Introduction
Chronic obstructive pulmonary disease (COPD) is a
disease characterized by persistent airflow limitation (1). According to a report published by the
World Health Organization, COPD will become the 4th leading cause
of disease-related economic burden and the 3rd leading cause of
mortality worldwide by 2030 (2).
Obstructive sleep apnea (OSA) is a systemic disease with a high
incidence and certain potential risks, such as cardiovascular and
metabolic disease. Reports have indicated that OSA affects 17% of
women and 34% of men in the US, and has a similar prevalence in
other countries (3). Previous
studies have reported that OSA is an independent risk factor for
coronary heart disease, congestive heart failure and
cerebrovascular disease (4,5), although the correlation between these
diseases and OSA has not been systematically studied.
David Flenley (6)
was the first to create the term ‘overlap syndrome’ (OS), referring
to the coexistence of COPD with OSA, and some studies have revealed
a decreased survival rate among patients with OS compared with
those with either COPD or OSA alone (7,8).
Clinical studies have reported that vascular endothelial injury
occurs in both COPD and OSA, and endothelial dysfunction is more
severe in patients with OS compared with patients with either
condition alone and is correlated with the severity of the disease
(9,10). Intermittent hypoxia can induce the
production of cytokines, including TNF-α, IL-6 and IL-8, and
adhesion molecules by activating another important transcription
factor, NF-κB to promote the development of inflammatory reactions
and affect the formation of atherosclerosis (11,12),
thereby leading to vascular endothelial dysfunction (13). Therefore, identification of
therapeutic strategies for vascular endothelial injury is crucial
for the treatment of OS. To the best of our knowledge, research on
vascular injury in OS is currently lacking. At present, there are
few effective drugs in clinical treatment of OS (14). Therefore, it is important to conduct
in-depth research on novel therapeutic measures to improve vascular
endothelial injury and dysfunction.
Cell therapy has been used in the study of pulmonary
diseases and the treatment of vascular complications (15). Previous studies have reported that
embryonic stem cells and bone marrow (BM)-derived endothelial
progenitor cells (EPCs) can differentiate into vascular endothelial
cells (VECs) (16). COPD animal
model studies have revealed that allogeneic EPCs transplanted into
the trachea can prevent or delay disease progression by reducing
inflammatory infiltration, relieving VEC apoptosis, increasing
antioxidant activity and inhibiting proteolytic enzyme activity
(17). BM mesenchymal stem cells
(BMSCs) are considered cell transplantation and tissue engineering
seed cells due to their convenience, simple separation, rapid
expansion, high safety, low immunogenicity and multi-directional
differentiation potential (18–20).
BMSCs can quickly migrate from the BM into the peripheral
circulation, mobilize to injury sites and differentiate into EPCs
that further differentiate into VECs to repair the injury (21). MSCs have potential therapeutic roles
in the treatment of obstructive sleep apnea-hypopnea syndrome
(OSAHS) (22) and COPD (23,24).
Previous studies have revealed that BMSCs can differentiate into
alveolar epithelial cells in animals with lung injury and can
repair pathological tissue (25,26).
However, to the best of our knowledge, few studies have been
conducted to evaluate the effect of BMSCs on vascular injury in an
OS rat model. Therefore, the aim of the present study was to
investigate the role of BMSCs on vascular injury in COPD-OSA OS
in vivo.
In the current study, an OS rat model was
constructed using the smoke chamber exposure and intermittent
hypoxia method, and then BMSCs were intravenously injected into
rats. The localization of BMSCs was identified in some major organs
using immunofluorescence assays, and the injured vascular tissues
were collected to determine the damage via hematoxylin and eosin
(H&E) staining, reverse transcription-quantitative (RT-q)PCR
and western blot analysis. Apoptosis of VECs was detected using
TUNEL and immunofluorescence assays. CD31 expression in injured
vessels was detected via the immunohistochemical technique.
Materials and methods
Animal grouping
A total of 24 Sprague-Dawley rats (female; weight,
120±20 g; age, 6 weeks) were purchased from Beijing Vital River
Laboratory Animal Technology Co., Ltd. Rats were maintained in a
clean-grade room under controlled temperature and lighting
conditions with a 12-h light/dark photoperiod at 19–23°C and 40–60%
humidity in the Animal Center of Kunming Medical University. The
diet and drinking water of the rats were not restricted. In total,
five rats were kept per cage. All animal experiments were approved
by the Animals Ethics Committee of The First People's Hospital of
Kunming and the Guide for the Care and Use of Laboratory
Animals.
The OS rat model was established using the cigarette
smoke and intermittent hypoxia exposure method according to our
previous study (27). BMSCs were
isolated from the femur and tibia of 1-week-old Sprague-Dawley rats
(female; weight, 120±20 g). The extraction method of BMSCs in rats
were performed as described previously (27). A total of 24 female rats were
randomly divided into three groups (n=8): Sham, OS model and BMSC.
Rats in the sham group were treated with false smoke and air (~21%
O2) exposure. The OS model was established using the
cigarette smoke and intermittent hypoxia exposure method. The
6-week-old female SD rats were exposed to cigarette smoke every day
at 8:00 to 8:30 a.m. and 5:30 to 6:00 p.m. (15 cigarettes at once,
two times daily), intermittent hypoxia with ~99% nitrogen
(N2) for 30 sec and then exposed to air (~21%
O2) every day for 90 sec at 9:00 to 5:00 p.m. (30 times
per hour, 8 h per day) for 8 weeks. All rats were successfully
established as the OS model. BMSCs were labeled with the enhanced
green fluorescent protein (GFP) lentivirus (cat. no. GM100202-2;
Genomeditech Co., Ltd.) following the manufacturer's instructions.
Following 24 h after cigarette smoke and intermittent hypoxia
exposure, the rats in the model group were injected intravenously
with PBS (50 µl), and those in the BMSC group were injected
intravenously with 50 µl BMSCs (total number of cells,
2×106/rat) using a 1 ml syringe via the tail vein (one
time/week on the 7th day of each week, for a total of four times).
A total of 4 weeks after the last injection, the green fluorescence
of BMSC in different tissues was observed under a confocal
fluorescence microscope with magnification at ×900 (Leica
Microsystems GmbH). Rats were euthanized with an overdose of
anesthetic (sodium pentobarbital 150 mg/kg; intraperitoneal). The
rats had no heartbeat, continued involuntary breathing for 2–3 min
and had no blink reflex, which was considered to indicate
mortality. The descending aorta of aortic tissues were then
collected from the rats.
The OS animal model was considered successfully
established by evaluating lung morphologic analysis, as well as
quantifying the emphysema and lung injury score, based on our
previous study (27). Hypoxia and
certain cardiovascular and cerebrovascular diseases can cause
vascular injury in the large and medium-sized arteries (28), and so the most representative
thoracic aorta (the descending aorta) was the primary research
target. The descending aorta in the thoracic aorta is relatively
thick and straight, and is easy to obtain sections from and to
observe (28); thus, the descending
aorta was used as the experimental tissue. In total, three of the
OS model rats were injected intravenously with the GFP-labeled
BMSCs (2×106/rat) to investigate the location and
differentiation of the transplanted BMSCs, and five of the OS model
rats were injected intravenously with unlabeled BMSCs for
examination with the TUNEL assay. All rats were used to perform
H&E staining and immunocytochemistry assays.
Aorta morphologic analysis
Aortic tissues were fixed in 4% formalin for 24 h at
room temperature, embedded in paraffin, cut into 4-µm-thick
sections and stained with H&E (cat. no. G1120; Beijing Solarbio
Science & Technology Co., Ltd.) for 10 min each at room
temperature. The experiment was conducted according to the
manufacturer's instructions. The tissue sections were examined via
light microscopy at ×400 magnification.
Masson staining
Aortic tissues were fixed in 4% formalin for 24 h at
room temperature, embedded in paraffin, cut into 4-µm-thick
sections and stained with a Masson kit (cat. no. G1340; Beijing
Solarbio Science & Technology Co., Ltd.) for 5 min at room
temperature. The experiment was conducted according to the
manufacturer's instructions. In total, ≥3 200-fold fields of view
were randomly selected for each slice in each group. The tissue
sections were examined using light microscopy at ×200
magnification. The collagen volume fraction (CVF) of the sections
was determined using the ratio of pixel area of blue collagen
fibers to total artery area using Image-Pro Plus 6.0 software
(Media Cybernetics, Inc.).
TUNEL assay
The apoptosis of VECs was performed as previously
described (27) using a TUNEL assay
kit (cat. no. 11684817910; Roche Diagnostics, Inc.). Tissue samples
were fixed in 4% formaldehyde for 24 h at room temperature and
embedded in paraffin. Next, 4-µm-thick paraffin sections were
adhered to slides. Sections were deparaffinized by heating the
slides for 30 min at 60°C. The sections were washed with PBS twice.
The sample was added to 50 µl TUNEL assay solution and incubated at
37°C for 60 min in the dark. Then, the samples were washed with PBS
twice. Sections were counterstained with hematoxylin for 5–10 min
at room temperature to visualize nuclei. The film was sealed via
anti-fluorescence quenching, and the sections were observed under a
confocal microscope with ×400 magnification. In total, three fields
of view were randomly selected. The available excitation wavelength
range was 450–500 nm, and the emission wavelength range was 515–565
nm (green fluorescence). The tissue sections were examined via
confocal microscopy.
Immunofluorescence
The tissue sections were placed in a 65°C incubator
and baked for 15 min. Paraffin sections were incubated at room
temperature in xylene I for 15 min, xylene II for 15 min, ethanol I
for 5 min, anhydrous ethanol II for 5 min, 85% alcohol for 5 min,
75% alcohol for 5 min and distilled water to wash. Then, the
samples were washed with PBS + 0.1% Triton X-100T (PBST) three
times for 5 min each, at room temperature in a shaking bed. Tissue
sections were placed in a repair box filled with EDTA antigen
repair buffer, and antigen repair was conducted for 10 min at 100°C
in the microwave oven. Then, slices were washed with 0.1% PBST
three times, for 5 min each time, at room temperature in a shaking
bed. The tissue was blocked with 5% v/v normal goat serum (cat. no.
SL038; Beijing Solarbio Science & Technology Co., Ltd.) for 30
min at room temperature. Sections were incubated with an anti-CD34
antibody (1:100; cat. no. A10796; ABclonal Biotech Co., Ltd.)
overnight at 4°C and with a CoraLite594-conjugated secondary
antibody (1:100; cat. no. SA00013-4; ProteinTech Group, Inc.) for 2
h at room temperature. Prior to DAPI staining of the nuclei,
sections were washed three with PBS for 5 min each. Then, 10 µg/ml
DAPI dye was added and incubated at room temperature in the dark
for 10 min. Film sealing was performed by washing with PBS three
times. The section was sealed with anti-fluorescence quenching
sealant. Sections were observed using a confocal microscope with
×400 magnification.
Immunocytochemistry
Aortic tissues were fixed in 4% formalin for 24 h at
room temperature, embedded in paraffin and cut into 4-µm-thick
sections. An immunocytochemistry assay was performed according to a
previous described method (27).
The section was blocked with 5% v/v normal goat serum (cat. no.
SL038; Beijing Solarbio Science & Technology Co., Ltd.) for 30
min at room temperature. Sections were incubated with an anti-CD31
antibody (1:100; cat. no. A3181; ABclonal Biotech Co., Ltd.)
overnight at 4°C and then incubated with goat anti-rabbit IgG (H+L)
horseradish peroxidase (HRP)-conjugated secondary antibody (1:200;
cat. no. AS014; ABclonal Biotech Co., Ltd.) for 2 h at room
temperature. The reactions were visualized using a
3,3′-diaminobenzidine visualization kit (Fuzhou Maixin Biotech Co.,
Ltd.) for 10 min at room temperature. Sections were counterstained
with hematoxylin to visualize nuclei, stained with hematoxylin for
5–10 min at room temperature and dehydrated. Sections were examined
under a light microscope at a magnification of ×200. Brown staining
indicated immunoreactive cells, and blue staining indicated the
nuclei. Sections were analyzed using Image-Pro Plus software
(version 6.0; Media Cybernetics, Inc.) to obtain the integrated
optical density.
RT-qPCR
Total RNA from aortic tissues was extracted using
TRIzol® (Takara Bio, Inc.). cDNA was synthesized from
the RNA using a cDNA first strand synthesis kit (Takara Bio, Inc.)
according to the manufacturer's instructions (37°C for 15 min, 85°C
for 5 sec). qPCR was performed using SYBR-Green PCR master mix
(Takara Bio, Inc.). The qPCR reaction amplification system was as
follows: Initial denaturation at 95°C for 10 min, 40 of cycles of
denaturation at 95°C for 15 sec, annealing at 60°C for 15 sec and
elongation at 60°C for 60 sec. The reaction was performed in a PCR
amplification system (ABI 7300; Thermo Fisher Scientific, Inc.).
The following primers were used: Endothelin-1 (ET-1) forward (F),
5′-ACCACAGACCAAGGGAACAG-3′ and reverse (R),
5′-GGTCTTGATGCTGTTGCTGA-3′; vascular cell adhesion molecule-1
(VCAM-1) F, 5′-TGACATCTCCCCTGGATCTC-3′ and R,
5′-CTCCAGTTTCCTTCGCTGAC-3′; endothelial nitric oxide synthase
(eNOS) F, 5′-TGACCCTCACCGATACAACA-3′ and R,
5′-CTGGCCTTCTGCTCATTTTC-3′; and GAPDH F, 5′-CTCATGACCACAGTCCATGC-3′
and R, 5′-TTCAGCTCTGGGATGACCTT-3′. Relative gene expression data
was analyzed via the 2−ΔΔCq method (29).
Western blot analysis
Aortic tissues from all rats were extracted with
RIPA lysis buffer (Beyotime Institute of Biotechnology). Protein
concentration was determined using the BCA Protein Assay kit
(Beyotime Institute of Biotechnology), and 35 µg protein was
analyzed with 10% SDS-PAGE. Then, the protein was transferred to
the PVDF membrane. The membrane was treated in a blocking solution
(5% skimmed milk) at room temperature for 2 h and incubated with an
anti-ET-1 (1:1,000; cat. no. A0686; ABclonal Biotech Co., Ltd.),
anti-VCAM-1 (1:1,000; cat. no. A11236; ABclonal Biotech Co., Ltd.),
anti-eNOS (1:1,000; cat. no. A1548; ABclonal Biotech Co., Ltd.),
anti-CD31 (1:1,000; cat. no. A3181; ABclonal Biotech Co., Ltd.),
anti-GFP Tag (1:1,000; cat. no. 50430-2-AP; ProteinTech Group,
Inc.) or anti-β-actin antibodies (1:5,000; cat. no. 20536-1-AP;
ProteinTech Group, Inc.) at 4°C for overnight, followed by
incubation with HRP Goat Anti-Rabbit IgG (H+L) secondary antibody
(1:5,000; cat. no. AS014; ABclonal Biotech Co., Ltd.) at room
temperature for 1 h. The membrane was detected with the ECL
Detection reagents (EMD Millipore). The optical density of the
resulting bands was determined using ImageJ 2× software (Rawak
Software, Inc.), and the densitometry measurements were normalized
to that of β-actin.
Statistical analysis
Data are presented as the mean ± SD. Comparisons
were assessed with one-way ANOVA followed by Tukey's post hoc test,
using GraphPad Prism software version 5.0a (GraphPad Software,
Inc.). All experiments were conducted ≥3 times. P<0.05 was
considered to indicate a statistically significant difference.
Results
Body observation of rats in each
group
All rats survived. In the OS group rats, the initial
reaction to smoke was irritability, and then the rats exercised
less and closed their eyes. When exposure to smoke was prolonged,
rats gradually appeared to breathe abnormally and salivate, as well
as had an intermittent cough. After 2–3 weeks of audible wheezing,
their skin became yellow and signs of depression were observed,
with a loss of appetite and a loss of weight. The rats in the BMSC
group demonstrated normal activity, yellowing fur, a slightly
decreased appetite and little change in body size. The rats in the
sham group demonstrated normal activity before and after the
experiment, good appetite, fat bodies, no shedding of fur and no
cyanosis caused by breathing air (data not shown). The weight of
rats was significantly decreased in the model group (217.23±7.19 g)
compared with that in the sham group (254.26±9.92 g), but no
difference between the sham group and the BMSC group was observed
(251.78±6.34 g).
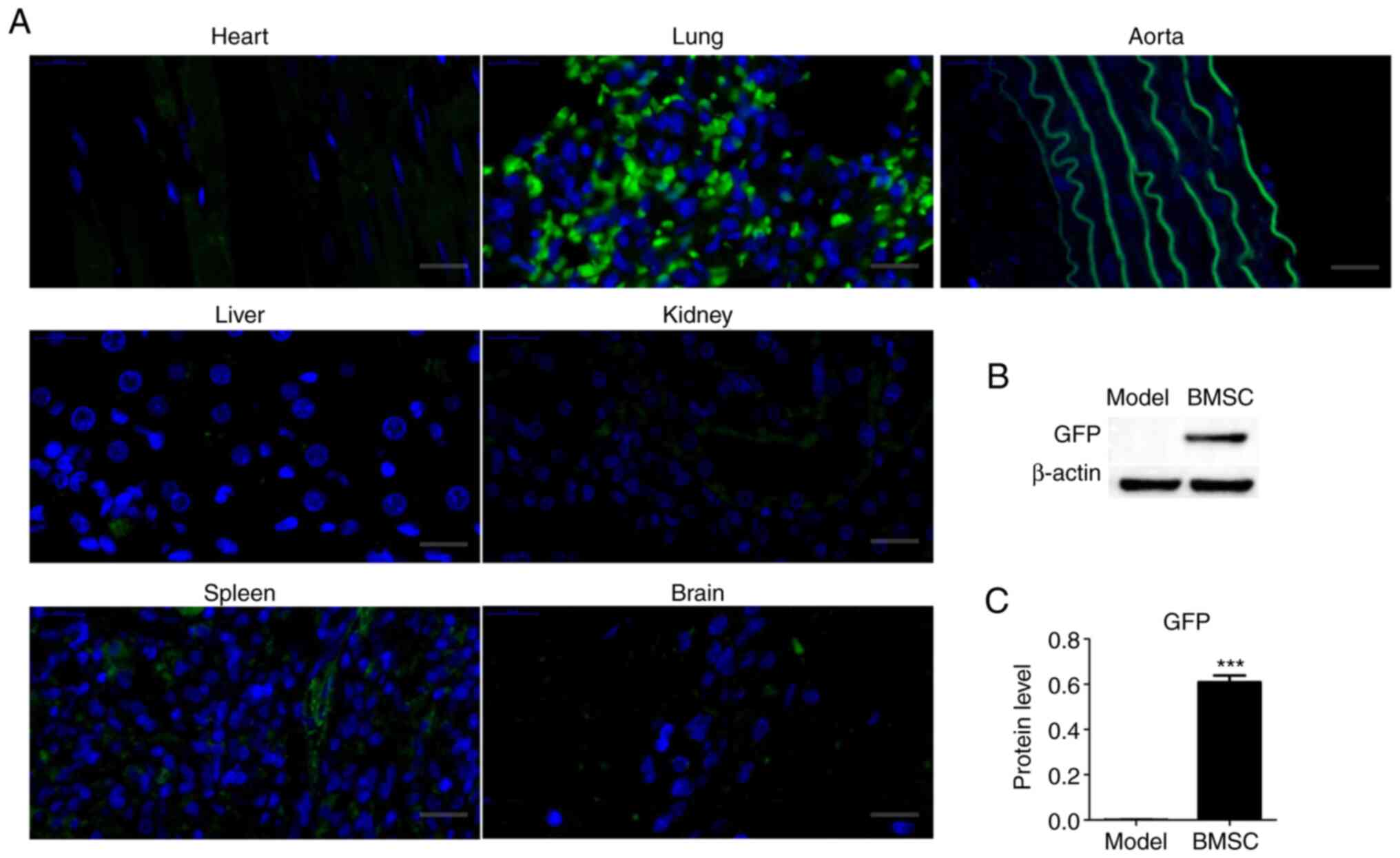
Localization of BMSCs in OS rats
To investigate the localization of BMSCs in OS rats,
GFP-BMSCs were injected into OS rats via the tail vein. As
presented in Fig. 1, green
fluorescence was identified in seven major organs of OS rats using
confocal microscopy. It was found that green fluorescence was
expressed in all seven tissues type, but was most obvious in lung
and arterial tissues (Fig. 1A).
This finding suggested that lung and arterial tissues may be
severely damaged in the OS model, and that BMSCs could migrate to
the damaged tissues. The GFP-labeled BMSCs were verified using
western blot analysis. GFP protein expression was significantly
higher in the BMSC group compared with that in the model group
(Fig. 1B and C).
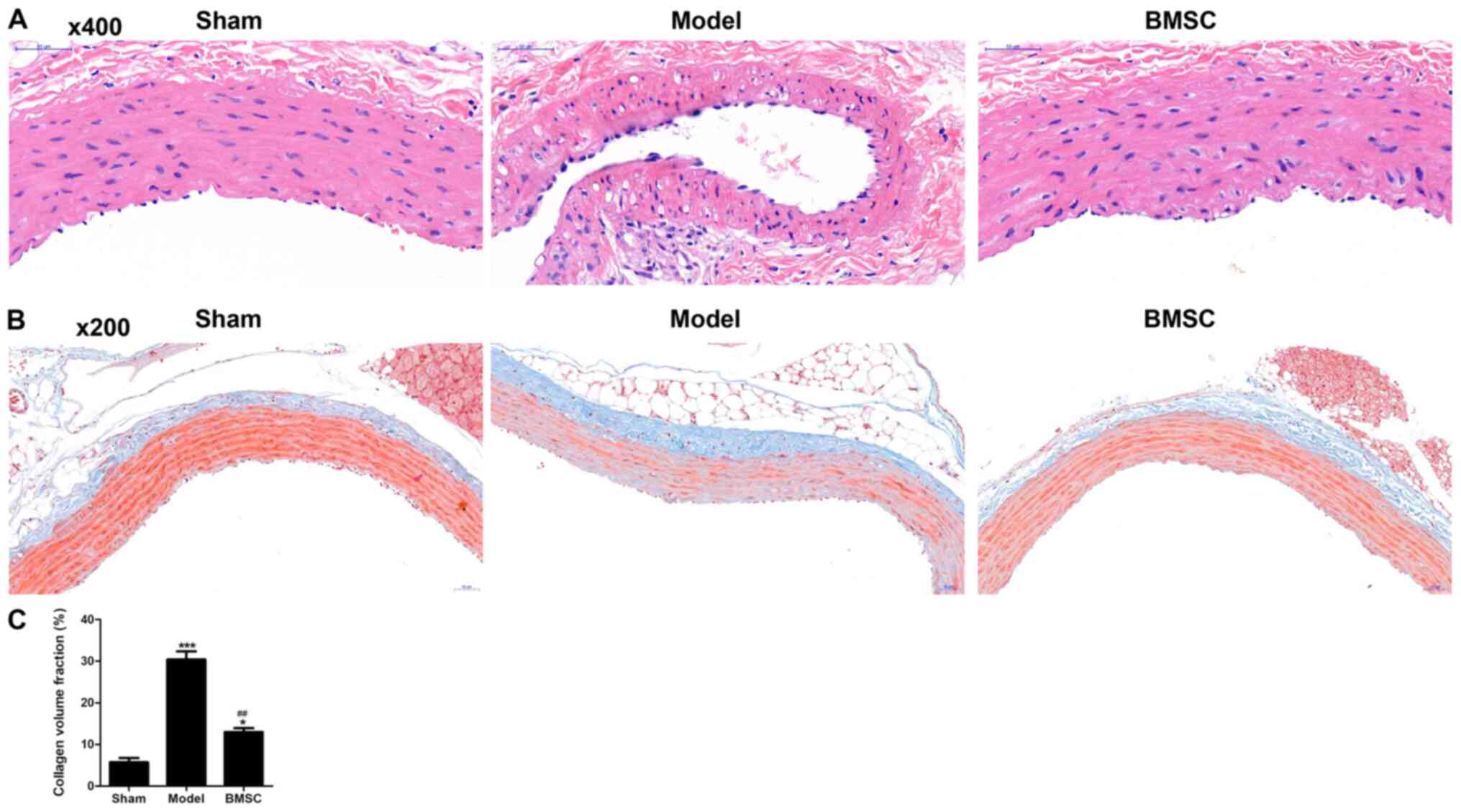
BMSCs repair arterial injury
The pathological morphology of arterial tissues was
detected using H&E staining. In the sham group, the vascular
wall structure of the aorta was clear, and the boundary of the
outer membrane, middle membrane and intima was clear (Fig. 2A). In the model group, the vascular
wall structure of the aorta was disordered, and the boundary
between the outer membrane, middle membrane and intima was not
clear. Moreover, the elastic membrane of the media was not visible,
and smooth muscle cells were disordered and swollen. Hyperplasia,
cell morphology changes and endothelial swelling were also
observed. In the BMSC group, the vascular wall structure of the
aorta was clear, the tunica media was thickened, the smooth muscle
cells were proliferated, the arrangement of the vascular wall
structure was not orderly and endothelial cells were slightly
swollen (Fig. 2A). These results
indicated that arterial tissues were severely damaged in the OS
model, and that BMSCs can inhibit these damages.
BMSCs inhibit collagenous fiber
formation in OS rats
The collagenous fibers of arterial tissues were
examined using Masson staining. Compared with that of the sham
group, the expression of collagen fibers (blue) in the outer and
medial membrane of aortic tissues of the model group was markedly
increased, and its elastic fibers (red) were notably decreased
(Fig. 2B). Compared with that of
the model group, the expression of collagen fibers in the BMSC
group was significantly decreased, but was still higher compared
with that in the sham group. The collagen fibers (blue) were also
quantified based on the CVF (Fig.
2C). These results suggested that BMSCs repaired arterial
injury by inhibiting the formation of collagen fibers.
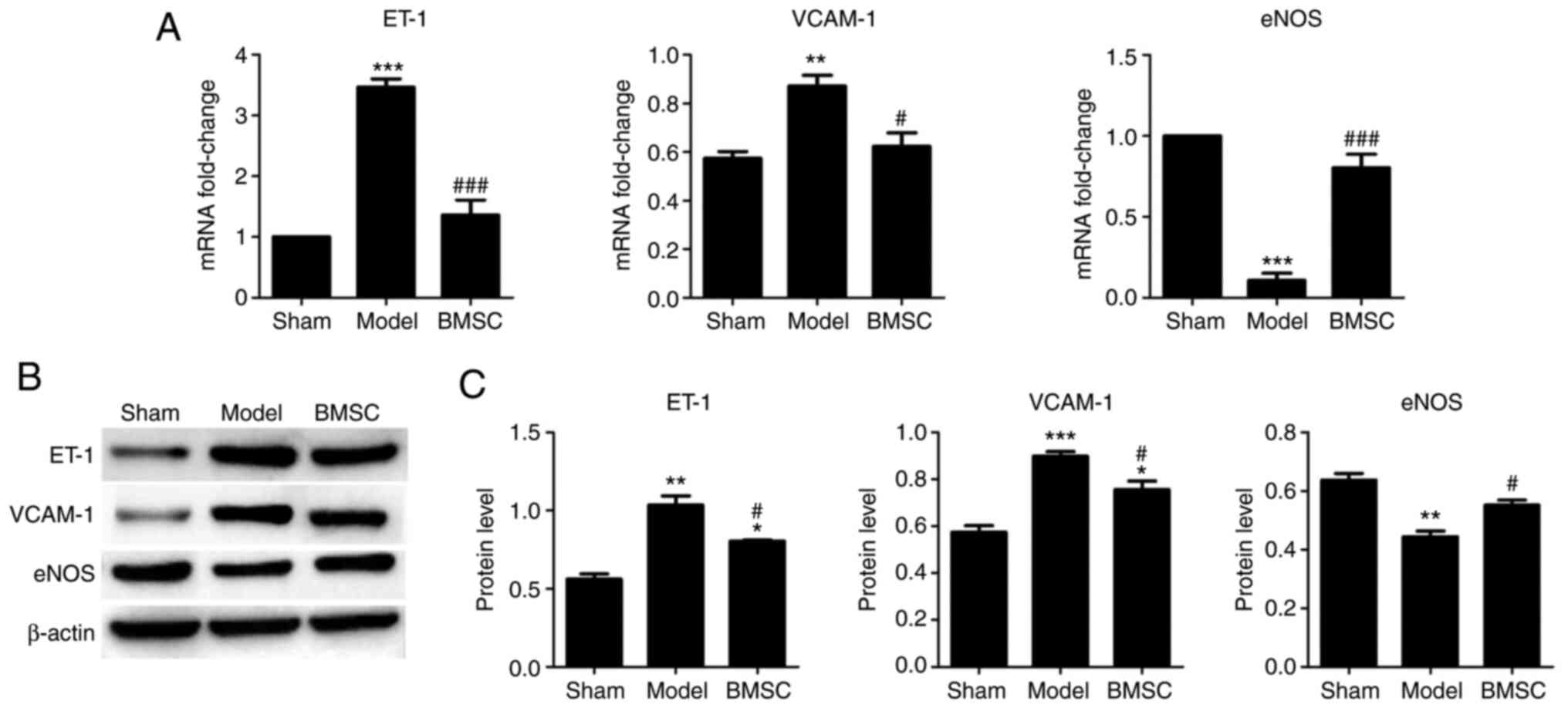
BMSCs suppresses endotheliocyte injury
in OS rats
To demonstrate whether BMSCs can suppress
endotheliocyte injury, the endotheliocyte injury-related genes
ET-1, VCAM-1 and eNOS were assessed via RT-qPCR and western
blotting. The expression levels of ET-1 and VCAM-1 were
significantly increased in the model group compared with the sham
group, but were decreased in the BMSC group compared with the model
group (Fig. 3A). The expression of
eNOS was significantly decreased in the model group compared with
the sham group, and was upregulated in the BMSC group compared with
the model group. The results of the western blot analysis were
consistent with the RT-qPCR results (Fig. 3B and C). These findings suggested
that BMSCs repaired arterial injury by inhibiting endotheliocyte
injury.
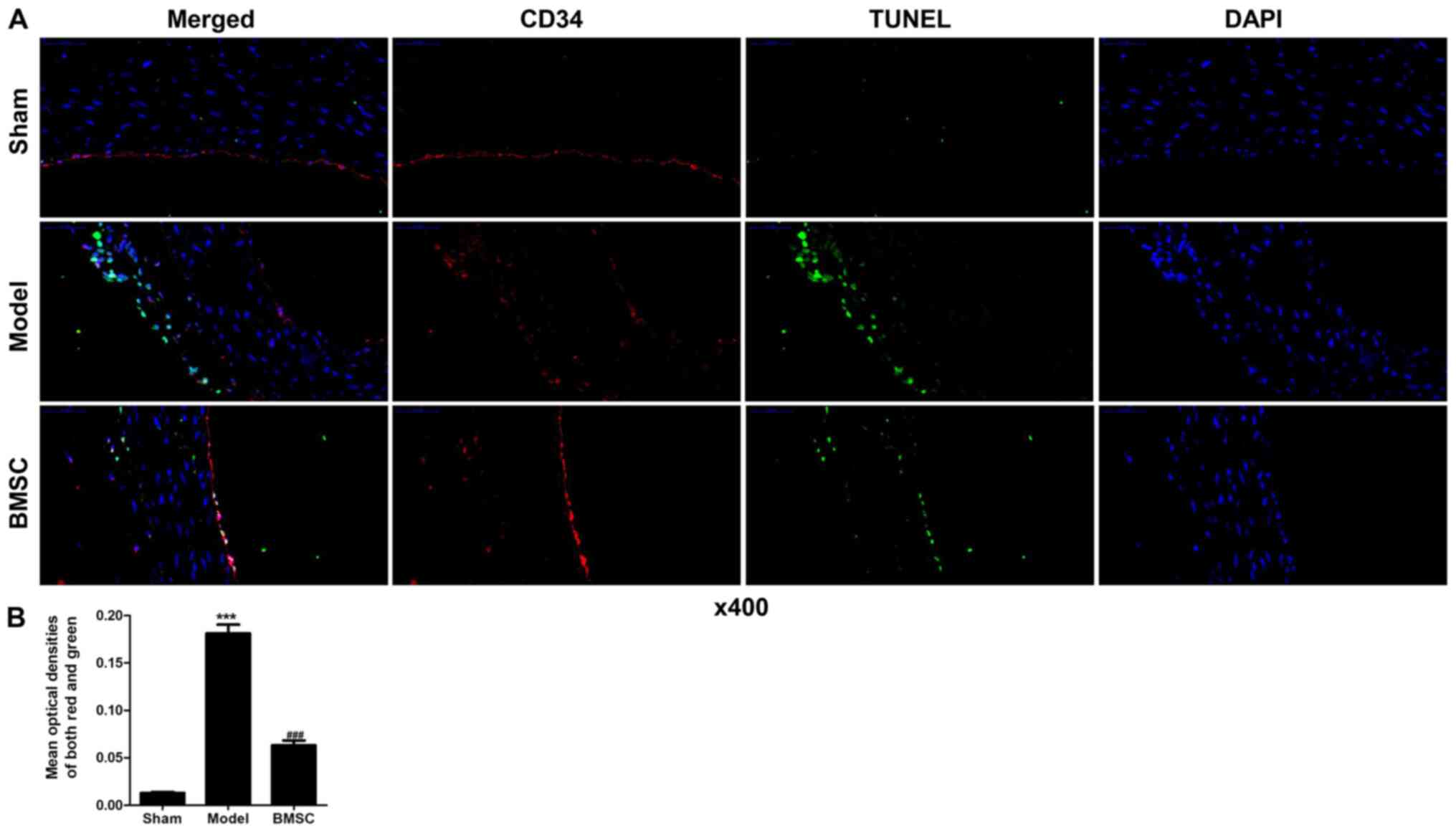
BMSCs suppress endotheliocyte
apoptosis in OS rats
A TUNEL assay was performed to detect endotheliocyte
apoptosis. The apoptotic cells under fluorescence microscopy
displayed green fluorescence, while the endotheliocytes under
fluorescence microscopy fluoresced red. The co-expression of red
and green fluorescence indicated apoptotic endotheliocytes.
Compared with the sham group, higher levels of endotheliocyte
apoptosis were observed in the model group. Endotheliocyte
apoptosis was significantly decreased in the BMSC group compared
with the model group, although it was greater compared with that in
the sham group (Fig. 4A and B).
Quantitative analysis of the co-expression of green and red
fluorescence indicated that BMSCs significantly suppressed the
apoptosis of endotheliocytes induced by OS model (Fig. 4B). These results demonstrated that
BMSCs repaired arterial injury by inhibiting endotheliocyte
apoptosis.
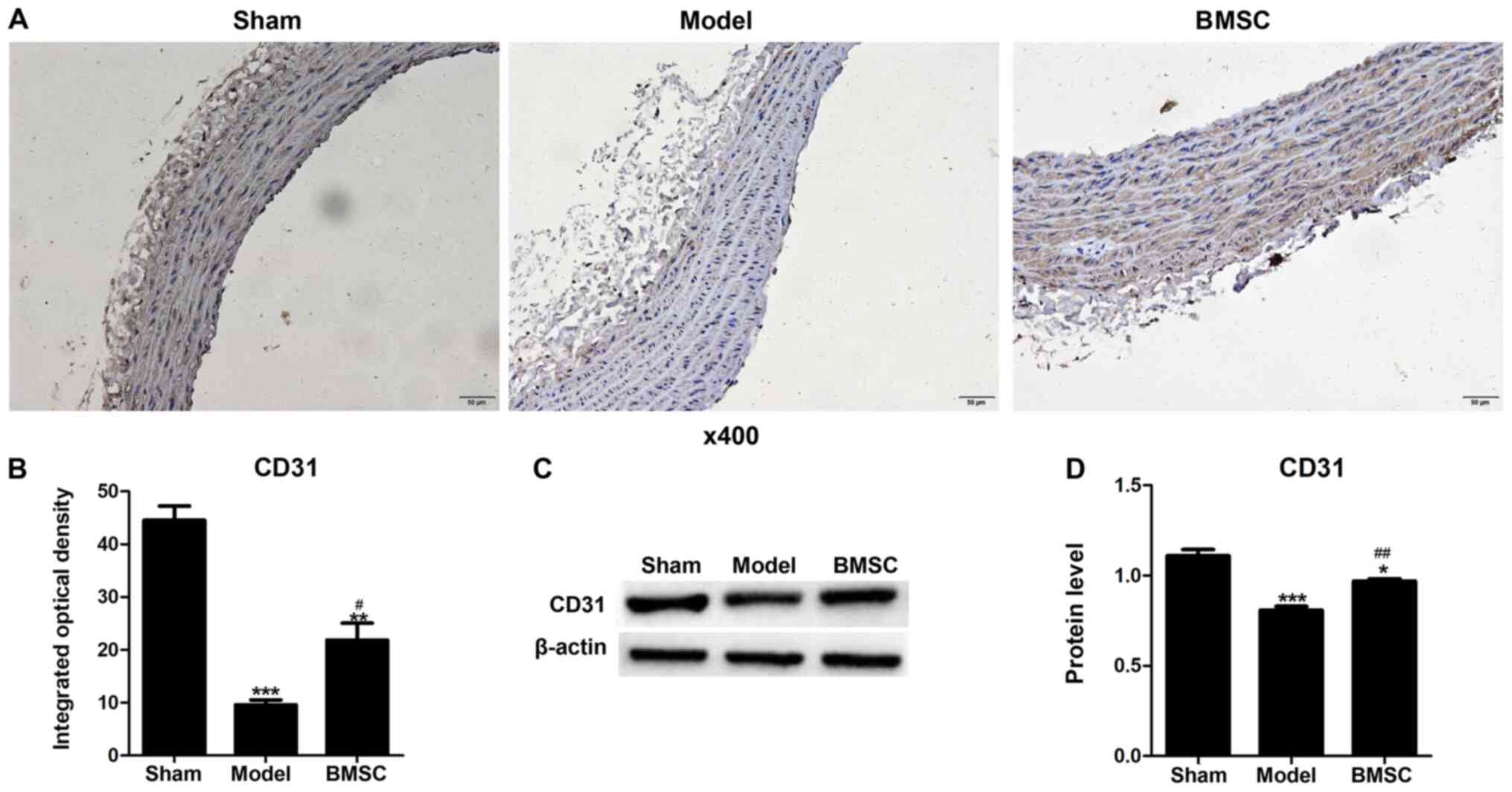
BMSCs increase the expression of CD31
in aortic tissues of OS rats
The expression of CD31 protein was detected using an
immunohistochemical assay. Lower levels of brown staining were
observed in the aortic tissues of the model group compared with
that in the sham group (Fig. 5A and
B). However, BMSC transplantation significantly increased the
brown staining in the aortic tissues of OS rats (Fig. 5A and B). The quantitative results of
the immunohistochemical assay are presented in Fig. 5B. CD31 protein expression was also
detected using western blot analysis (Fig. 5C and D), and the same changes were
identified as those indicated by the immunohistochemical assay
results. Collectively, it was suggested that BMSCs inhibited the
apoptosis of endotheliocytes in the aortic tissues of OS rats.
Discussion
Clinically, OSA combined with COPD is known as OS
(30). Both COPD and OSA involve
vascular endothelial injury, and the endothelial dysfunction in
patients with OS is more serious compared with that of either
condition alone and is correlated with the severity of the disease
(9). COPD and OSA have different
pathogeneses, leading to contradictory clinical treatments of
patients with OS (7). Currently,
there are no effective drugs for the treatment of OS in clinical
practice (14). Therefore, novel
therapeutic measures to improve vascular endothelial injury and
dysfunction are urgently required.
Cell therapy has been widely used in the study of
pulmonary diseases, and its research topics include the treatment
of chronic pulmonary diseases and vascular-related complications
via cell lung transplantation and circulating stem/progenitor cells
(15). BMSCs are non-hematopoietic
stem cells with multi-differentiation potential and have the
ability to induce tissue regeneration, anti-inflammatory effects
and immunosuppression (31). MSC
transplantation can downregulate inflammatory mediators in COPD and
OSAHS animal models (32,33). It has also been reported that
embryonic stem cells and BM-derived EPCs can differentiate into
VECs (16). Studies on various
animal disease models have revealed that MSCs can repair vascular
endothelial injury and correct dysfunction by inhibiting
inflammation, oxidative stress and endotheliocyte apoptosis, as
well as directly differentiating into endotheliocytes (34–36).
Moreover, MSCs alleviate acute lung injury by enhancing
anti-inflammatory pathways (37).
Based on the aforementioned studies, it was hypothesized that BMSC
therapy may be a new and effective treatment approach for vascular
endothelial injury, dysfunction or apoptosis in patients with OS.
To the best of our knowledge, few studies have investigated the
effect of BMSCs on aortic endothelial injury in an OS rat
model.
Our previous experiment demonstrated that the
inhibition of the progression of emphysema by BMSCs in the OS model
may be via the differentiation of BMSCs into endotheliocytes,
consequently suppressing endotheliocyte apoptosis, and by their
antioxidative stress function (27). However, the effect of BMSC
transplantation on aortic injury remained unknown. The present
study constructed an OS rat model using cigarette smoke and
intermittent hypoxia. It was found that transplanted BMSCs migrated
not only into lung tissues, but also into the aorta, heart, liver,
spleen, kidney and brain. However, the greatest number of BMSCs
migrated to lung and aortic tissues. Granulocyte colony-stimulating
factor can promote the migration of BMSCs to damaged lung tissue,
ultimately alleviating pulmonary fibrosis (38). Extracellular vesicles derived from
BMSCs could be beneficial in undertaking a reparative effort in
abdominal aortic aneurysm-induced degeneration of vascular tissue
(39). BMSCs can migrate to damaged
tissues (40,41), and in the current study, BMSCs are
present not only in the lungs but also in other tissues. This
result indicates that the OS model can lead to severe aortic and
lung injury. The present study detected aortic injury using H&E
and Masson staining. H&E staining demonstrated that the
vascular wall structure of the aorta was disordered, and the
boundary between the outer membrane, middle membrane and intima was
not clear. The elastic membrane of the media was not visible,
smooth muscle cells were disordered as well as showed swelling,
hyperplasia and cell morphology changes, and endothelial swelling
was observed in the OS groups. Moreover, the expression of collagen
fibers in the outer and middle aortic membranes of the OS group was
significantly increased, and its elastic fibers were markedly
decreased. However, in the BMSC group, BMSCs alleviated vascular
injury and suppressed the formation of collagen fibers. These
results suggested that arterial tissues were severely damaged in
the OS model and that BMSCs can inhibit these damages.
Nitric oxide (NO) and ET-1 are antagonistic vascular
active substances synthesized and are secreted by VECs (42,43).
ET-1 negatively regulates the release of NO in the endothelium, and
the increase in NO concentration inhibits the formation of ET-1.
The dynamic balance between the two maintains normal vascular
endothelial function, and an increase of ET-1 and a decrease of NO
are markers of vascular endothelial injury (44,45).
eNOS can synthesize NO. In previous studies, numerous factors in
vivo and in vitro were revealed to accelerate or delay
the process of reendothelialization by upregulating or
downregulating the expression of eNOS (46,47).
It has been reported that VCAM-1 is highly expressed in rat aortic
endothelial cells after balloon injury, and the expression of
VCAM-1 enhances with increasing inflammatory response time
(48). From the present RT-qPCR and
western blotting results, the expression levels of ET-1 and VCAM-1
were found to be significantly promoted, while the expression of
eNOS was significantly inhibited in OS rats compared with the sham
rats. Furthermore, an immunohistochemical assay was used to analyze
the expression of CD31 in the injured vessels. It was identified
that BMSCs could suppress endothelial cell apoptosis. Thus, the
current study indicated that BMSCs may be potent therapeutic tools
for vascular injury caused by OS.
There are some limitations to the present study. It
was identified that BMSCs were mainly localized to the lung and
aortic tissues, and a protective effect of BMSCs on aortic injury
of OS model was observed. However, the related mechanism via which
BMSCs protected against aortic injury remains unknown.
In conclusion, the present study demonstrated the
therapeutic effect of BMSC administration for aortic injury in OS
rats induced by cigarette smoke and intermittent hypoxia. It was
identified that BMSCs inhibited aortic injury in the OS model by
suppressing endotheliocyte apoptosis. However, the detailed
mechanism among these changes requires further investigation.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural
Science Foundation of China (grant no. 81560010) and the Science
and Technology Planning Project of Yunnan Province [grant no.
2017FE467(−100)].
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZJ, HB, JH, XH and JD conceived and designed the
study. MC, ZH, CY, LY, LH, HL, KZ and QW performed the experiments.
HL, KZ and QW processed the data. LH, HB, JH, XH and JD wrote the
manuscript. HB, JH and ZJ reviewed and edited the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The animal experiments were approved by the Animals
Ethics Committee of The First People's Hospital of Kunming and in
accordance with the Guide for the Care and Use of Laboratory
Animals.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Tsai SC: Chronic obstructive pulmonary
disease and sleep related disorders. Curr Opin Pulm Med.
23:124–128. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Portegies ML, Lahousse L, Joos GF, Hofman
A, Koudstaal PJ, Stricker BH, Brusselle GG and Ikram MA: Chronic
obstructive pulmonary disease and the risk of stroke. The Rotterdam
Study. Am J Respir Crit Care Med. 193:251–258. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gottlieb DJ and Punjabi NM: Diagnosis and
management of obstructive sleep Apnea: A review. JAMA.
323:1389–1400. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shahar E, Whitney CW, Redline S, Lee ET,
Newman AB, Nieto FJ, O'Connor GT, Boland LL, Schwartz JE and Samet
JM: Sleep-disordered breathing and cardiovascular disease:
Cross-sectional results of the Sleep Heart Health Study. Am J
Respir Crit Care Med. 163:19–25. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Munoz R, Duran-Cantolla J, Martínez-Vila
E, Gallego J, Rubio R, Aizpuru F and De La Torre G: Severe sleep
apnea and risk of ischemic stroke in the elderly. Stroke.
37:2317–2321. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Flenley DC: Sleep in chronic obstructive
lung disease. Clin Chest Med. 6:651–661. 1985.PubMed/NCBI
|
|
7
|
Marin JM, Soriano JB, Carrizo SJ, Boldova
A and Celli BR: Outcomes in patients with chronic obstructive
pulmonary disease and obstructive sleep apnea: The overlap
syndrome. Am J Respir Crit Care Med. 182:325–331. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sharma B, Neilan TG, Kwong RY, Mandry D,
Owens RL, McSharry D, Bakker JP and Malhotra A: Evaluation of right
ventricular remodeling using cardiac magnetic resonance imaging in
co-existent chronic obstructive pulmonary disease and obstructive
sleep apnea. COPD. 10:4–10. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Thomashow MA, Shimbo D, Parikh MA, Hoffman
EA, Vogel-Claussen J, Hueper K, Fu J, Liu CY, Bluemke DA,
Ventetuolo CE, et al: Endothelial microparticles in mild chronic
obstructive pulmonary disease and emphysema. The Multi-Ethnic Study
of Atherosclerosis Chronic Obstructive Pulmonary Disease study. Am
J Respir Crit Care Med. 188:60–68. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
McNicholas WT: COPD-OSA overlap syndrome:
Evolving evidence regarding epidemiology, clinical consequences,
and management. Chest. 152:1318–1326. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Willerson JT and Ridker PM: Inflammation
as a cardiovascular risk factor. Circulation. 109 (Suppl
1):II2–II10. 2004.PubMed/NCBI
|
|
12
|
Greenberg H, Ye X, Wilson D, Htoo AK,
Hendersen T and Liu SF: Chronic intermittent hypoxia activates
nuclear factor-kappaB in cardiovascular tissues in vivo. Biochem
Biophys Res Commun. 343:591–596. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ryan S and McNicholas WT: Intermittent
hypoxia and activation of inflammatory molecular pathways in OSAS.
Arch Physiol Biochem. 114:261–266. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rezaeetalab F, Rezaeitalab F and Dehestani
V: Inhaled steroids reduce apnea-hypopnea index in overlap
syndrome. Pneumologia. 62:212–214. 2013.PubMed/NCBI
|
|
15
|
Heise RL, Link PA and Farkas L: From here
to there, progenitor cells and stem cells are everywhere in lung
vascular remodeling. Front Pediatr. 4:802016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ando J and Yamamoto K: Vascular
mechanobiology: Endothelial cell responses to fluid shear stress.
Circ J. 73:1983–1992. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shi Z, Chen Y, Cao J, Zeng H, Yang Y, Chen
P, Luo H, Peng H, Cai S and Guan C: Intratracheal transplantation
of endothelial progenitor cells attenuates smoking-induced COPD in
mice. Int J Chron Obstruct Pulmon Dis. 12:947–960. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sun YQ, Deng MX, He J, Zeng QX, Wen W,
Wong DS, Tse HF, Xu G, Lian Q, Shi J and Fu QL: Human pluripotent
stem cell-derived mesenchymal stem cells prevent allergic airway
inflammation in mice. Stem Cells. 30:2692–2699. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Luo D, Yan X, Liu D, Zhou X and Liu G:
Differential effects of mesenchymal stem cells on a heterogeneous
cell population within lung cancer cell lines. Mol Cell Biochem.
378:107–116. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Le Blanc K, Tammik C, Rosendahl K,
Zetterberg E and Ringden O: HLA expression and immunologic
properties of differentiated and undifferentiated mesenchymal stem
cells. Exp Hematol. 31:890–896. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Allers C, Sierralta WD, Neubauer S, Rivera
F, Minguell JJ and Conget PA: Dynamic of distribution of human bone
marrow-derived mesenchymal stem cells after transplantation into
adult unconditioned mice. Transplantation. 78:503–508. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Carreras A, Almendros I and Farré R:
Potential role of bone marrow mesenchymal stem cells in obstructive
sleep apnea. Int J Stem Cells. 4:43–49. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Park JS, Kim HK, Kang EY, Cho R and Oh YM:
Potential therapeutic strategy in chronic obstructive pulmonary
disease using pioglitazone-augmented Wharton's Jelly-derived
mesenchymal stem cells. Tuberc Respir Dis (Seoul). 82:158–165.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu HM, Liu YT, Zhang J and Ma LJ: Bone
marrow mesenchymal stem cells ameliorate lung injury through
anti-inflammatory and antibacterial effect in COPD mice. J Huazhong
Univ Sci Technolog Med Sci. 37:496–504. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shangguan L, Li X, Wang Z and Luo Z:
Transforming growth factor-β1 induces bone marrow-derived
mesenchymal stem cells to differentiate into cancer-associated
fibroblasts. Zhonghua Zhong Liu Za Zhi. 37:804–809. 2015.(In
Chinese). PubMed/NCBI
|
|
26
|
Ding W, Li J, Singh J, Alif R,
Vazquez-Padron RI, Gomes SA, Hare JM and Shehadeh LA: miR-30e
targets IGF2-regulated osteogenesis in bone marrow-derived
mesenchymal stem cells, aortic smooth muscle cells, and
ApoE−/− mice. Cardiovasc Res. 106:131–142. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chen M, Huang Z, Bi H, Pan X, He J, He L,
He X, Du J, Zhou K, Wang L, et al: Effects of bone marrowderived
mesenchymal stem cell transplantation on chronic obstructive
pulmonary disease/obstructive sleep apnea overlap syndrome in rats.
Mol Med Rep. 20:4665–4673. 2019.PubMed/NCBI
|
|
28
|
Tang XJ, Wang B, Huang PY, Guo ZT, Tang
QL, Li SS and Yang XM: Effects of chronic intermittent hypoxia on
blood pressure and vascular remodeling. Zhonghua Er Bi Yan Hou Tou
Jing Wai Ke Za Zhi. 54:601–605. 2019.(In Chinese). PubMed/NCBI
|
|
29
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhang XW, Cai W, Jin F, Zhang YQ and Zhang
XL: Effect of Bi-level positive airway pressure ventilator on the
heart function and vascular endothelial function of patients with
the overlap syndrome. Zhonghua Jie He He Hu Xi Za Zhi. 34:17–20.
2011.(In Chinese). PubMed/NCBI
|
|
31
|
Kadota T, Fujita Y, Yoshioka Y, Araya J,
Kuwano K and Ochiya T: Extracellular vesicles in chronic
obstructive pulmonary disease. Int J Mol Sci. 17:18012016.
View Article : Google Scholar
|
|
32
|
Weiss DJ, Casaburi R, Flannery R,
LeRoux-Williams M and Tashkin DP: A placebo-controlled, randomized
trial of mesenchymal stem cells in COPD. Chest. 143:1590–1598.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Carreras A, Almendros I, Montserrat JM,
Navajas D and Farré R: Mesenchymal stem cells reduce inflammation
in a rat model of obstructive sleep apnea. Respir Physiol
Neurobiol. 172:210–212. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Luan Y, Zhang ZH, Wei DE, Zhao JJ, Kong F,
Cheng GH and Wang YB: Implantation of mesenchymal stem cells
improves right ventricular impairments caused by experimental
pulmonary hypertension. Am J Med Sci. 343:402–406. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Calió ML, Marinho DS, Ko GM, Ribeiro RR,
Carbonel AF, Oyama LM, Ormanji M, Guirao TP, Calió PL, Reis LA, et
al: Transplantation of bone marrow mesenchymal stem cells decreases
oxidative stress, apoptosis, and hippocampal damage in brain of a
spontaneous stroke model. Free Radic Biol Med. 70:141–154. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hung SC, Pochampally RR, Chen SC, Hsu SC
and Prockop DJ: Angiogenic effects of human multipotent stromal
cell conditioned medium activate the PI3K-Akt pathway in hypoxic
endothelial cells to inhibit apoptosis, increase survival, and
stimulate angiogenesis. Stem Cells. 25:2363–2370. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Luo F, Jiang W, Xu Y, Liu XM, Wang W,
Zhang W and Luo C: The mechanisms involved in mesenchymal stem cell
alleviation of sepsis-induced acute lung injury in mice: A pilot
study. Curr Ther Res Clin Exp. 93:1005932020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhao FY, Cheng TY, Yang L, Huang YH, Li C,
Han JZ, Li XH, Fang LJ, Feng DD, Tang YT, et al: G-CSF inhibits
pulmonary fibrosis by promoting BMSC homing to the lungs via
SDF-1/CXCR4 chemotaxis. Sci Rep. 10:105152020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Sajeesh S, Broekelman T, Mecham R and
Ramamurthi A: Stem cell derived extracellular vesicles for vascular
elastic matrix regenerative repair. Acta Biomate. 113:267–278.
2020. View Article : Google Scholar
|
|
40
|
Yamada M, Kubo H, Kobayashi S, Ishizawa K,
Numasaki M, Ueda S, Suzuki T and Sasaki H: Bone marrow-derived
progenitor cells are important for lung repair after
lipopolysaccharide-induced lung injury. J Immunol. 172:1266–1272.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ortiz LA, Gambelli F, McBride C, Gaupp D,
Baddoo M, Kaminski N and Phinney DG: Mesenchymal stem cell
engraftment in lung is enhanced in response to bleomycin exposure
and ameliorates its fibrotic effects. Proc Natl Acad Sci USA.
100:8407–8411. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Konczalla J, Wanderer S, Mrosek J, Schuss
P, Platz J, Güresir E, Seifert V and Vatter H: Crosstalk between
the angiotensin and endothelin-system in the cerebrovasculature.
Curr Neurovasc Res. 10:335–345. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Millatt LJ, Abdel-Rahman EM and Siragy HM:
Angiotensin II and nitric oxide: A question of balance. Regul Pept.
81:1–10. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Signorello MG, Viviani GL, Armani U,
Cerone R, Minniti G, Piana A and Leoncini G: Homocysteine, reactive
oxygen species and nitric oxide in type 2 diabetes mellitus. Thromb
Res. 120:607–613. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Wiwanitkit V: Endothelin-1 and protein
kinase C co-expression in the pathogenesis of diabetic retinopathy.
J Diabetes Complications. 21:359–362. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Urao N, Okigaki M, Yamada H, Aadachi Y,
Matsuno K, Matsui A, Matsunaga S, Tateishi K, Nomura T, Takahashi
T, et al: Erythropoietin-mobilized endothelial progenitors enhance
reendothelialization via Akt-endothelial nitric oxide synthase
activation and prevent neointimal hyperplasia. Circ Res.
98:1405–1413. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Schwartz R, Osborne-Lawrence S, Hahner L,
Gibson LL, Gormley AK, Vongpatanasin W, Zhu W, Word RA, Seetharam
D, Black S, et al: C-reactive protein downregulates endothelial NO
synthase and attenuates reendothelialization in vivo in mice. Circ
Res. 100:1452–1459. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Tanaka H, Sukhova GK, Swanson SJ, Clinton
SK, Ganz P, Cybulsky MI and Libby P: Sustained activation of
vascular cells and leukocytes in the rabbit aorta after balloon
injury. Circulation. 88:1788–1803. 1993. View Article : Google Scholar : PubMed/NCBI
|