoBa FFQ). The MoBa FFQ asks participants to report the frequency
of consumption and portion size of certain items over a defined
period of time. Each item is defined by a series of foods or
beverages. Additional questions on food purchasing and preparation
methods enable the analysis software to further refine nutrient
calculations. The MoBa FFQ used in this study was developed and
validated by the Norwegian Institute of Public Health in Oslo,
Norway (27,28). It enquires about the intake of 225
food items, grouped according to typical Norwegian meal patterns,
and is designed to capture the dietary habits of the participant
over a defined period, including the intake of any oral
supplements. Analysis of the obtained data provides information
concerning the intake of energy, water, macronutrients,
micronutrients, minerals and alcohol, in addition to 100 specific
food groups and items. It also yields information regarding meal
patterns.
Statistical analysis
The paired t-test was used to analyze the data. The
data are presented as the mean ± SEM values, and P<0.05 was
considered to indicate a statistically significant difference.
Results
Patients
Of the 46 patients recruited to this study, 18
abandoned the study; one was excluded due to non-compliance and one
due to cooperation problems; four became better following the
dietary guidance sessions, and then lost interest in and motivation
for completing the study; two were diagnosed with celiac disease;
one was diagnosed with lupus; one became pregnant and one moved
abroad during the study. Thus, 17 of the original 46 patient cohort
completed the study. These patients comprised 12 females and five
males with a mean age of 34 years (range, 20–45 years); six of the
17 were IBS-D, eight were IBS-C and three were IBS-M. The time
taken between receiving dietary guidance and completing the second
set of questionnaires ranged from 3–9 months (median, 4
months).
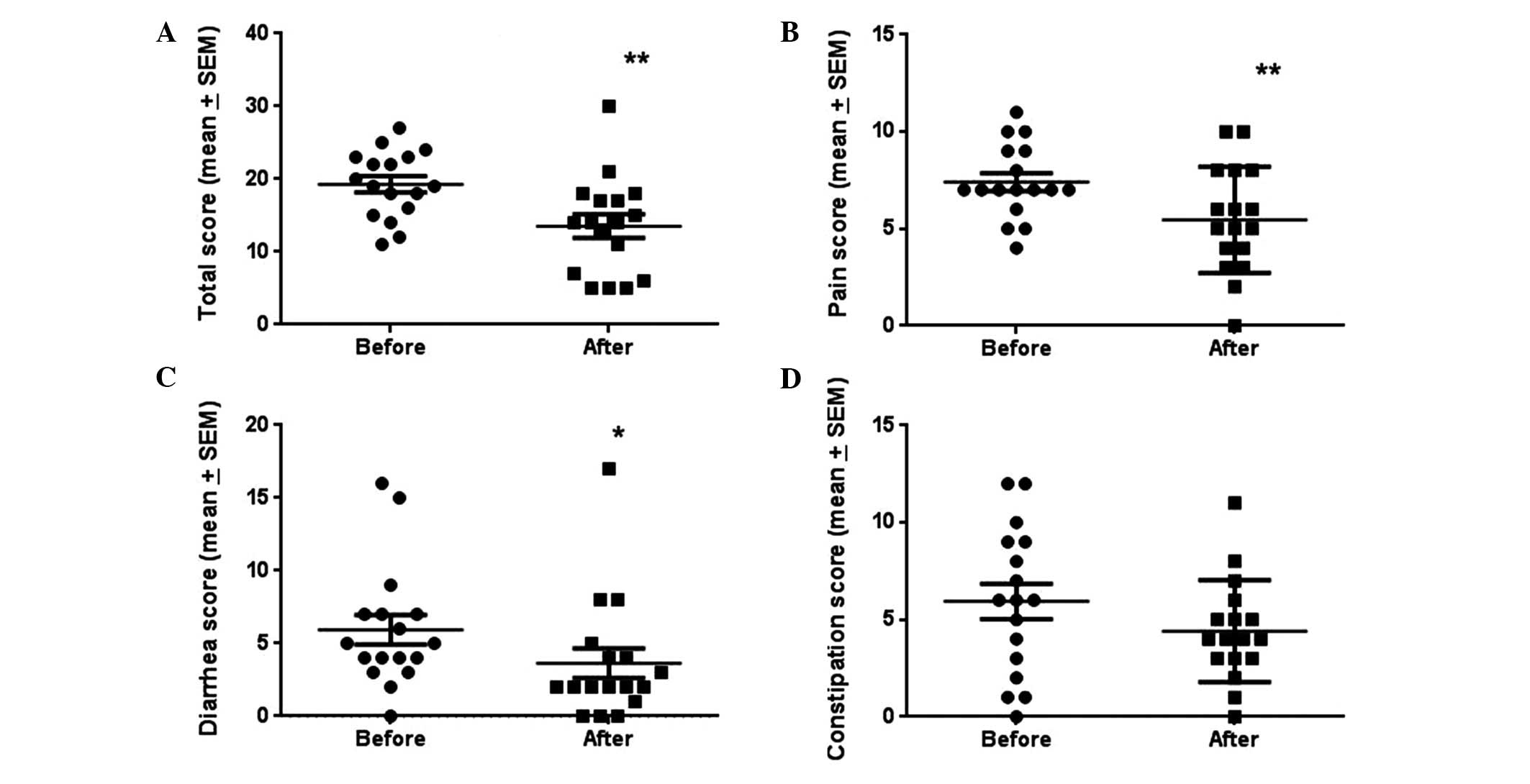
Birmingham IBS symptom score
questionnaire
The total scores of the Birmingham IBS symptom score
questionnaires before and subsequent to receiving dietary guidance
were 41.47±1.62 and 35.71±1.12, respectively. The reduction in
symptoms was statistically significant (P=0.001). All three of the
questionnaire dimensions (i.e., abdominal pain, diarrhea and
constipation) were also reduced following the dietary guidance
sessions; however, the result for constipation was not
statistically significant (Fig.
1).
IBS-QOL
The total IBS-QOL score increased significantly from
125.4±4.2 to 136.8±3.8 following the dietary guidance sessions
(P=0.003). This improvement was statistically significant in all
domains, with the exception of the impact on relations (Fig. 2 and Table I).
 | Table IScores on the eight domains of the
Irritable Bowel Syndrome-Quality of Life (IBS-QOL) questionnaire in
patients with IBS before and following dietary guidance
sessions. |
Table I
Scores on the eight domains of the
Irritable Bowel Syndrome-Quality of Life (IBS-QOL) questionnaire in
patients with IBS before and following dietary guidance
sessions.
| IBS-QOL score | |
|---|
|
| |
|---|
| Domain | Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| Dysphoria | 28.1±1.4 | 31.5±0.9 | 0.009b |
| Interference with
activity | 18.6±0.7 | 20.9±0.7 | 0.003b |
| Body image | 18.1±0.8 | 20.0±1.1 | 0.007b |
| Health worry | 15.2±0.7 | 16.9±0.6 | 0.001b |
| Food avoidance | 5.8±0.6 | 4.6±0.4 | 0.018b |
| Social reactions | 18.8±0.8 | 20.6±0.7 | 0.021a |
| Sexual function | 8.2±0.4 | 8.9±0.3 | 0.035a |
| Impact on
relations | 12.8±0.4 | 13.4±0.4 | 0.172 |
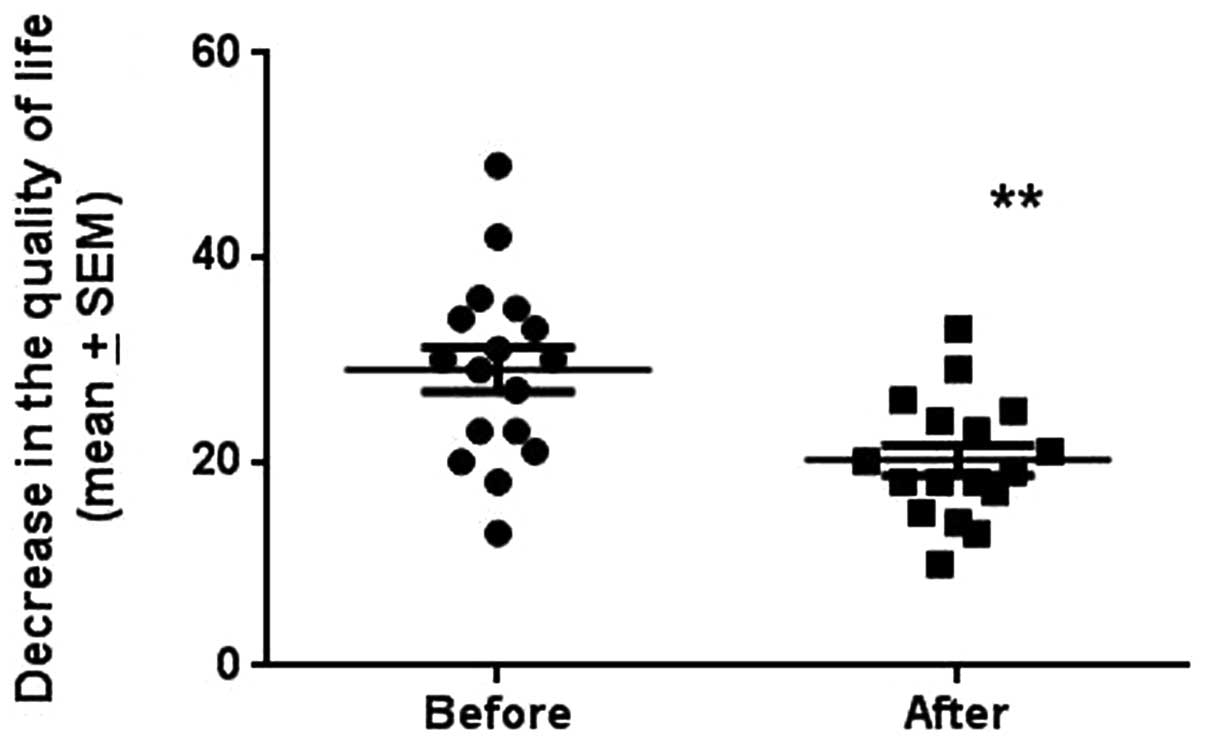
SF-NDI
The total SF-NDI scores (which reflect the reduction
in HRQoL) before and following the dietary guidance sessions were
29.1±2.2 and 20.2±1.5, respectively. This improvement in HRQoL was
statistically significant (P=0.002; Fig. 3).
MoBa FFQ
There were no statistically significant differences
in the intake of calories, carbohydrate (total and starch), fiber,
protein, fat (total, saturated and trans-, mono- and
polyunsaturated), sugar or alcohol in the patients with IBS who
received dietary guidance (Table
II). However, there was a significant increase in the intake of
cholesterol. The dietary guidance did not affect the meal pattern
in the patients with IBS (Table
III). There was an increase in the consumption of various dairy
products, although the change was not statistically significant
(Table IV). However, there was a
decrease in the consumption of dairy products with probiotic
supplements, in line with our recommendation during the study.
Although the intake of β-carotene, retinol equivalents, calcium and
riboflavin was increased, only the increase in vitamin
B12 was statistically significant (Table V). There was a significant
reduction in the consumption of various FODMAP- and insoluble
fiber-rich fruits and vegetables (Table VI). The replacement of wheat and
wheat products with spelt and spelt products, respectively, enabled
the patients to consume the food items that they considered
essential (Table VII).
| Table IIDaily intake of macronutrients and
alcohol in patients with irritable bowel syndrome (IBS) before and
following dietary guidance sessions. |
Table II
Daily intake of macronutrients and
alcohol in patients with irritable bowel syndrome (IBS) before and
following dietary guidance sessions.
| Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| Energy (kcal) | 1968±183 | 1889±219 | 0.610 |
| Carbohydrates
(g) |
| Total | 249.7±28.6 | 228.3±30.0 | 0.342 |
| Starch | 125.8±15.5 | 108.2±13.1 | 0.185 |
| Fiber (g) | 27.4±2.5 | 23.1±2.2 | 0.093 |
| Protein (g) | 75.7±5.5 | 78.2±9.4 | 0.704 |
| Fats (g) |
| Total | 72.5±6.3 | 72.3±7.6 | 0.967 |
| Saturated | 26.6±2.6 | 26.5±3.2 | 0.965 |
| Cholesterol | 232.6±26.0 | 288.6±38.9 | 0.040a |
| Trans | 1.4±0.2 | 1.8±0.4 | 0.243 |
|
Monounsaturated | 24.2±2.1 | 24.4±2.4 | 0.918 |
|
Polyunsaturated | 14.9±1.4 | 13.9±1.3 | 0.334 |
| Sugar (g) | 50.4±8.3 | 49.4±9.2 | 0.876 |
| Alcohol (ml) | 1.4±0.6 | 1.2±0.4 | 0.620 |
| Table IIIWeekly pattern of meal types in
patients with irritable bowel syndrome (IBS) before and following
dietary guidance sessions. |
Table III
Weekly pattern of meal types in
patients with irritable bowel syndrome (IBS) before and following
dietary guidance sessions.
| Number of
meals | |
|---|
|
| |
|---|
| Meal type | Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| Breakfast | 2.1±0.5 | 1.8±0.4 | 0.260 |
| Morning snack | 5.4±0.6 | 4.4±0.5 | 0.256 |
| Lunch | 3.9±0.6 | 3.0±0.5 | 0.219 |
| Snack before
dinner | 6.2±0.6 | 5.9±0.6 | 0.716 |
| Dinner | 1.4±0.2 | 1.3±0.2 | 0.579 |
| Evening snack | 5.6±0.6 | 6.2±0.5 | 0.370 |
| Supper | 3.1±0.5 | 3.2±0.4 | 0.675 |
| Night time
meal | 7.4±0.5 | 7.2±0.5 | 0.867 |
| Table IVDaily intake of dairy products,
artificial sweeteners and soft drinks in patients with irritable
bowel syndrome (IBS) before and following dietary guidance
sessions. |
Table IV
Daily intake of dairy products,
artificial sweeteners and soft drinks in patients with irritable
bowel syndrome (IBS) before and following dietary guidance
sessions.
| Dairy products | Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| Milk products,
whole fat (g) | 0.8±0.5 | 6.2±5.0 | 0.262 |
| Milk products, low
fat (g) | 118.8±59.9 | 138.7±82.8 | 0.506 |
| Sour milk with
probiotic supplement (g) | 31.5±29.3 | 4.5±2.6 | 0.339 |
| Yoghurt (g) | 14.1±4.6 | 34.4±10.6 | 0.070 |
| Soya milk (g) | 0.9±0.6 | 1.3±0.9 | 0.332 |
| Cheese, whole fat
(g) | 7.0±2.9 | 7.8±3.7 | 0.676 |
| Cheese, low fat
(g) | 0.2±0.1 | 0.4±0.2 | 0.260 |
| Brown goat’s cheese
(g) | 1.1±0.4 | 2.6±1.8 | 0.335 |
| Artificial
sweeteners (mg) | 0.02±0.01 | 0.01±0.01 | 0.163 |
| Soft drinks,
sweetened (ml) | 71.3±31.9 | 53.5±20.7 | 0.478 |
| Soft drinks,
unsweetened (ml) | 91.7±39.8 | 37.5±29.2 | 0.085 |
| Table VDaily intake of vitamins and minerals
in patients with irritable bowel syndrome (IBS) before and
following dietary guidance sessions. |
Table V
Daily intake of vitamins and minerals
in patients with irritable bowel syndrome (IBS) before and
following dietary guidance sessions.
| Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| Vitamins |
| β-carotene
(mg) | 2543±511 | 2721±360 | 0.624 |
| Folate (μg) | 224.8±17.8 | 223.2±28.8 | 0.942 |
| Niacin equivalents
(μg) | 28.3±2.0 | 29.5±3.1 | 0.584 |
| Retinol
equivalents (mg) | 839±95 | 1039±152 | 0.199 |
| Riboflavin
(mg) | 1.5±0.2 | 1.7±0.3 | 0.513 |
| Thiamin (mg) | 1.3±0.1 | 1.2±0.2 | 0.727 |
| Vitamin
B6 (mg) | 1.4±0.1 | 1.3±0.1 | 0.478 |
| Vitamin
B12 (μg) | 4.5±0.5 | 6.1±1.1 | 0.042a |
| Vitamin C
(mg) | 124.6±18.3 | 126.1±16.6 | 0.913 |
| Vitamin D
(μg) | 2.9±0.4 | 3.8±0.5 | 0.079 |
| Vitamin E
(mg) | 10.2±0.9 | 10.1±0.9 | 0.941 |
| Minerals |
| Calcium (mg) | 773±85 | 884±186 | 0.373 |
| Copper (mg) | 1.2±0.1 | 1.1±0.1 | 0.383 |
| Iron (mg) | 9.7±0.7 | 8.9±0.9 | 0.412 |
| Magnesium
(mg) | 358±28.3 | 333.5±42.8 | 0.500 |
| Phosphorus
(mg) | 1455±110 | 1475±213 | 0.901 |
| Potassium
(mg) | 3577±281 | 3454±400 | 0.686 |
| Selenium (μg) | 50.1±3.7 | 54.6±5.9 | 0.316 |
| Sodium (mg) | 2694±209 | 2618±276 | 0.754 |
| Zinc (mg) | 9.6±0.7 | 9.5±1.2 | 0.925 |
| Table VIDaily intake of various vegetables,
fruits and berries in patients with irritable bowel syndrome (IBS)
before and following dietary guidance sessions. |
Table VI
Daily intake of various vegetables,
fruits and berries in patients with irritable bowel syndrome (IBS)
before and following dietary guidance sessions.
| Daily intake
(g) | |
|---|
|
| |
|---|
|
Vegetables/fruits/berries | Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| Cauliflower:
raw | 1.4±0.9 | 0.7±0.6 | 0.300 |
| Cauliflower:
cooked | 4.9±2.0 | 4.9±2.8 | 0.996 |
| Broccoli: raw | 1.5±1.0 | 1.2±1.0 | 0.821 |
| Broccoli:
cooked | 5.2±1.4 | 5.4±2.2 | 0.909 |
| Peas | 2.1±0.5 | 0.4±0.2 | 0.006b |
| Cabbage: raw | 1.5±1.0 | 0.1±0.1 | 0.193 |
| Cabbage:
cooked | 2.3±0.7 | 0.2±0.2 | 0.010a |
| Paprika: raw | 4.9±1.4 | 1.8±1.3 | 0.006b |
| Paprika:
cooked | 3.3±0.9 | 0.7±0.3 | 0.019a |
| Onion, leak or
garlic | 11.5±2.9 | 1.7±0.8 | 0.003b |
| Tomatoes | 5.7±1.6 | 11.2±3.4 | 0.102 |
| Potatoes:
fried | 5.5±1.2 | 7.6±1.3 | 0.070 |
| Potatoes: cooked,
mashed or gratin | 63.7±9.8 | 61.1±8.5 | 0.770 |
| Oranges | 44.5±17.4 | 47.5±17.2 | 0.884 |
| Bananas | 24.1±8.0 | 4.7±1.6 | 0.023a |
| Grapes | 16.2±5.0 | 2.6±1.4 | 0.016a |
| Pears | 16.5±6.3 | 4.5±2.4 | 0.059 |
| Apples | 29.3±8.0 | 34.7±13.6 | 0.688 |
| Peaches | 8.9±3.2 | 6.7±3.1 | 0.553 |
| Grapefruit | 1.4±0.9 | 0.6±0.3 | 0.421 |
| Mangos | 4.3±2.1 | 4.9±3.3 | 0.885 |
| Plums | 2.3±0.9 | 4.4±2.9 | 0.497 |
| Melons | 4.9±1.4 | 4.5±1.7 | 0.692 |
| Blueberries | 6.9±2.1 | 6.5±2.1 | 0.879 |
| Strawberries | 12.2±3.0 | 12.2±5.1 | 0.992 |
| Prunes: dried | 0.3±0.1 | 0.7±0.3 | 0.188 |
| Apricots:
dried | 0.5±0.3 | 0.9±0.4 | 0.329 |
| Mushrooms | 1.7±0.3 | 1.4±0.4 | 0.513 |
| Green beans | 0.3±0.2 | 0.3±0.2 | 1.000 |
| Table VIIDaily intake of patients with
irritable bowel syndrome (IBS), demonstrating the replacement of
wheat products with spelt products following dietaryguidance
sessions. |
Table VII
Daily intake of patients with
irritable bowel syndrome (IBS), demonstrating the replacement of
wheat products with spelt products following dietaryguidance
sessions.
| Daily intake
(g) | |
|---|
|
| |
|---|
| Wheat/spelt
products | Before dietary
guidance | Following dietary
guidance | P-value |
|---|
| White bread | 3.4±1.7 | 4.4±1.7 | 0.636 |
| Dark bread | 85.4±27.3 | 48.0±21.5 | 0.319 |
| Spaghetti and other
pasta | 15.1±2.0 | 13.4±1.6 | 0.456 |
| Waffles or
pancakes | 10.1±2.0 | 7.1±1.3 | 0.103 |
| Chocolate
cakes | 5.1±0.8 | 2.8±0.7 | 0.002b |
| Crisp bread | 15.4±7.2 | 17.2±6.3 | 0.723 |
| Sweet buns | 4.7±1.5 | 1.1±0.3 | 0.025a |
Discussion
There was a high incompletion rate in this study,
with a completion rate of only 37%, and a rate of abandonment of
39%. This was within the limits (30–40%) of comparative studies
(18,29). The low number of patients
completing the study was due to several factors; 4% due to
non-compliance and collaboration problems leading to exclusion; 9%
due to a marked improvement in symptoms following the dietary
guidance leading to a lack of motivation to continue with the
study; 7% due to the diagnosis of an organic disease during the
study; and 4% due to pregnancy and moving abroad.
A previous study demonstrated that although patients
with IBS purposely avoided certain food items that were rich in
FODMAPs, they unknowingly maintained a high FODMAP intake due to
the consumption of alternative FODMAP-rich sources (18). It has also been reported that
patients with IBS avoid certain food items, such as milk and dairy
products, unnecessarily, which results in a low intake of certain
vitamins and minerals (15,16,18,20).
It is therefore apparent that patients with IBS require guidance to
appropriately manage their diet.
The question of how dietary guidance should be
provided, and what should it contain, remains unanswered.
Individual guidance has been demonstrated to be effective in
reducing the symptoms and improving the quality of life of patients
with IBS (18), in comparison with
guidance provided in a group situation (i.e., an IBS school), which
has been demonstrated to be less effective (30–32).
As discussed previously (20), the
common dietary advice given to patients with IBS to reduce symptoms
is unmanageable in daily life, and raises the risk of inadequate
nutrient intake, particularly of vitamins and minerals. Dietary
advice should be simple and easy to apply. In the present study,
the patients were advised to avoid a small number of food items
that were richest in FODMAPs and insoluble fibers, such as onions,
garlic, paprika, beans and peas. In addition, they were advised to
avoid foods containing artificial sweeteners and carbonated
beverages.
In the present study, the replacement of wheat and
wheat products with spelt and spelt products, respectively, enabled
the patients with IBS to continue to consume food items, such as
bread, without a drastic change to their lifestyle. Spelt is known
to contain fewer galactans and fructans (both of which are FODMAPs)
than wheat. This observation challenges the emerging concept that
gluten has a role in the development of symptoms in IBS (33).
The present results demonstrate that three sessions
of dietary guidance, each lasting 45 min and provided by a nurse,
may reduce the symptoms and improve the quality of life of patients
with IBS, as well improving their vitamin and mineral intake. This
effect has been demonstrated to be long-term (18). This indicates that dietary guidance
may be used as a cost-effective option for the management of IBS;
combining dietary guidance with other lifestyle measures, such as a
regular intake of probiotics and regular exercise, would augment
the effect of dietary management (34). Food supplements with beneficial
bacteria, including Lactobacillus spp. and
Bifidobacterium spp., would increase the tolerance to both
FODMAPs and fibers, since they do not produce gas on fermenting
carbohydrates (1). In addition,
physical activity has been found to increase gastrointestinal
transit (35,36).
References
|
1
|
El-Salhy M, Gundersen D, Hatlebakk JG and
Hausken T: Irritable bowel syndrome. Nova Science Publishers; New
York, NY: 2012
|
|
2
|
Thompson WG: A world view of IBS.
Irritable Bowel Syndrome: Diagnosis and Treatment. Camilleri M and
Spiller RC: WB Saunders; Edinburgh: pp. 17–26. 2002
|
|
3
|
Agréus L, Svärdsudd K, Nyrén O and Tibblin
G: Irritable bowel syndrome and dyspepsia in the general
population: overlap and lack of stability over time.
Gastroenterology. 109:671–680. 1995.PubMed/NCBI
|
|
4
|
Thompson WG and Heaton KW: Functional
bowel disorders in apparently healthy people. Gastorenterology.
79:283–288. 1980.PubMed/NCBI
|
|
5
|
Kennedy TM, Jones RH, Hungin AP,
O’Flanagan H and Kelly P: Irritable bowel syndrome,
gastro-oesophageal reflux, and bronchial hyper-responsiveness in
the general population. Gut. 43:770–774. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Drossman DA, Li Z, Andruzzi E, Temple RD,
Talley NJ, Thompson WG, Whitehead WE, Janssens J, et al: U.S.
householder survey of functional gastrointestinal disorders.
Prevalence, sociodemography, and health impact. Dig Dis Sci.
38:1569–1580. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Talley NJ, Gabriel SE, Harmsen WS,
Zinsmeister AR and Evans RW: Medical costs in community subjects
with irritable bowel syndrome. Gastroenterology. 109:1736–1741.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hungin AP, Whorwell PJ, Tack J and Mearin
F: The prevalence, patterns and impact of irritable bowel syndrome:
an international survey of 40,000 subjects. Aliment Pharmacol Ther.
17:643–650. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jones R and Lydeard S: Irritable bowel
syndrome in the general population. BMJ. 304:87–90. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bordie AK: Functional disorders of the
colon. J Indian Med Assoc. 58:451–456. 1972.PubMed/NCBI
|
|
11
|
O’Keefe EA, Talley NJ, Zinsmeister AR and
Jacobsen SJ: Bowel disorders impair functional status and quality
of life in the elderly: a population-based study. J Gerontol A Biol
Sci Med Sci. 50:M184–M189. 1995.PubMed/NCBI
|
|
12
|
Everhart JE and Renault PF: Irritable
bowel syndrome in office-based practice in the United States.
Gastroenterology. 100:998–1005. 1991.PubMed/NCBI
|
|
13
|
Wilson S, Roberts L, Roalfe A, Bridge P
and Singh S: Prevalence of irritable bowel syndrome: a community
survey. Br J Gen Pract. 54:495–502. 2004.PubMed/NCBI
|
|
14
|
Harvey RF, Salih SY and Read AE: Organic
and functional disorders in 2000 gastroenterology outpatients.
Lancet. 1:632–634. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Simrén M, Månsson A, Langkilde AM,
Svedlund J, Abrahamsson H, Bengtsson U and Björnsson ES:
Food-related gastrointestinal symptoms in the irritable bowel
syndrome. Digestion. 63:108–115. 2001.PubMed/NCBI
|
|
16
|
Williams EA, Nai X and Corfe BM: Dietary
intakes in people with irritable bowel syndrome. BMC Gastroenterol.
11:92011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nanda R, James R, Smith H, Dudley CR and
Jewell DP: Food intolerance and the irritable bowel syndrome. Gut.
30:1099–1104. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ostgaard H, Hausken T, Gundersen D and
El-Salhy M: Diet and effects of diet management on quality of life
and symptoms in patients with irritable bowel syndrome. Mol Med
Rep. 5:1382–1390. 2012.PubMed/NCBI
|
|
19
|
El-Salhy M, Ostgaard H, Gundersen D,
Hatlebakk JG and Hausken T: The role of diet in the pathogenesis
and management of irritable bowel syndrome (Review). Int J Mol Med.
29:723–731. 2012.PubMed/NCBI
|
|
20
|
Böhn L, Störsrud S and Simrén M: Nutrient
intake in patients with irritable bowel syndrome compared with the
general population. Neurogastroenterol Motil. 25:23–30.
2013.PubMed/NCBI
|
|
21
|
Ligaarden SC, Lydersen S and Farup PG:
Diet in subjects with irritable bowel syndrome: a cross-sectional
study in the general population. BMC Gastroenterol. 12:612012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Roalfe AK, Roberts LM and Wilson S:
Evaluation of the Birmingham IBS symptom questionnaire. BMC
Gastroenterol. 8:302008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Patrick DL, Drossman DA, Frederick IO,
DiCesare J and Puder KL: Quality of life in persons with irritable
bowel syndrome: development and validation of a new measure. Dig
Dis Sci. 43:400–411. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Drossman DA, Patrick DL, Whitehead WE,
Toner BB, Diament NE, Hu Y, Jia H and Bangdiwala SI: Further
validation of the IBS-QOL: a disease-specific quality-of-life
questionnaire. Am J Gastroenterol. 95:999–1007. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Talley NJ, Verlinden M and Jones M:
Quality of life in functional dyspepsia: responsiveness of the
Nepean Dyspepsia Index and development of a new 10-item short form.
Aliment Pharmacol Ther. 15:207–216. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Arslan G, Lind R, Olafsson S, Florvaag E
and Berstad A: Quality of life in patients with subjective food
hypersensitivity: applicability of the 10-item short form of the
Nepean Dyspepsia Index. Dig Dis Sci. 49:680–687. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Masson LF, McNeill G, Tomany JO, Simpson
JA, Peace HS, Wei L, Grubb DA and Bolton-Smith C: Statistical
approaches for assessing the relative validity of a food-frequency
questionnaire: use of correlation coefficients and the kappa
statistic. Public Health Nutr. 6:313–321. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Brantsaeter AL, Haugen M, Alexander J and
Meltzer HM: Validity of a new food frequency questionnaire for
pregnant women in the Norwegian Mother and Child Cohort Study
(MoBa). Matern Child Nutr. 4:28–43. 2008. View Article : Google Scholar
|
|
29
|
Enck P, Klosterhalfen S and Kruis W:
Determination of placebo effect in irritable bowel syndrome. Dtsch
Med Wochenschr. 130:1934–1937. 2005.(In German).
|
|
30
|
Ringström G, Störsrud S, Lundqvist S,
Westman B and Simrén M: Development of an educational intervention
for patients with Irritable Bowel Syndrome (IBS): a pilot study.
BMC Gastroenterol. 9:102009.PubMed/NCBI
|
|
31
|
Ringström G, Störsrud S, Posserud I,
Lundqvist S, Westman B and Simrén M: Structured patient education
is superior to written information in the management of patients
with irritable bowel syndrome: a randomized controlled study. Eur J
Gastroenterol Hepatol. 22:420–428. 2010.PubMed/NCBI
|
|
32
|
Ringström G, Störsrud S and Simrén M: A
comparison of a short nurse-based and a long multidisciplinary
version of structured patient education in irritable bowel
syndrome. Eur J Gastroenterol Hepatol. 24:950–957. 2012.PubMed/NCBI
|
|
33
|
Aziz I and Sanders DS: Emerging concepts:
from coeliac disease to non-coeliac gluten sensitivity. Proc Nutr
Soc. 71:576–580. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
El-Salhy M, Lillebø E, Reinemo A, Salmelid
L and Hausken T: Effects of a health program comprising
reassurance, diet management, probiotics administration and regular
exercise on symptoms and quality of life in patients with irritable
bowel syndrome. Gastroenterol Insights. 2:21–26. 2010. View Article : Google Scholar
|
|
35
|
Strid H, Simrén M, Störsrud S, Stotzer PO
and Sadik R: Effect of heavy exercise on gastrointestinal transit
in endurance athletes. Scand J Gastroenterol. 46:673–677. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Huang W, Huang X, Xing Z, Qiu X, Wang Y,
Fan R, Liu W, et al: Meranzin hydrate induces similar effect to
Fructus Aurantii on intestinal motility through activation of H1
histamine receptors. J Gastrointest Surg. 15:87–96. 2011.
View Article : Google Scholar : PubMed/NCBI
|