Introduction
Kawasaki disease (KD), also known as mucocutaneous
lymph node syndrome, is an idiopathic acute vasculitis condition,
which primarily occurs in infants and younger children, and
clinically mimics febrile diseases (1). At present, the differential diagnosis
of KD and other febrile diseases is primarily dependent on clinical
symptoms, such as persistent fever for >5 days, skin rashes,
purulent lymphadenitis and enlargement of lymph nodes of the neck,
conjunctival hyperemia, diffuse hyperemia of the oral mucosa,
palmoplantar erythema, and edema of the hands and feet (2). These clinical symptoms lack the
required specificity to accurately differentiate KD from febrile
diseases, often resulting in the misdiagnosis of KD. Thus, 15–25%
of patients with KD are incorrectly diagnosed and receive
inadequate treatment during the window of opportunity for
successful treatment; consequently, the disease may progress to
different degrees of coronary artery damage, and may even result in
acquired heart disease (3).
Notably, KD is becoming one of the primary causes of pediatric
acquired heart disease (4,5). Therefore, there is an urgent
requirement to identify novel differential diagnostic markers of
KD.
It has previously been demonstrated that KD may be
associated with certain immune factors, and the occurrence of KD
may be associated with susceptibility genes and associated
infections (6). Notably, these
susceptibility genes may serve an important role in the onset and
development of KD due to an imbalance in the immune system induced
by subsequent infections (7). In
the earlier phases of KD, the presence of cytokines and chemokines,
which are associated with the innate immune response, are part of
the defense against foreign pathogens (8), and infiltration of immunoglobulin
(Ig)A antibodies and microtubule organization activate the
lymphocyte immune response to specific antigens (9). In our previous study, it was
demonstrated that there was a quantity of autoantibodies present in
the peripheral circulation of patients with KD, including
anti-phosphoglycerate kinase 1 (PGK1) antibodies in the serum of
patients (10). The aim of the
present study was to identify specific diagnostic markers present
in the serum of patients with KD, which may be used for
differentiating KD from other diseases during the earlier stages.
Immunoproteomic methods were used to identify KD-associated markers
and investigate their diagnostic value.
Materials and methods
Patients
The present study was approved by the Medical Ethics
Committee of Beijing Children's Hospital (approval no. 2012-23),
and written informed consent for treatment and clinical
examinations was obtained from all guardians of the children
recruited. A total of 126 subjects collected from Beijing
Children's Hospital participated in the present study, including 50
patients with KD, 38 non-KD febrile controls (FCs) and 38
age-matched healthy controls (HCs). Serum samples were collected
between November 2013 and June 2016 at Beijing Children's Hospital;
serum samples were collected by centrifugation (8,000 × g for 5 min
at 4°C) of ≥1 ml blood samples. The clinicopathological
characteristics of patients with KD, and FCs and HCs are presented
in Table SI, and the comparisons
of clinicopathological characteristics of patients with KD, and FCs
and HCs are presented in Table I.
Diagnostic criteria met the fifth edition of the Research Committee
of KD diagnostic criteria (11);
the FC group consisted of patients with fever for >3 days that
clinically mimicked KD.
 | Table I.Clinicopathological variables of
patients with KD, and FCs and HCs. |
Table I.
Clinicopathological variables of
patients with KD, and FCs and HCs.
|
|
|
|
| P-value |
|---|
|
|
|
|
|
|
|---|
| Variable | KD (n=50) | FC (n=38) | HC (n=38) | KD vs. FC | KD vs. HC |
|---|
| Sex
(female/male) | 22/28 | 16/22 | 10/28 | 0.8589 | 0.0876 |
| Age
(years)a | 2.5±2.2 | 2.7±1.9 | 3.3±1.8 | 0.8467 | 0.1734 |
| Coronary artery
lesions (−/+) | 11/39 |
|
|
|
|
| Neutrophil
granulocyte %a | 52.6±23.3 | 47.5±20.4 |
| 0.2852 |
|
| C-reactive protein
(mg/l)a | 55.8±53.8 | 27.7±28.4 |
| 0.0022 |
|
| Erythrocyte
sedimentation rate (mm/h)a | 61.5±30.0 | 36.2±23.6 |
| <0.0001 |
|
| White blood cell
(109/l)a | 11.1±4.8 | 10.8±4.4 |
| 0.7679 |
|
| Red blood cell
(1012/l)a | 4.0±0.3 | 4.3±0.5 |
| 0.0074 |
|
| Hemoglobin
(g/l)a | 104.8±10.2 | 110.4±14.0 |
| 0.0310 |
|
| Blood platelets
(109/l)a | 397.9±144.4 | 386.4±218.2 |
| 0.7787 |
|
Cell culture and indirect
immunofluorescence assays
HeLa cells (National Infrastructure of Cell Line
Resource) were plated on a sterile glass slide to generate HeLa
cell chips, and were cultured in high-glucose DMEM (HyClone; GE
Healthcare Life Sciences), supplemented with 10% FBS (Hangzhou
Sijiqing Biological Engineering Materials Co., Ltd.) in a 37°C
incubator containing 5% CO2. The slides were fixed with
4% paraformaldehyde for 10 min at room temperature, permeabilized
with 0.2% Triton X-100 for 10 min at room temperature and blocked
with 5% goat serum (Hangzhou Sijiqing Biological Engineering
Materials Co., Ltd.) for 2 h at 37°C. Subsequently, slides were
incubated with serum (diluted 1:20 in PBS) obtained from patients
in the KD, FC and HC groups, and incubated at 37°C for 1 h. For the
positive control, serum samples were replaced with an anti-β-actin
(ACTB) antibody (1:100; cat. no. 60008-1-Ig; Wuhan Sanying
Biotechnology); for the negative control, serum samples were
replaced with PBS. The HeLa cell chips were washed with PBS-0.3%
Tween-20 (PBST) three times, then incubated with FITC-conjugated
goat-anti human IgG antibodies (1:100; cat. no. bs-0297G-FITC;
BIOSS) at 37°C for 1 h. Cell nuclei were counterstained with DAPI
(Beyotime Institute of Biotechnology) for 5 min at room
temperature. Images of cell chips were captured using an Olympus
FV1000 confocal laser-scanning microscope (Olympus Corporation;
magnification, ×40). Semi-quantitative analysis of the fluorescence
intensity of the HeLa cell chips was conducted using ImageJ version
1.51n software (National Institutes of Health). To obtain the
average fluorescence density of each cell, the fluorescence density
of all the cells in the entire image were analyzed.
Western blotting of HeLa cell
extracts
Total protein was extracted from HeLa cells using
RIPA lysis buffer (Beyotime Institute of Biotechnology), containing
1 mM phenylmethylsulfonyl fluoride and 1% protease inhibitors.
Total protein was quantified using the BCA Protein Assay kit (cat.
no. C05-02001; BIOSS) and proteins (30 µg/lane) were separated by
SDS-PAGE on a 12% gel. The separated proteins were transferred onto
PVDF membranes and subsequently blocked with 5% skimmed milk for 1
h at 37°C. Serum samples from the KD, FC and HC groups (1:100) were
used as the probe antibodies and were incubated with the PVDF
membrane for 12 h at 4°C. After the incubation, the PVDF membranes
were washed with 0.3% PBST three times (10 min/wash) and incubated
with goat horseradish peroxidase (HRP)-conjugated anti-human IgG
secondary antibody (1:10,000; cat. no. bs-0297G-HRP; BIOSS) at 37°C
for 1 h. Protein bands were visualized using an enhanced
chemiluminescence reagent (Applygen Technologies, Inc.) and
recovered for mass spectrometry.
In-gel digestion, mass spectrometry
and protein identification
In-gel digestion and mass spectrometry were
performed as previously described (12). Briefly, gel pieces containing the
target protein band were excised from the SDS-PAGE gels, washed
with a mixture of 25 mM NH4HCO3 and 50%
acetonitrile for 30 min at 25°C, dehydrated at 8,000 × g for 15 min
at 4°C using vacuum centrifugation, then washed with 25 mM
NH4HCO3 and 10 mM dithiothreitol for 2 h at
37°C. After cooling to room temperature, the gel pieces were washed
with 25 mM NH4HCO3 containing 55 mM
iodoacetamide for 45 min at 25°C in the dark. The target gel pieces
were subsequently washed with 50% acetonitrile in 25 mM
NH4HCO3 for 10 min at 25°C and dehydrated in
a vacuum concentrator at 8,000 × g for 15 min at 4°C. The
dehydrated gel pieces were digested with trypsin and 20 µl 0.05 M
NH4HCO3 (Sigma-Aldrich; Merck KGaA) at 37°C
for 12 h. Finally, peptide fragments of target proteins were
sequenced using an LC-MALDI-TOF/TOF mass spectrometer (Applied
Biosystems; Thermo Fisher Scientific, Inc.); commercial sequencing
services were provided by the Institute of Microbiology, Chinese
Academy of Sciences. Data were analyzed using the Mascot Server
bioinformatics database search engine (Matrix Science, Inc.).
Protein scores >56 were considered significant. Since HeLa cells
are a human cell line, the search species was selected as Homo
sapiens in the Mascot database. A further selection criterion
was that the protein molecular weight was ~70 kDa.
ELISA
Heat shock cognate 71 kDa protein (HSP7C; cat. no.
11329-H07E; Sino Biological, Inc.) was diluted in
carbonate-bicarbonate buffer (0.05 M; pH 9.6) to a final
concentration of 500 ng/ml and used to coat the wells of a 96-well
microplate at 4°C overnight. Subsequently, the wells were blocked
with 10% goat serum at 37°C for 2 h. Serum samples (100 µl)
obtained from the KD (n=50), FC (n=38) and HC (n=38) groups were
diluted 1:100 in 0.1% PBST and added to the microplate as probe
antibodies, and incubated at 37°C for 2 h. Wells were then rinsed
five times with 0.3% PBST, and subsequently a goat HRP-conjugated
anti-human IgG secondary antibody (1:10,000) was added and
incubated at 37°C for 1 h. Wells were rinsed, and 100 µl
tetramethylbenzidine was added and incubated for 5 min at 25°C. The
reaction was terminated with 50 µl 2 M H2SO4.
The optical density (OD) value of each well was detected using a
microplate reader at a detection wavelength of 450 nm and a
reference wavelength of 620 nm.
Statistical analysis
SPSS version 17.0 software (SPSS, Chicago, IL) and
GraphPad Prism version 7.0 software (GraphPad Software Inc.) were
used to perform statistical analysis. Continuous data are presented
as the mean ± SD and experiments were repeated two times. To
compare clinicopathological variables when the variances between
the two groups were equal, a Student's t-test was used; a
Cox-Cochran test was used for unequal variances; and a
χ2 test was used to analyze categorical data. When three
groups were compared, one-way ANOVA followed by the Sidak's
multiple comparison test was conducted. To determine statistical
differences between the three groups analyzed by ELISA, a
Kruskal-Wallis test followed by a Dunn's post hoc multiple
comparisons test was used. The receiver operating characteristic
(ROC) analysis was performed using MedCalc version 9.2.0.1 software
(MedCalc Software) and OD values corresponding to the highest
Youden index were used as the cut-off values (13). P<0.05 was considered to indicate
a statistically significant difference.
Results
Antigens in HeLa cells can be
recognized by KD serum
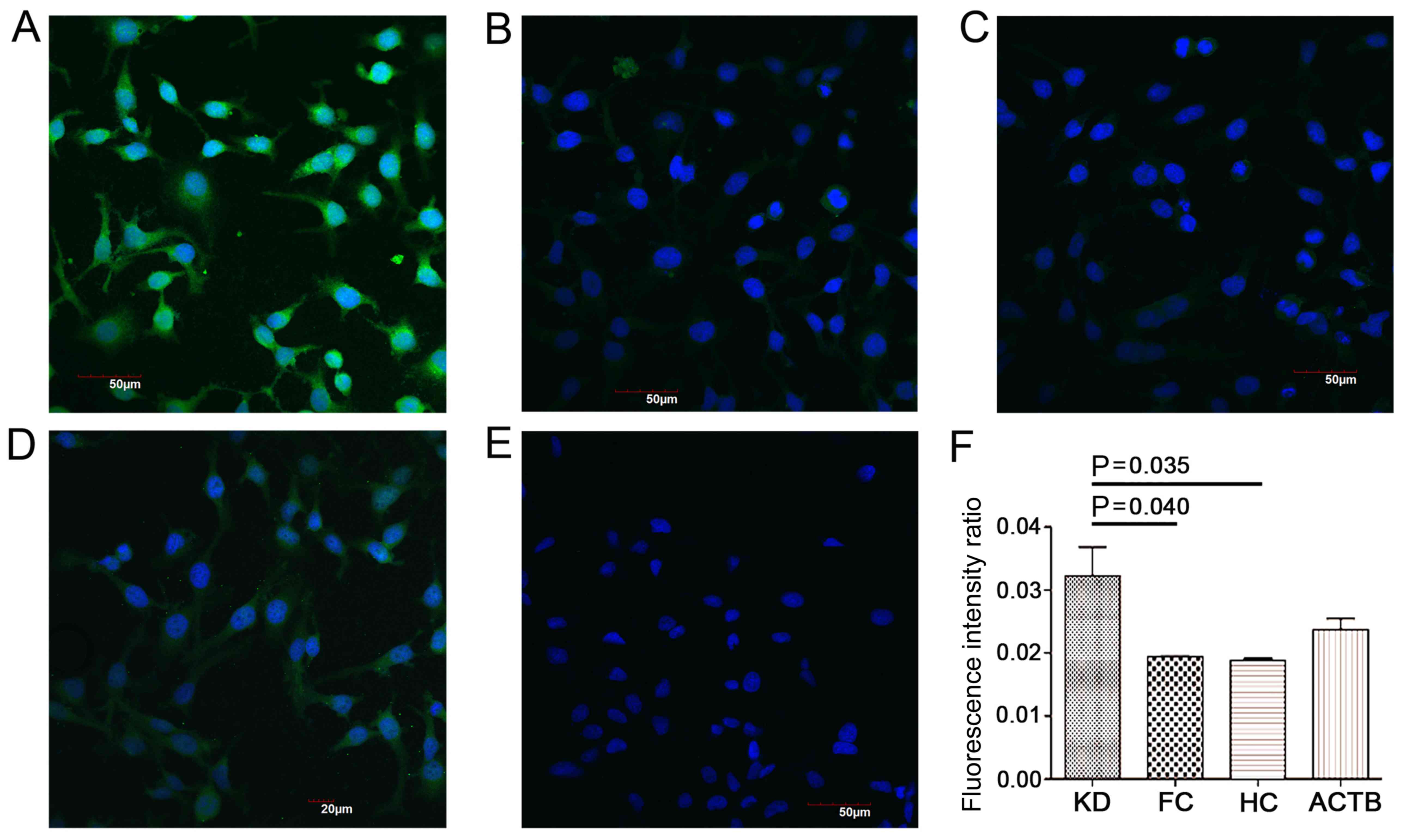
HeLa cell chips were produced and used for the
indirect immunofluorescence assay, in which serum samples
containing the probe antibodies were incubated with the cell chips,
and anti-ACTB antibody was used as the positive control.
Significantly increased fluorescence intensities were observed in
the cells incubated with sera from the KD group compared with sera
from the FC and HC groups (Fig. 1;
P<0.05). These results suggested that certain antigens in the
HeLa cells could be probed using antibodies present in the serum of
patients with KD.
Identification of a novel antibody
present in the serum of patients with KD
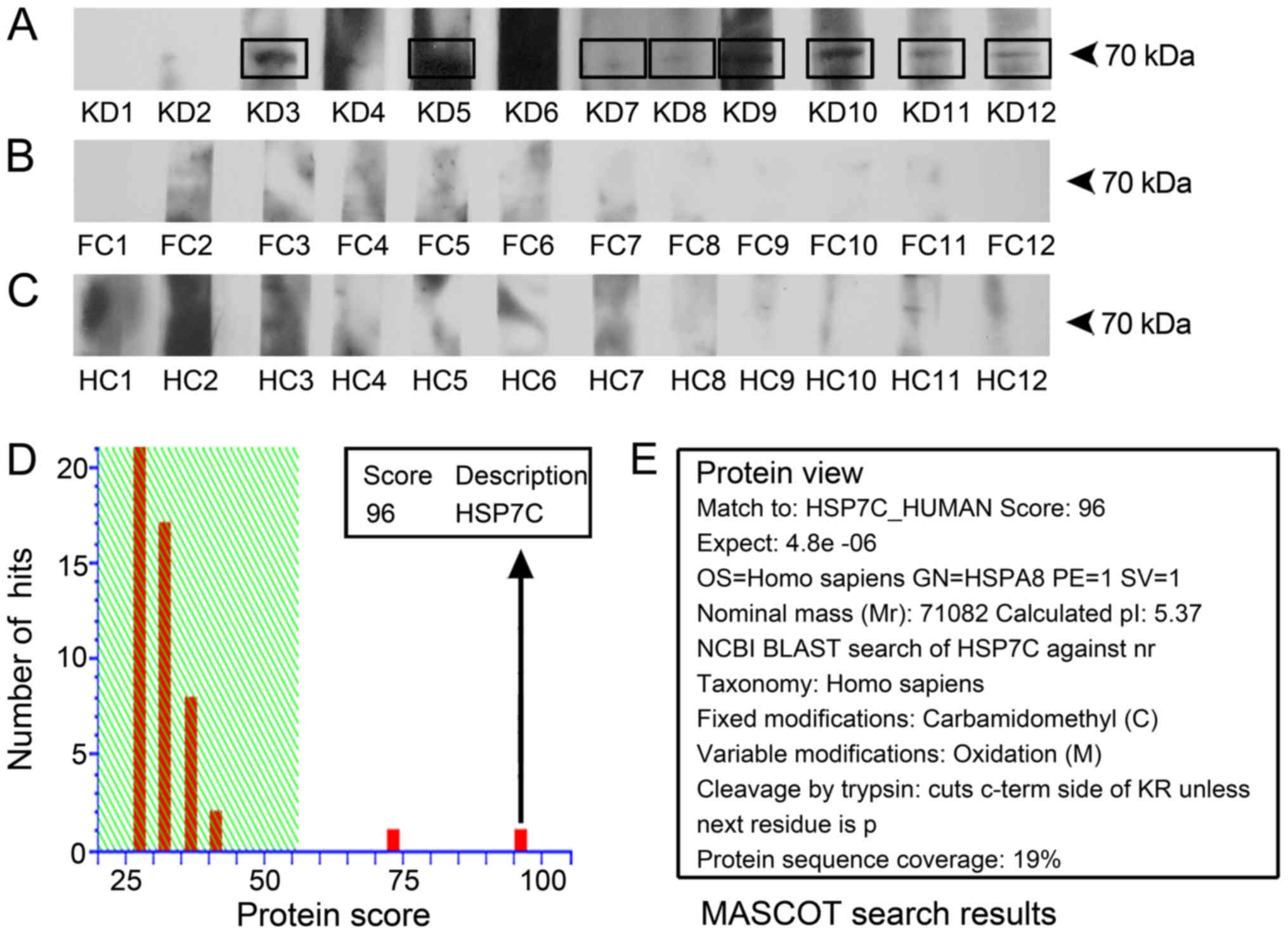
Whole extracts of HeLa cells were used as human
antigen sources, and western blotting was performed to identify
target antigens of antibodies present in the serum of patients with
KD. As a result, eight out of 12 KD serum samples probed an antigen
with a molecular weight of ~70 kDa, which was absent from cells
incubated with serum from the FC and HC groups (Fig. 2A-C). The results suggested that
this 70-kDa protein reacted with antibodies present in the serum
samples of patients with KD. The protein band at 70 kDa was
isolated from the gels and identified using mass spectrometry
(Fig. 2D). The amino acid sequence
of the target protein shared 19% protein sequence coverage with
HSP7C, whose gene name is HSPA8 (Fig.
2D and E); and HSP7C demonstrated the highest score of 96 in
the Mascot database. Therefore, further verification was performed
to confirm the presence of anti-HSP7C antibodies in the serum of
patients with KD.
Anti-HSP7C antibodies are present in
the serum of patients with KD
A total of 126 serum samples from the KD, FC and HC
groups were used to investigate the presence of anti-HSP7C
antibodies in the peripheral blood using ELISA. The OD values of
the KD, FC and HC group were 0.285±0.096, 0.233±0.087 and
0.189±0.049, respectively (data not shown). The performance of the
clinical differential diagnosis value of HSP7C was analyzed using a
ROC curve, and the cut-off OD value was used as the corresponding
maximization of the Youden index. Serum levels of anti-HSP7C
antibodies could differentiate patients with KD from patients in
the FC group, with an area under the curve (AUC) of 0.691 (95% CI,
0.584–0.785; P=0.0006), with 60.00% sensitivity and 78.95%
specificity (Fig. 3A). When the
cut-off OD value was set as 0.267, which corresponded to the
highest Youden index value (KD vs. FC), the positive ratio of
anti-HSP7C antibodies in the KD, FC and HC groups were 60.00
(30/50), 21.05 (8/38) and 5.26% (2/38), respectively (Fig. 3C). Serum levels of anti-HSP7C
antibodies could also differentiate the KD group from the HC group
with an AUC of 0.848 (95% CI, 0.756–0.916; P=0.0001), with 60.00%
sensitivity and 97.37% specificity (Fig. 3B). Further analysis demonstrated
that the expression levels of anti-HSP7C antibodies in the KD group
were significantly increased compared with the levels in the serum
from the FC and HC groups (Fig.
3C). The association between serum anti-HSP7C antibody levels
and clinicopathological characteristics of patients with KD was
analyzed (Table II). Patients
with KD were divided into the following two subgroups: i) Lower
serum expression levels of anti-HSP7C antibodies (ELISA cut-off
value ≤0.267); and ii) higher expression levels of anti-HSP7C
antibodies (ELISA cut-off value >0.267). As shown in Table II, there was a significant
difference (P=0.0094) in the number of platelets (PLTs) between
patients with lower antibody levels (461.6±128.0×109/l)
compared with patients with higher antibody levels
(355.5±140.8×109/l). In addition, serum PLT count has
previously been reported to be elevated in patients with KD
(14), and it has been suggested
that serum PLT count in patients with KD is closely associated with
coronary artery lesion (CAL) (15). In the present study, the blood PLT
count in patients with KD with and without CAL was
426.8±111.7×109/l and 389.8±152.6×109/l,
respectively; this finding was not significantly different (data
not shown).
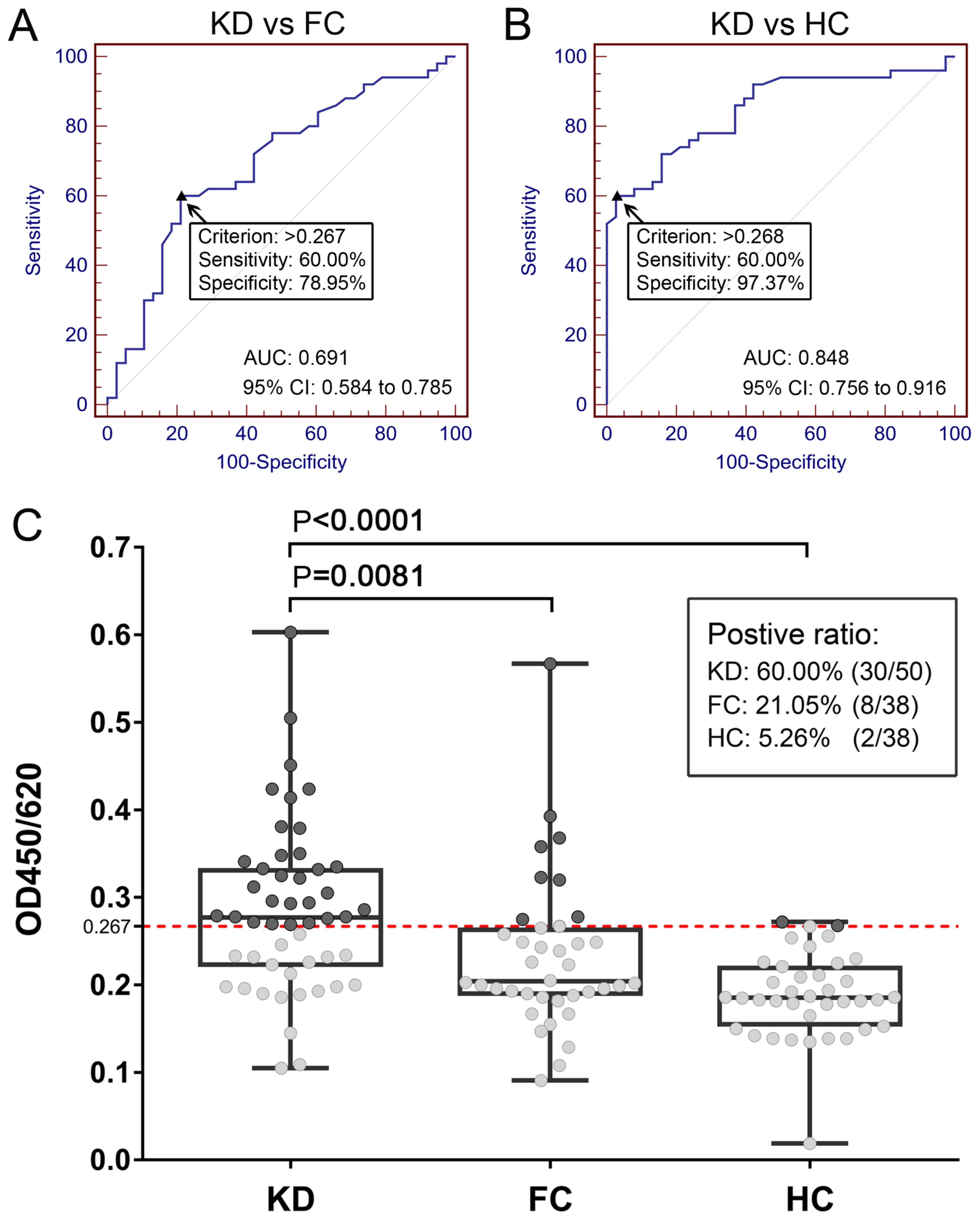 | Figure 3.Diagnostic value of serum anti-HSP7C
antibodies for KD assessed using ELISA. (A) ROC curve analysis of
anti-HSP7C antibody levels in KD and FC groups with an AUC value of
0.691 (95% CI, 0.584–0.785; P=0.0006). (B) ROC curve analysis of
anti-HSP7C antibody levels in the serum samples from the KD and HC
groups with an AUC value of 0.848. (95% CI, 0.756–0.916; P=0.0001).
(C) Scatter plot demonstrating the difference in expression levels
of anti-HSP7C antibodies between the KD, FC and HC groups. The
cut-off value was set at 0.267 (red dotted line; corresponding to
the highest Youden index of KD vs. FC; anti-HSP7C antibodies were
detected in 30/50 KD samples (60.00%), 8/38 FC samples (21.05%) and
2/38 HC samples (5.26%). Levels of anti-HSP7C antibody in the KD
serum samples were significantly increased compared with in the
samples serum from the FC (P=0.0081) and HC (P<0.0001) groups.
Box plots demonstrate the median and the interquartile range, and
the complete range of the data. AUC, area under the curve; FC,
febrile control; HC, healthy control; HSP7C, heat shock cognate 71
kDa protein; KD, Kawasaki disease; OD, optical density; ROC,
receiver operating characteristic. |
| Table II.Clinicopathological variables of
patients with Kawasaki disease categorized according to the serum
anti-HSP7C antibody expression status. |
Table II.
Clinicopathological variables of
patients with Kawasaki disease categorized according to the serum
anti-HSP7C antibody expression status.
| A, Laboratory
variables |
|---|
|
| Serum anti-HSP7C
antibody level |
|
|---|
|
|
|
|
|---|
| Variable | Low (n=20) | High (n=30) | P-value |
|---|
| Sex
(female/male) | 9/11 | 13/17 | 0.9074 |
| Age
(years)a | 2.6±2.2 | 2.4±2.3 | 0.7165 |
| Neutrophil
granulocyte %a | 52.5±24.6 | 52.7±22.9 | 0.9658 |
| C-reactive protein
(mg/l)a | 53.0±60.5 | 57.7±49.8 | 0.7640 |
| Erythrocyte
sedimentation rate (mm/h)a | 63.5±31.4 | 60.2±29.6 | 0.7118 |
| White blood cell
(109/l)a | 11.2±4.4 | 11.0±5.1 | 0.9037 |
| Red blood cell
(1012/l)a | 4.7±0.3 | 3.9±0.3 | 0.1268 |
| Hemoglobin
(g/l)a | 107.3±12.8 | 103.1±7.7 | 0.2018 |
| Blood platelet
(109/l)a | 461.6±128.0 | 355.5±140.8 | 0.0094 |
|
| B, Clinical
variables |
|
| Serum anti-HSP7C
antibody level |
|
|
|
|
|
|
Variable | Low
(n=20) | High
(n=30) | P-value |
|
| Coronary artery
lesions (−/+) | 13/7 | 26/4 | 0.0700 |
| Fever (−/+) | 1/19 | 0/30 | 0.2160 |
| Lymph nodes
(−/+) | 2/18 | 3/27 | >0.9999 |
| Bilateral
conjunctival hyperemia (−/+) | 1/19 | 1/29 | 0.7683 |
| Lips red and
chapped (−/+) | 2/18 | 1/29 | 0.3308 |
| Hard swelling of
hands and feet (−/+) | 5/15 | 8/22 | 0.8953 |
| Torsal polymorphic
erythema (−/+) | 15/5 | 13/17 | 0.0271 |
Discussion
KD is an idiopathic form of acute systemic
vasculitis, the etiology and pathogenesis of which remain unclear.
Previous studies have noted that the pathology of KD is associated
with immune factors (16,17); in particular, the immune system of
patients with KD appears overactive, and neutrophils,
CD8+ T cells, dendritic cells and monocytes have been
reported to contribute to arterial wall lesions in patients with
KD. It has also been reported that the etiology of KD may be
associated with bacterial infection caused by superantigens and
abnormal immune responses (18).
Fujieda et al (19)
described peroxiredoxin 2 (PRDX2) as an immune target of KD and
high serum levels of anti-PRDX2 antibodies were detected in 43.3%
of patients with KD. Another study revealed that
anti-4-trimethylaminobutyraldehyde dehydrogenase antibodies were
also significantly increased in the serum of patients with KD
(20). In our previous study, it
was demonstrated that there was a marked quantity of autoantibodies
present in the peripheral circulation of patients with KD; in 2018,
we reported that serum anti-PGK1 antibodies were detected in 46% of
serum samples obtained from patients with KD, in 13% of serum
samples from the FC group and 2.6% serum samples from the HC group
(10).
In the present study, a novel anti-HSP7C antibody in
the serum of patients with KD was successfully identified. One
interesting finding from the present study was that HeLa cells
could be used as a source of antigens for immune target
identification. HSP7C proteins were identified by western blotting
and confirmed using mass spectrometry. The results of the present
study demonstrated that the serum of patients with KD had a
specific immune response to the HSP7C protein that was
significantly different compared with the FC and HC groups. HSP7C
is a member of a molecular chaperone family, known as heat shock
proteins, which are involved in various cellular processes,
including proteomic stress protection, peptide folding and
transport (21–24). Studies have reported that heat
shock proteins are closely associated with certain diseases
(25–27); for example, HSP60 is associated
with coronary heart disease (28),
and HSP22 overexpression is associated with the progression and
prognosis of gastric cancer (29).
It has been hypothesized that the heat shock protein 65 from
bacteria stimulates the heat shock protein 63 antigen of the host
to participate in host immune system activation, T-cell activation,
the promotion of cytokine cascade amplification reactions, the
identification of host blood vessels and the induction of systemic
vascular damage (30). Therefore,
the production of high levels of anti-HSP7C antibodies in patients
with KD may be accompanied by abnormal activity of HSP7C.
The sera of patients with KD were immunoreactive to
the HSP7C protein; therefore, autoimmunity to HSP7C in patients
with KD was investigated. The presence of the anti-HSP7C antibody
was analyzed using ELISA, and 60% of patients with KD presented
with upregulated serum levels of anti-HSP7C antibodies, whereas
only 21.05 and 5.26% of patients in the FC and HC groups presented
with upregulated levels of the antibody, respectively. ROC analysis
was performed to determine the classification ability of serum
anti-HSP7C antibody in the KD and FC groups. The AUC was 0.691,
indicating that serum anti-HSP7C could differentiate the KD group
from the FC group. The non-parametric analysis also demonstrated
significant differences in serum levels of anti-HSP7C antibody
between the KD and FC groups, with a P-value of 0.0081. On the
other hand, based on the scatter plot of anti-HSP7C antibody
titers, it was revealed that it was insufficient to use anti-HSP7C
antibody alone as a marker to differentiate KD from FC, as some
patients in the FC group also had positive antibody levels.
Although the positive ratio of the KD group anti-HSP7C antibody was
as high as 60.00% (30/50), whereas in the FC group, only 21.05%
(8/38) individuals were positive. The onset of KD is often
accompanied by a prolonged increase in body temperature. The
clinical symptoms are similar to a common fever (2,5);
thus, patients with fever but without KD (FC) were used as the
disease control. It is reasonable to assume that the expression of
the corresponding antibody may also be increased in patients with
FC; however, the present study reported that the expression levels
of anti-HSP7C antibody were not increased to the same degree as the
patients with KD. In clinical practice, patients are generally
diagnosed through a comprehensive analysis of multiple clinical
indicators, such as fever for >5 days, skin rashes, purulent
lymphadenitis and enlargement of lymph nodes of the neck,
conjunctival hyperemia, diffuse hyperemia of the oral mucosa,
palmoplantar erythema, and edema of the hands and feet (31). Therefore, the anti-HSP7C antibody
may represent an additional diagnostic marker for KD, which could
be used in combination with the other clinical indicators to
improve the diagnosis of KD.
Clinicopathological variables were compared between
patients with higher and lower expression levels of anti-HSP7C
antibody. The presence of anti-HSP7C antibodies was associated with
PLT counts and polymorphic erythema in patients with KD. CAL is a
complication of KD, and studies have reported that the occurrence
of CAL is closely associated with the duration of fever in
patients, which is accompanied by a significant increase in
C-reactive protein, PLT and erythrocyte sedimentation rate counts
(14,32). In the present study, the PLT counts
in patients with KD with and without CAL were
426.8±111.7×109/l and 389.8±152.6×109/l,
respectively. The activation of platelet-derived growth factor, its
receptor and the downstream pathways have previously been observed
to be involved in the formation of CAL in patients with KD, whereas
intravenous immunoglobulin inhibited this activation (33). In the present study, there was a
significant difference in the PLT counts between patients with
lower levels of HSP7C antibody (461.6±128.0×109/l) and
patients with higher levels (355.5±140.8×109/l). The PLT
counts in patients with KD exhibited the opposite trend compared
with anti-HSP7C antibody levels.
To the best of our knowledge, the present study is
the first to demonstrate a potential involvement of anti-HSP7C
antibodies in patients with KD, suggesting that anti-HSP7C
antibodies may be used as an auxiliary diagnostic marker for
identifying and diagnosing patients with KD. However, the present
study has certain limitations and investigating the presence of
anti-HSP7C antibodies in patients with KD will require further
studies; for example, in this study, antibody levels varied widely
among patients with KD; therefore, it was hypothesized that
different subtypes of KD may exist. In the future, a larger cohort
and additional clinical data of patients with KD will need to be
collected to further analyze the differences between patients with
KD with increased levels of anti-HSP7C antibody compared with other
patients with KD, in order to determine why the anti-HSP7C antibody
is only upregulated in a portion of patients with KD. Furthermore,
serum samples from the HC group should be collected for KD-related
blood tests to help further analyze the differences in clinical
indicators between patients with KD and HCs. Studies should also
investigate the mechanism underlying the production of anti-HSP7C
antibodies in patients with KD and determine whether patients with
KD may exhibit any antibodies against antigens from exogenous
pathogens, as more attention must be directed towards the antigens
derived from other species related to KD.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural
Science Foundation of China (grant nos. 81571592 and 31371203) and
the Hebei Provincial Department of Science and Technology (grant
nos. 17277787D and 19942410G).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HD, YW and ZD designed the study. YZ, JC and HH
collected and analyzed the data. JC drafted the manuscript and YZ
revised the paper. All authors have read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Medical Ethics
Committee of Beijing Children's Hospital (approval no. 2012-23),
and written informed consent for the treatment and clinical
examinations was obtained from all guardians of the children
recruited.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
KD
|
Kawasaki disease
|
|
FC
|
non-KD febrile control
|
|
HSP7C
|
heat shock cognate 71 kDa protein
|
References
|
1
|
Kawasaki T: Acute febrile mucocutaneous
syndrome with lymphoid involvement with specific desquamation of
the fingers and toes in children. Arerugi. 16:178–222. 1967.(In
Japanese). PubMed/NCBI
|
|
2
|
Dajani AS, Taubert KA, Gerber MA, Shulman
ST, Ferrieri P, Freed M, Takahashi M, Bierman FZ, Karchmer AW,
Wilson W, et al: Diagnosis and therapy of Kawasaki disease in
children. Circulation. 87:1776–1780. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kato H, Sugimura T, Akagi T, Sato N,
Hashino K, Maeno Y, Kazue T, Eto G and Yamakawa R: Long-term
consequences of Kawasaki disease. A 10- to 21-year follow-up study
of 594 patients. Circulation. 94:1379–1385. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Benseler SM, McCrindle BW, Silverman ED,
Tyrrell PN, Wong J and Yeung RS: Infections and Kawasaki disease:
Implications for coronary artery outcome. Pediatrics.
116:e760–e766. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Takahashi K, Oharaseki T and Yokouchi Y:
Pathogenesis of Kawasaki disease. Clin Exp Immunol. 164 (Suppl
1):S20–S22. 2011. View Article : Google Scholar
|
|
6
|
Newburger JW, Takahashi M, Gerber MA,
Gewitz MH, Tani LY, Burns JC, Shulman ST, Bolger AF, Ferrieri P,
Baltimore RS, et al: Diagnosis, treatment, and long-term management
of Kawasaki disease: A statement for health professionals from the
Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease,
council on cardiovascular disease in the Young, American Heart
Association. Pediatrics. 114:1708–1733. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Onouchi Y: Genetics of Kawasaki disease:
What we know and don't know. Circ J. 76:1581–1586. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yoshioka T, Matsutani T, Iwagami S,
Toyosaki-Maeda T, Yutsudo T, Tsuruta Y, Suzuki H, Uemura S,
Takeuchi T, Koike M and Suzuki R: Polyclonal expansion of TCRBV2-
and TCRBV6-bearing T cells in patients with Kawasaki disease.
Immunology. 96:465–472. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rowley AH, Eckerley CA, Jäck HM, Shulman
ST and Baker SC: IgA plasma cells in vascular tissue of patients
with Kawasaki syndrome. J Immunol. 159:5946–5955. 1997.PubMed/NCBI
|
|
10
|
Cui J, Zhou Y, Hu H, Zhao L, Du Z and Du
H: PGK1 as an immune target in Kawasaki disease. Clin Exp Immunol.
194:371–379. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Guidelines for diagnosis and management of
cardiovascular sequelae in Kawasaki disease. 2005.
|
|
12
|
Sun S, Ma H, Han G, Wu R, Zou H and Liu Y:
Efficient enrichment and identification of phosphopeptides by
cerium oxide using on-plate matrix-assisted laser
desorption/ionization time-of-flight mass spectrometric analysis.
Rapid Commun Mass Spectrom. 25:1862–1868. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rucker G and Schumacher M: Summary ROC
curve based on a weighted Youden index for selecting an optimal
cutpoint in meta-analysis of diagnostic accuracy. Stat Med.
29:3069–3078. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ruan Y, Ye B and Zhao X: Clinical
characteristics of Kawasaki syndrome and the risk factors for
coronary artery lesions in China. Pediatr Infect Dis J.
32:e397–e402. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu R, Gao F, Huo J and Yi Q: Study on the
relationship between mean platelet volume and platelet distribution
width with coronary artery lesion in children with Kawasaki
disease. Platelets. 23:11–16. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Iemura M, Ishii M, Sugimura T, Akagi T and
Kato H: Long term consequences of regressed coronary aneurysms
after Kawasaki disease: Vascular wall morphology and function.
Heart. 83:307–311. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Newburger JW, Takahashi M and Burns JC:
Kawasaki disease. J Am Coll Cardiol. 67:1738–1749. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Meissner HC and Leung DY: Superantigens,
conventional antigens and the etiology of Kawasaki syndrome.
Pediatr Infect Dis J. 19:91–94. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fujieda M, Karasawa R, Takasugi H,
Yamamoto M, Kataoka K, Yudoh K, Kato T, Ozaki S and Wakiguchi H: A
novel anti-peroxiredoxin autoantibody in patients with Kawasaki
disease. Microbiol Immunol. 56:56–61. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Matsunaga A, Harita Y, Shibagaki Y,
Shimizu N, Shibuya K, Ono H, Kato H, Sekine T, Sakamoto N, Igarashi
T and Hattori S: Identification of 4-Trimethylaminobutyraldehyde
dehydrogenase (TMABA-DH) as a candidate serum autoantibody target
for Kawasaki disease. PLoS One. 10:e01281892015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yamamoto YH, Kimura T, Momohara S,
Takeuchi M, Tani T, Kimata Y, Kadokura H and Kohno K: A novel ER
J-protein DNAJB12 accelerates ER-associated degradation of membrane
proteins including CFTR. Cell Struct Funct. 35:107–116. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sopha P, Kadokura H, Yamamoto YH, Takeuchi
M, Saito M, Tsuru A and Kohno K: A novel mammalian ER-located
J-protein, DNAJB14, can accelerate ERAD of misfolded membrane
proteins. Cell Struct Funct. 37:177–187. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kim CP, Hantouche C, Wong M, Matthes E,
Robert R, Hanrahan JW, Shrier A and Young JC: Hsp70 and DNAJA2
limit CFTR levels through degradation. PLoS One.
14:e2209842019.
|
|
24
|
Li K, Jiang Q, Bai X, Yang YF, Ruan MY and
Cai SQ: Tetrameric assembly of K+ channels requires
ER-located chaperone proteins. Mol Cell. 65:52–65. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Martin CA, Carsons SE, Kowalewski R,
Bernstein D, Valentino M and Santiago-Schwarz F: Aberrant
extracellular and dendritic cell (DC) surface expression of heat
shock protein (hsp)70 in the rheumatoid joint: Possible mechanisms
of hsp/DC-mediated cross-priming. J Immunol. 171:5736–5742. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lenzi C, Palazzuoli A, Giordano N,
Alegente G, Gonnelli C, Campagna MS, Santucci A, Sozzi M,
Papakostas P, Rollo F, et al: H pylori infection and systemic
antibodies to CagA and heat shock protein 60 in patients with
coronary heart disease. World J Gastroenterol. 12:7815–7820. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Li XS, Xu Q, Fu XY and Luo WS: Heat shock
protein 22 overexpression is associated with the progression and
prognosis in gastric cancer. J Cancer Res Clin Oncol.
140:1305–1313. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rothenbacher D, Hoffmeister A, Bode G,
Miller M, Koenig W and Brenner H: Helicobacter pylori heat shock
protein 60 and risk of coronary heart disease: A case control study
with focus on markers of systemic inflammation and lipids.
Atherosclerosis. 156:193–199. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li XS, Xu Q, Fu XY and Luo WS: Heat shock
protein 22 overexpression is associated with the progression and
prognosis in gastric cancer. J Cancer Res Clin Oncol.
140:1305–1313. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sun J and Zhai S: Development of Kawasaki
disease pathogenesis. J App Clin Pediatrics. 22:10372007.
|
|
31
|
Guidelines for diagnosis and management of
cardiovascular Sequelae in Kawasaki disease (JCS 2003). J Cardiol.
43:263–283. 2004.(In Japanese). PubMed/NCBI
|
|
32
|
Zhang W, Li Q, Zhao XD, Tang XM, Wang XG,
Wang M, Wu DQ, Ou Q and Yang XQ: Clinical analysis of 942 cases of
Kawasaki disease. Zhonghua Er Ke Za Zhi. 44:324–328. 2006.(In
Chinese). PubMed/NCBI
|
|
33
|
Ueno K, Nomura Y, Hashiguchi T, Masuda K,
Morita Y, Hazeki D, Eguchi T, Maruyama I and Kawano Y: Platelet
vascular endothelial growth factor is a useful predictor for
prognosis in Kawasaki syndrome. Br J Haematol. 148:285–292. 2010.
View Article : Google Scholar : PubMed/NCBI
|