Introduction
Endometrial cancer is the sixth most common cancer
in women worldwide; approximately 320,000 new cases were diagnosed
in 2012 (1). The incidence rate and
number of mortalities from endometrial cancer are increasing,
despite improvements in overall survival rates (2). Overall survival rates for endometrial
cancer are good, and the 5-year survival rate for disease confined
to the uterus is as high as 96% (3).
In the majority of cases, patients with endometrial cancer exhibit
symptoms that include abnormal vaginal bleeding or discharge, and
~90% of women diagnosed with endometrial cancer have abnormal
uterine bleeding (4). Therefore, in
pre- and post-menopausal women exhibiting abnormal uterine
bleeding, transvaginal ultrasonography and endometrial biopsy
should be performed for the potential early diagnosis of
endometrial cancer (5). Early
detection of endometrial cancer improves prognosis; therefore,
improved diagnostic methods are critical for patients with symptoms
of endometrial cancer, and screening methods for the detection of
early-stage cancer prior to the onset of symptoms are expected to
achieve meaningful improvements in overall survival. However, there
are currently no routine, effective screening tests for endometrial
cancer (6).
Tumor markers may be secreted by tumors at levels in
excess of those secreted by normal tissues and cells (7). Such tumor markers can include unique
extracellular matrix or cell adhesion molecules, growth factors,
receptors, cytokines, or products of abnormal metabolic processes.
In addition, antibodies produced by the body against tumor markers
may themselves be used as markers. Tumor markers can be used as
indicators of diagnosis, prognosis, and can informative for
clinical management and follow-up (7). Numerous investigations have assessed
different biological variables in tissue and serum samples from
patients with endometrial cancer, in order to detect possible
biomarkers that could be predictive of clinical outcomes. For
example, Gadducci et al (8)
reported the ability of different tissue and serum biomarkers,
including p53, the PENT-PIK3-mTOR signaling pathway, MSI,
β-Catenin, the Ras-MAPK-ERK signaling pathway and VEGF in tissue
and CA 125, CA15-3, YKL-40 VEGF and HE-4 in serum, to predict
clinical outcomes in patients with endometrioid-type endometrial
carcinoma. Elevated serum CA125 levels have been detected in 11–43%
of patients with endometrial cancer (9,10).
Investigators have shown that elevated CA125 levels are able to
predict extrauterine lesions, large tumor size, invasion of the
lymphovascular space and deep myometrium, involvement of the cervix
and adnexa, positive cytology, lymph node metastasis, and the
requirement for adjuvant treatment (11). However, in patients with pure
endometrioid-type endometrial cancer who have undergone adjuvant
therapy and in patients with serous papillary carcinoma, the role
of serum CA125 is controversial (12). Additionally, CA125 has limited utility
for monitoring the response to chemotherapy and may not predict
recurrence in the absence of other clinical signs (13). Therefore, additional studies are
required to identify novel tumor markers for more accurate
detection and management of endometrial cancers.
Peroxiredoxins (PRDXs), which were first discovered
~25 years ago (14), are a family of
22-to 27-kDa, non-selenium-dependent glutathione peroxidases that
destroy peroxides, organic hydroperoxides and peroxynitrite
(15). The PRDX gene family (16) includes six isoforms in mammals; these
isoforms can be classified into three subclasses: Typical
2-cysteine PRDXs (PRDXs 1–4), atypical 2-cysteine PRDX (PRDX5), and
atypical 1-cysteine PRDX (PRDX6) (17). PRDXs are associated with cell
proliferation, apoptosis, differentiation, and gene expression
in vitro (18). Notably, high
expression levels of PRDXs are associated with increased resistance
to radiation and certain chemotherapeutics, whereas PRDX deficiency
can sensitize cells to chemotherapy and apoptosis (19).
In addition, oxidative metabolism of estrogen and
the subsequent formation of reactive oxygen species (ROS) are
important estrogen-related carcinogenic mechanisms (20). Felty et al (21) suggested that physiological estrogen
concentrations could induce significant oxidative stress in
vitro and that estrogen-induced ROS formation occurs in the
mitochondria. For example, in estrogen receptor (ER)-positive
breast cancer, which is a major estrogen-dependent cancer,
estrogens are important cellular ROS inducers (22). Additionally, published data suggest
that PRDX1, PRDX3, PRDX4 and PRDX5 expression levels are associated
with prognosis in patients with breast cancer (23–25).
Similarly, endometrial cancer is an estrogen-dependent malignancy;
therefore, certain PRDXs may be associated with the prognosis or
clinicopathological characteristics of endometrial cancer.
Accordingly, in the present study, the expression
levels of various PRDXs were evaluated in endometrial cancer
tissues, and the relationship between PRDX expression and prognosis
in patients with endometrial cancer was investigated.
Materials and methods
Tissues
Fresh tissue specimens were collected from the
endometrial tissues of 70 patients who underwent hysterectomy at
Inje University Busan Paik Hospital (Busan, Korea) between January
2008 and December 2010. Using a retrospective chart review, a
database was established containing information regarding
prognostic factors, such as age, body mass index, histopathological
factors, stage, recurrence, and survival. Tissue specimens were
classified into two groups: Normal endometrium and endometrial
cancer. 42 patients with endometrial cancer received full staging
surgery, including total hysterectomy, bilateral
salpingo-oophorectomy, omentectomy, bilateral pelvic
lymphadenectomy and para-aortic lymphadenectomy. Endometrial
carcinomas are graded by their architecture and revised
International Federation of Gynecology and Obstetrics (FIGO)
classification (26) is used for
their staging. Normal endometrial tissues were obtained from
hysterectomies performed for benign uterine disease, including
uterine myoma, adenomyosis, or uterine prolapse.
This study was performed following the acquisition
of informed consent from all patients and approval from the
Institutional Review Board of Busan Paik Hospital.
RNA isolation and cDNA synthesis
Total RNA was isolated from tissue samples using
TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA) according to the manufacturer's protocol. cDNA
was synthesized from 1 µg total RNA using a TOPscript™ cDNA
Synthesis Kit (Enzynomics, Daejeon, Korea). The reverse
transcription (RT) reaction was performed at 42°C for 60 min in a
reaction mixture containing 10X TOPscript™ RT reaction MIX (dT18)
and TOPscript™ Reverse TranscriptaseR+ (200 U/µl) in a
total volume of 20 µl.
Semi-quantitative RT-polymerase chain
reaction (PCR)
The RT product (1 µl) was used for PCR. Each
reaction contained 10 pM of each primer, 1.5 mM MgCl2,
250 µM dNTPs, 10 mM Tris-HCl (pH 9.0), 30 mM KCl, and 1 unit Top
DNA polymerase (AccuPower® PCR PreMix; cat. no. K-2012;
Bioneer Corporation, Daejeon, Korea). The primers utilized are
presented in Table I. Reactions were
performed on a T100 Thermal Cycler (Bio-Rad, Hercules, CA, USA).
Amplification was conducted with the following thermal cycling
conditions: 5 min at 95°C; 35 cycles of amplification consisting of
30 sec at 95°C, 40 sec at 55°C, and 30 sec at 72°C; and a final
extension at 72°C for 5 min. For analysis, 5 µl of the product was
subjected to agarose gel electrophoresis and visualized by ethidium
bromide. PCR bands were quantified using the Multi Gauge V2.2
software program (FUJI PHOTO FILM, Japan).
 | Table I.Primer sequences for RT-PCR analysis
of PRDX. |
Table I.
Primer sequences for RT-PCR analysis
of PRDX.
| Gene | Primer sequence | Product size
(bp) |
|---|
| PRDX1 | Forward
5′-GGGTATTCTTCGGCAGATCA-3′ | 221 |
|
| Reverse
5′-GCAGCCTGGCACTAAAACAG-3′ |
|
| PRDX2 | Forward
5′-GTGTCCTTCGCCAGATCACT-3′ | 154 |
|
| Reverse
5′-ACGTTGGGCTTAATCGTGTC-3′ |
|
| PRDX3 | Forward
5′-CAAGCAAAATTATTCAGCACCA-3′ | 129 |
|
| Reverse
5′-CCCCTTAAAGTCATCAAGGCT-3′ |
|
| PRDX4 | Forward
5′-GAAATTATCGCTTTTGGCGA-3′ | 149 |
|
| Reverse
5′-AGTGGAATCCTTATTGGCCC-3′ |
|
| PRDX5 | Forward
5′-GTGGTGGCCTGTCTGAGTGT-3′ | 150 |
|
| Reverse
5′-GGACACCAGCGAATCATCTA-3′ |
|
| PRDX6 | Forward
5′-GGATGGGGATAGTGTGATGG-3′ | 81 |
|
| Reverse
5′-TTGGTGAAGACTCCTTTCGG-3′ |
|
| hB2MF | Forward
5′-TGACTTTGTCACAGCCCAAG-3′ | 265 |
|
| Reverse
5′-GAGCTACCTGTGGAGCAACC-3′ |
|
Immunohistochemistry
Paraffin block was provided at Inje University Busan
Paik Hospital (Busan, Korea). Immunohistochemical analysis was
performed on 4-µm-thick paraffin-embedded sections of 42 tissues,
which were mounted on SuperFrost Plus slides. Slides were heated
for 1 h at 60°C, deparaffinized in xylene, rehydrated in graded
alcohol and rinsed in distilled water. Antigen retrieval and
immunohistochemistry were performed using either a Benchmark XT or
Discovery XT automated immunohistochemistry system (Ventana Medical
Systems, Inc., Tucson, AZ) with an OptiView DAB IHC Detection kit.
Slides were incubated for 34 min at room temperature with diluted
primary antibody. The appropriately diluted primary antibodies were
as follows: PRDX1 (Abcam, Cambridge, MA, USA; cat. no. ab109506;
dilution, 1:500), PRDX3 (Abcam; cat. no. ab16751; dilution,
1:1,000), PRDX5 (Abcam; cat. no. ab127922; dilution, 1:200), and
PRDX6 (Abcam; cat. no. ab133348; dilution, 1:700). After antibody
staining, sections were washed in distilled water, lightly
counterstained with hematoxylin, rehydrated and mounted with
coverslips. The intensity of immunohistochemical staining was
evaluated in five randomly selected high-power fields using a light
microscope (magnification ×400). Sections were subsequently divided
into four categories: -, no positive cells; +, weak cytoplasmic
staining; ++, moderate cytoplasmic staining; +++, strong
cytoplasmic staining. The results were independently assessed by
one investigator who was blinded to patient characteristics, stage
and prognosis.
Statistical analysis
Statistical analyses were performed using MedCalc
version 14.8.1 (Frank Schoonjans, Ghent University, Belgium).
Categorical variables were compared using χ2 tests and
Fisher's exact tests. The mean, median, and standard deviation were
calculated for continuous variables and were compared using
Mann-Whitney U-tests for two groups, Kruskal-Wallis tests for three
or more unmatched groups, and Pearson's correlation coefficients.
Survival analysis was performed by Kaplan-Meier analysis and
generalized log-rank tests. P<0.05 was considered to indicate a
statistically significant difference.
Results
Measurement of PRDX expression levels
in endometrial cancer and normal endometrial tissues by RT-PCR
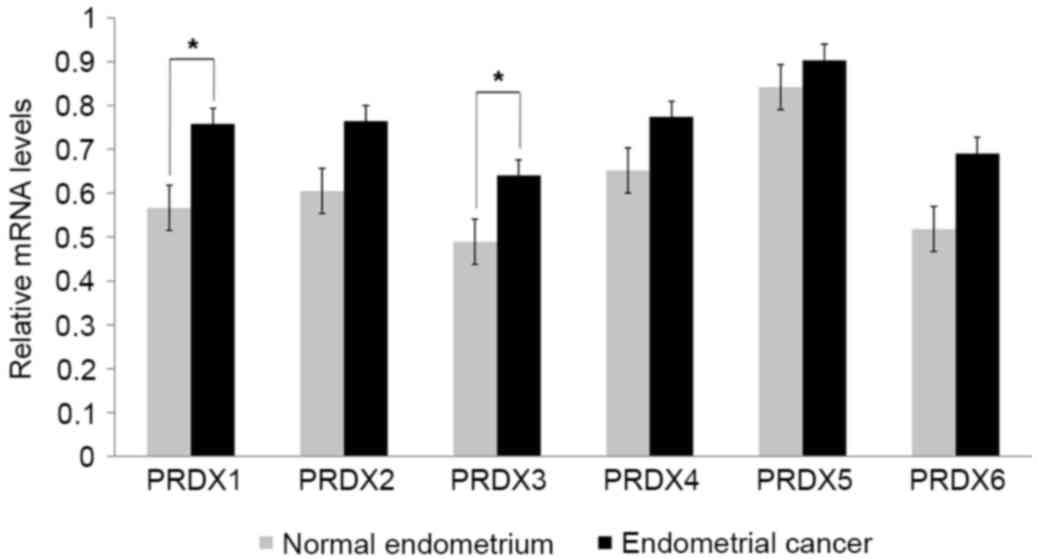
The expression levels of various PRDX mRNAs were
analyzed in endometrial cancer (n=26) and normal endometrial tissue
(n=10) to determine whether PRDX expression was associated with
endometrial cancer. All PRDX mRNAs were upregulated in endometrial
cancer compared with normal endometrial tissue (Fig. 1). Although the expression levels of
PRDX2, PRDX4 and PRDX5 mRNAs were higher in endometrial cancer than
in normal endometrium, these differences were not significant.
Additionally, the expression level of PRDX6 mRNA in endometrial
cancer was marginally higher than that in normal endometrium (0.52
vs. 0.69, respectively; P=0.0612). Notably, the expression levels
of PRDX1 (0.57 vs. 0.76, respectively; P=0.0015) and PRDX3 (0.49
vs. 0.64, respectively; P=0.0134) were significantly increased in
endometrial cancer compared with those in normal endometrial
tissues (Fig. 1).
Measurement of PRDX expression levels
in endometrial cancer and paired normal endometrial tissues by
immunohistochemistry
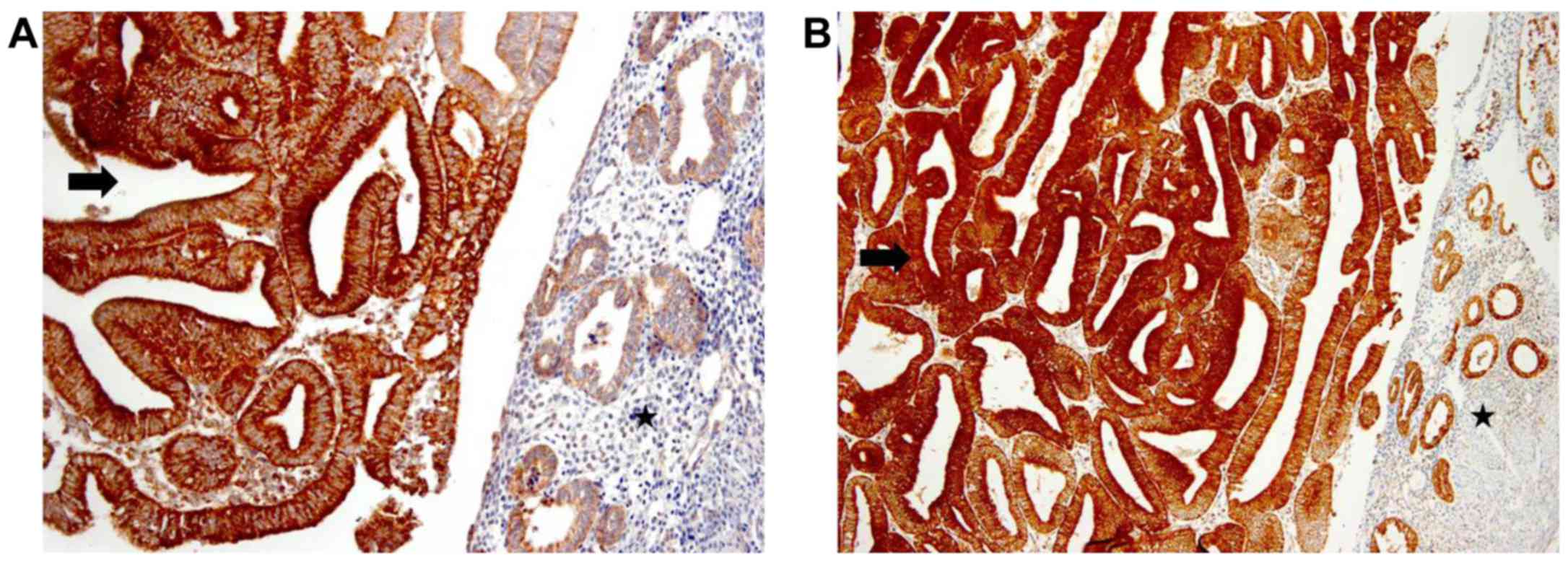
The expression levels of PRDX proteins were compared
between endometrial cancer and paired normal endometrial tissues
using immunohistochemistry. Based on the RT-PCR analysis, which
detected marked changes in the expression of PRDX1, PRDX3, and
PRDX6 mRNAs, and a previous study in which PRDX5 was found to be
overexpressed in endometrial cancer (27), immunohistochemical staining for PRDX1,
PRDX3, PRDX5, and PRDX6 was performed. The results showed that
59.5% of endometrial cancer samples and 31.6% of normal endometrial
samples showed strong cytoplasmic staining for PRDX3, and
statistical analysis revealed that PRDX3 was significantly
overexpressed in endometrial cancer compared with normal
endometrial tissue (P=0.0001; Table
II; Fig. 2A). Similarly, a total
76.2% of endometrial cancer samples and 55.9% of normal endometrial
tissues were strongly positive for PRDX5, and PRDX5 was
significantly overexpressed in endometrial cancer compared with
that in endometrial tissues (P=0.0023; Table II; Fig.
2B). However, no significant differences in the expression of
PRDX 1 and 6 were observed between cancer and normal tissue.
| Table II.Intensity of immunostaining for PRDXs
in normal endometrial tissue from cancer and endometrial cancer
samples. |
Table II.
Intensity of immunostaining for PRDXs
in normal endometrial tissue from cancer and endometrial cancer
samples.
|
|
|
| Staining intensity,
n (%) |
|
|---|
|
|
|
|
|
|
|---|
| PRDX isoform | Sample type | No. of samples | + | ++ | +++ | P-value |
|---|
| 1 | Normal | 24 | 5 (20.8) | 7 (29.2) | 12 (50.0) | NS |
|
| Cancer | 42 | 17 (40.5) | 19 (45.2) | 6 (14.3) |
|
| 3 | Normal | 19 | 3 (15.8) | 10 (52.6) | 6 (31.6) | 0.0001a |
|
| Cancer | 42 | 6 (14.3) | 11 (26.2) | 25 (59.5) |
|
| 5 | Normal | 34 | 8 (23.5) | 7 (20.6) | 19 (55.9) | 0.0023a |
|
| Cancer | 42 | 3 (7.1) | 7 (16.7) | 32 (76.2) |
|
| 6 | Normal | 25 | 5 (20.0) | 16 (64.0) | 4 (16.0) | NS |
|
| Cancer | 42 | 12 (28.6) | 22 (52.4) | 8 (19.0) |
|
Analysis of the association between
PRDX3/PRDX5 overexpression and prognosis in patients with
endometrial cancer
The associations between PRDX isoform expression and
prognosis were evaluated in patients with endometrial cancer in
order to investigate the usefulness of PRDX as a prognostic
biomarker for endometrial cancer. As PRDX3 and PRDX5 were
demonstrated to be overexpressed in endometrial cancer by
immunohistochemistry, prognostic factors for endometrial cancer
were investigated according to PRDX3 and PRDX5 expression. Patients
were divided into the low (weak or moderate staining) and high
(strong staining) PRDX3 and PRDX5 expression groups, and
clinicopathological and prognostic variables of endometrial cancer,
including grade, histology, FIGO stage, depth of myometrial
invasion and lymph node status were compared between the low and
high expression groups of each marker.
High PRDX5 expression was more frequently observed
in advanced-stage cancer than in early-stage cancer (100 vs. 66.7%;
P=0.0399). Additionally, high expression of PRDX5 tended to be
associated with the presence of lymph node metastasis; however,
this association was not statistically significant (100 vs. 68.7%;
P=0.0838). A total of 6 cases of recurrent cancer were reported,
and all showed high expression of PRDX5. Additionally, 8 patients
with endometrial cancer died during follow-up, and the majority of
these patients exhibited high expression of PRDX3 (75% vs. 55.9% of
patients who survived) and PRDX5 (87.5% vs. 73.5% of patients who
survived); however, no significant associations were detected
(Table III).
| Table III.Associations between PRDX3/PRDX5
expression and clinicopathological factors in patients with
endometrial cancer. |
Table III.
Associations between PRDX3/PRDX5
expression and clinicopathological factors in patients with
endometrial cancer.
|
|
| PRDX3 | PRDX5 |
|---|
|
|
|
|
|
|---|
| Factor | No. of
patients | Low expression
(n=17, 38.5%) | High expression
(n=25, 61.5%) | P-value | Low expression
(n=10, 23.8%) | High expression
(n=32, 76.2%) | P-value |
|---|
| Age
(years)a | 42 | 54.9±11.0 | 52.1±10.7 | 0.4107 | 51.4±7.7 | 53.8±12.0 | 0.5371 |
| Body
mass index (kg/m2)a | 42 | 24.3±2.4 | 25.6±5.1 | 0.3623 | 25.4±4.4 | 24.9±4.3 | 0.7646 |
| CA125
(U/ml)a | 42 | 242.6±575.1 | 36.7±41.9 | 0.0805 | 43.8±55.1 | 143.8±427.3 | 0.4684 |
| Endometrial cancer
typeb |
|
|
| 0.9115 |
|
| 0.8002 |
|
Estrogen-dependent | 14 | 5 (35.7) | 9 (64.3) |
| 3 (21.4) | 11 (78.6) |
|
|
Estrogen-independent | 28 | 12 (42.9) | 16 (57.1) |
| 7 (25.0) | 21 (75.0) |
|
| Histological
gradeb |
|
|
| 0.2372 |
|
| 0.6813 |
| 1 | 15 | 4 (26.7) | 11 (73.3) |
| 4 (26.7) | 11 (73.3) |
|
| 2 | 18 | 8 (44.4) | 10 (55.6) |
| 5 (27.8) | 13 (72.2) |
|
| 3 | 8 | 5 (62.5) | 3 (37.5) |
| 1 (12.5) | 7 (87.5) |
|
| Histological
typeb |
|
|
| 0.8986 |
|
| 0.5568 |
|
Endometrioid | 38 | 16 (42.1) | 22 (57.9) |
| 10 (26.3) | 28 (73.7) |
|
|
Non-endometrioid | 4 | 1 (25.0) | 3 (75.0) |
| 0 (0.0) | 4 (100.0) |
|
| FIGO
stageb |
|
|
| 0.1744 |
|
| 0.0399c |
|
Early | 30 | 10 (33.3) | 20 (66.7) |
| 10 (33.3) | 20 (66.7) |
|
|
Advanced | 12 | 7 (58.3) | 5 (41.7) |
| 0 (0.0) | 12 (100.0) |
|
| Myometrial invasion
(%)b |
|
|
| 0.7549 |
|
| 0.8363 |
|
<50 | 24 | 9 (37.5) | 15 (62.5) |
| 6 (25.0) | 18 (75.0) |
|
|
≥50 | 18 | 8 (44.4) | 10 (55.6) |
| 4 (22.2) | 14 (77.8) |
|
| Lymph node
metastasisb |
|
|
| 0.2837 |
|
| 0.0838 |
| No | 32 | 11 (34.4) | 21 (65.6) |
| 10 (31.3) | 22 (68.8) |
|
|
Yes | 10 | 6 (60.0) | 4 (40.0) |
| 0 (0.0) | 10 (100.0) |
|
| LVSIb |
|
|
| 0.7397 |
|
| 0.7535 |
| No | 27 | 11 (40.7) | 16 (59.3) |
| 7 (25.9) | 20 (74.1) |
|
|
Yes | 15 | 6 (40.0) | 9 (60.0) |
| 3 (20.0) | 12 (80.0) |
|
|
Recurrenceb |
|
|
| 0.9488 |
|
| 0.6611 |
| No | 36 | 14 (38.9) | 22 (61.1) |
| 9 (25.0) | 27 (75.0) |
|
|
Yes | 6 | 3 (50.0) | 3 (50.0) |
| 1 (16.7) | 5 (83.3) |
|
|
Survivalb |
|
|
| 0.5546 |
|
| 0.6545 |
| No | 8 | 2 (25.0) | 6 (75.0) |
| 1 (12.5) | 7 (87.5) |
|
|
Yes | 34 | 15 (44.1) | 19 (55.9) |
| 9 (26.5) | 25 (73.5) |
|
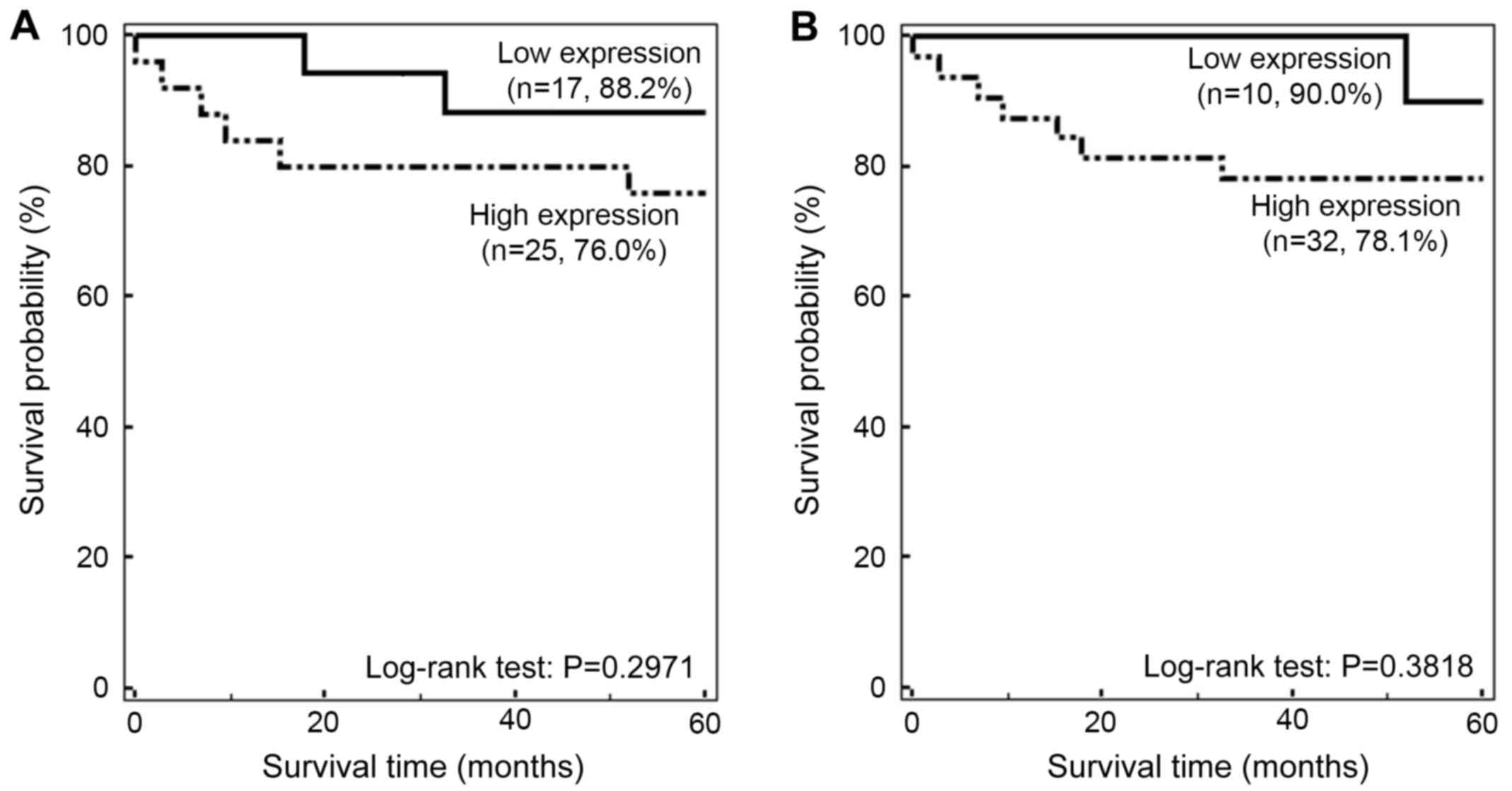
Although the 5-year survival rate was increased in
the low PRDX3 expression group compared with that in the high PRDX3
expression group (88.2 vs. 76.0%, respectively), this association
was not significant (P=0.2971; Fig.
3A). Additionally, the 5-year survival rate in the low PRDX5
expression group was non-significantly higher than that in the high
PRDX5 expression group (90 vs. 78.1%; P=0.3818; Fig. 3B).
Discussion
PRDX pathways are used by cells as enzymatic
antioxidant defense systems in order to prevent oxidative and
nitrosative damage caused by the presence of ROS (28). Among the six isoforms of PRDX
(PRDX1-6), PRDX3 is localized in the mitochondria and acts as a
mitochondrial scavenger of hydrogen peroxide, which protects
mitochondria against oxidative damage and affects diverse cellular
processes, including growth, differentiation, carcinogenesis and
apoptosis (29). PRDX5 is localized
in the cytosol, mitochondria, peroxisome and nucleus, and is able
to reduce hydrogen peroxide, alkyl hydroperoxides, and
peroxynitrite. PRDX5 is also able to use cytosolic and
mitochondrial thioredoxins as physiological electron donors
(30). These proteins are
overexpressed in several types of malignancy, including breast
cancer, mesothelioma, lung cancer, cervical cancer, prostate
cancer, and multiple myeloma (31).
Mitochondria in cancer cells are known to contain high levels of
PRDX3 and PRDX5 (32–36), and Song et al (37) reported that the mitochondrial PRDX3
antioxidant system, which is exclusively present in mitochondria,
may be a potential target for cancer therapy.
In the present study, the mRNA levels of all PRDX
isoforms were higher in endometrial cancer than in normal
endometrial tissue, with significant increases observed for
PRDX1 and PRDX3 mRNAs. However, on
immunohistochemical analysis, PRDX3 and PRDX5 were clearly elevated
in the majority of endometrial cancer samples, with PRDX3 protein
showing significantly increased expression. Although PRDX1
mRNA expression was significantly higher in endometrial cancer,
PRDX1 protein levels tended to be lower in endometrial cancer than
in the normal endometrium. This difference between the mRNA and
protein levels of PRDX1 may be due to the presence of extracellular
PRDXs, such as macrophage PRDX or secreted PRDXs (38). As PRDX3 and PRDX5 were found to be
highly expressed in endometrial cancer by RT-PCR and
immunohistochemistry, these targets may be considered biomarkers
associated with endometrial cancer.
Generally, factors associated with the prognosis of
endometrial cancer include FIGO stage, histology, tumor grade,
depth of myometrial invasion, lymphovascular space invasion, and
lymph node status (39). In this
study, high expression of PRDX5 was associated with advanced-stage
endometrial cancer. Although not statistically significant, high
expression of PRDX5 was also observed more frequently in patients
with lymph node metastasis, and overexpression of PRDX3 and PRDX5
appeared more frequent in patients who died during follow-up.
The lack of significance among these findings could
be explained by the small sample size and the limited stages and
histological characteristics of the samples. Indeed, the majority
of the samples were from patients with early-stage endometrial
cancer and low-grade tumors. Therefore, more meaningful results may
be obtained in studies with larger sample sizes and tumors with
various clinicopathological characteristics.
In conclusion, PRDX3 and PRDX5 were highly expressed
in endometrial cancer. In particular, the increased expression of
PRDX5 was significantly associated with advanced stage, and tended
to be increased among patients with positive lymph node status.
Although no significant differences were detected in this analysis,
the increased expression of PRDX3 and PRDX5 may be associated with
decreased survival time. Therefore, these proteins may be candidate
prognostic markers in patients with endometrial cancer. Additional
studies with larger sample sizes are required to fully determine
the prognostic roles of PRDX3 and PRDX5 in endometrial cancer.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PRDX
|
peroxiredoxin
|
|
hB2MF
|
human β2-microglobulin
|
|
LVSI
|
lymphovascular space invasion
|
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Evans T, Sany O, Pearmain P, Ganesan R,
Blann A and Sundar S: Differential trends in the rising incidence
of endometrial cancer by type: Data from a UK population-based
registry from 1994 to 2006. Br J Cancer. 104:1505–1510. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fei LY: Fast Stats: An interactive tool
for access to SEER cancer statistics. Surveillance Research
Program, National Cancer Institute; http://seer.cancer.gov/faststatsFebruary
2–2013
|
|
4
|
Smith-Bindman R, Kerlikowske K, Feldstein
VA, Subak L, Scheidler J, Segal M, Brand R and Grady D: Endovaginal
ultrasound to exclude endometrial cancer and other endometrial
abnormalities. JAMA. 280:1510–1517. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Committee on Practice
Bulletins-Gynecology, . Practice bulletin no. 128: Diagnosis of
abnormal uterine bleeding in reproductive-aged women. Obstet
Gynecol. 120:197–206. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Berek JS: Novak's Gynecology. 13th.
Lippincott Williams & Wilkins; Philadelphia, PA, USA: 2002
|
|
7
|
Ueda Y, Enomoto T and Kimura T, Miyatake
T, Yoshino K, Fujita M and Kimura T: Serum biomarkers for early
detection of gynecologic cancers. Cancers (Basel). 2:1312–1327.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gadducci A, Cosio S and Genazzani AR:
Tissue and serum biomarkers as prognostic variables in
endometrioid-type endometrial cancer. Crit Rev Oncol Hematol.
80:181–192. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hakala A, Kacinski BM, Stanley ER, Kohorn
EI, Puistola U, Risteli J, Risteli L, Tomás C and Kauppila A:
Macrophage colony-stimulating factor 1, a clinically useful tumor
marker in endometrial adenocarcinoma: comparison with CA 125 and
the aminoterminal propeptide of type III procollagen. Am J Obstet
Gynecol. 173:112–119. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Takeshima N, Shimizu Y, Umezawa S, Hirai
Y, Chen JT, Fujimoto I, Yamauchi K and Hasumi K: Combined assay of
serum levels of CA125 and CA19-9 in endometrial carcinoma. Gynecol
Oncol. 54:321–326. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Baser E, Gungor T, Togrul C, Turkoglu O
and Celen S: Preoperative prediction of poor prognostic parameters
and adjuvant treatment in women with pure endometrioid type
endometrial cancer: What is the significance of tumor markers? Eur
J Gynaecol Oncol. 35:513–518. 2014.PubMed/NCBI
|
|
12
|
Yasa C, Takmaz O, Dural O and Akhan SE:
The value of tumor markers in endometrial carcinoma: Review of
literature. Sci Res. 4:966–970. 2013.
|
|
13
|
Price FV, Chambers SK, Carcangiu ML,
Kohorn EI, Schwartz PE and Chambers JT: CA 125 may not reflect
disease status in patients with uterine serous carcinoma. Cancer.
82:1720–1725. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim K, Kim I, Lee KY, Rhee S and Stadtman
E: The isolation and purification of a specific ‘protector’ protein
which inhibits enzyme inactivation by a thiol/Fe (III)/O2
mixed-function oxidation system. J Biol Chem. 263:4704–4711.
1988.PubMed/NCBI
|
|
15
|
Rhee SG: Cell signaling. H2O2, a necessary
evil for cell signaling. Scienc e. 312:1882–1883. 2006.
|
|
16
|
Hall A, Nelson K, Poole LB and Karplus PA:
Structure-based insights into the catalytic power and
conformational dexterity of peroxiredoxins. Antioxid Redox Signal.
15:795–815. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Neumann CA, Cao J and Manevich Y:
Peroxiredoxin 1 and its role in cell signaling. Cell Cycle.
8:4072–4078. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mu ZM, Yin XY and Prochownik EV: Pag, a
putative tumor suppressor, interacts with the Myc Box II domain of
c-Myc and selectively alters its biological function and target
gene expression. J Biol Chem. 277:43175–43184. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yo YD, Chung YM, Park JK, Ahn CM, Kim SK
and Kim HJ: Synergistic effect of peroxiredoxin II antisense on
cisplatin-induced cell death. Exp Mol Med. 34:273–277. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Okoh V, Deoraj A and Roy D:
Estrogen-induced reactive oxygen species-mediated signalings
contribute to breast cancer. Biochim Biophys Acta. 1815:115–133.
2011.PubMed/NCBI
|
|
21
|
Felty Q, Xiong WC, Sun D, Sarkar S, Singh
KP, Parkash J and Roy D: Estrogen-induced mitochondrial reactive
oxygen species as signal-transducing messengers. Biochemistry.
44:6900–6909. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Musarrat J, Arezina-Wilson J and Wani A:
Prognostic and aetiological relevance of 8-hydroxyguanosine in
human breast carcinogenesis. Eur J Cancer. 32A:1–1214. 1996.
|
|
23
|
O'Leary PC, Terrile M, Bajor M, Gaj P,
Hennessy BT, Mills GB, Zagozdzon A, O'Connor DP, Brennan DJ, Connor
K, et al: Peroxiredoxin-1 protects estrogen receptor alpha from
oxidative stress-induced suppression and is a protein biomarker of
favorable prognosis in breast cancer. Breast Cancer Res.
16:R792014. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Karihtala P, Kauppila S, Soini Y and
Arja-Jukkola-Vuorinen: Oxidative stress and counteracting
mechanisms in hormone receptor positive, triple-negative and
basal-like breast carcinomas. BMC Cancer. 11:2622011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Elamin A, Zhu H, Hassan AM, Xu N and
Ibrahim ME: Peroxiredoxin V: A candidate breast tumor marker of
population specificity. Mol Clin Oncol. 1:541–549. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pecorelli S: Revised FIGO staging for
carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol
Obstet. 105:103–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Han S, Shen H, Jung M, Hahn BS, Jin BK,
Kang I, Ha J and Choe W: Expression and prognostic significance of
human peroxiredoxin isoforms in endometrial cancer. Oncol Lett.
3:1275–1279. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rhee SG, Chae HZ and Kim K:
Peroxiredoxins: A historical overview and speculative preview of
novel mechanisms and emerging concepts in cell signaling. Free
Radic Biol Med. 38:1543–1552. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wonsey DR, Zeller KI and Dang CV: The
c-Myc target gene PRDX3 is required for mitochondrial homeostasis
and neoplastic transformation. Proc Natl Acad Sci USA. 99:pp.
6649–6654. 2002; View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Knoops B, Clippe A, Bogard C, Arsalane K,
Wattiez R, Hermans C, Duconseille E, Falmagne P and Bernard A:
Cloning and characterization of AOEB166, a novel mammalian
antioxidant enzyme of the peroxiredoxin family. J Biol Chem.
274:30451–30458. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Whitaker HC, Patel D, Howat WJ, Warren AY,
Kay JD, Sangan T, Marioni JC, Mitchell J, Aldridge S, Luxton HJ, et
al: Peroxiredoxin-3 is overexpressed in prostate cancer and
promotes cancer cell survival by protecting cells from oxidative
stress. Br J Cancer. 109:983–993. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kinnula VL, Lehtonen S, Sormunen R,
Kaarteenaho-Wiik R, Kang SW, Rhee SG and Soini Y: Overexpression of
peroxiredoxins I, II, III, V, and VI in malignant mesothelioma. J
Pathol. 196:316–323. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Noh DY, Ahn SJ, Lee RA, Kim SW, Park IA
and Chae HZ: Overexpression of peroxiredoxin in human breast
cancer. Anticancer Res. 21:2085–2090. 2001.PubMed/NCBI
|
|
34
|
Choi JH, Kim TN, Kim S, Baek SH, Kim JH,
Lee SR and Kim JR: Overexpression of mitochondrial thioredoxin
reductase and peroxiredoxin III in hepatocellular carcinomas.
Anticancer Res. 22:3331–3335. 2002.PubMed/NCBI
|
|
35
|
Nonn L, Berggren M and Powis G: Increased
expression of mitochondrial peroxiredoxin-3 (Thioredoxin
Peroxidase-2) protects cancer cells against hypoxia and
drug-induced hydrogen peroxide-dependent. Mol Cancer Res.
1:682–689. 2003.PubMed/NCBI
|
|
36
|
Kropotov A, Gogvadze V, Shupliakov O,
Tomilin N, Serikov VB, Tomilin NV and Zhivotovsky B: Peroxiredoxin
V is essential for protection against apoptosis in human lung
carcinoma cells. Exp Cell Res. 312:2806–2815. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Song IS, Kim HK, Jeong SH, Lee SR, Kim N,
Rhee BD, Ko KS and Han J: Mitochondrial peroxiredoxin III is a
potential target for cancer therapy. Int J Mol Sci. 12:7163–7185.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Riddell JR, Wang XY, Minderman H and
Gollnick SO: Peroxiredoxin 1 stimulates secretion of
proinflammatory cytokines by binding to TLR4. J Immunol.
184:1022–1030. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Creasman WT, Odicino F, Maisonneuve P,
Quinn MA, Beller U, Benedet JL, Heintz AP, Ngan HY and Pecorelli S:
Carcinoma of the corpus uteri. FIGO 26th annual report on the
results of treatment in gynecological cancer. Int J Gynaecol
Obstet. 95 Suppl 1:S105–S143. 2006. View Article : Google Scholar : PubMed/NCBI
|