Cancer is the first or second leading cause of death
in patients aged <70 in 91 of 172 countries and is expected to
be the leading cause of cancer-associated death worldwide (1). In China, there has been an increase in
the incidence and mortality rates of cancer, and cancer is the
leading cause of death, constituting a major public health crisis;
~4,292,000 new cancer cases and ~2,814,000 cancer-associated deaths
occurred in China in 2015, with lung cancer being the most common
and the leading cause of cancer-associated deaths (2). Non-small cell lung cancer (NSCLC)
accounts for 80–85% of lung cancer cases (3), and the majority of patients with NSCLC
are diagnosed at an advanced stage with <30% of patients
undergoing surgical resection (4).
Large-scale sequencing studies have revealed the
complex genomic landscape of NSCLC (5–8) and the
genomic differences between lung adenocarcinomas and lung
squamous-cell carcinomas (9). In
NSCLCs, mutant oncogenes drive proliferation and tumor maintenance,
particularly in adenocarcinomas (5).
Tumors may be heavily dependent on these driver mutations for
survival rather than multiple downstream genetic and epigenetic
abnormalities (10). Mutations in
EGFR and gene fusion of EML4-anaplastic lymphoma kinase (ALK) are
the best studied and actionable genes in lung adenocarcinomas and
have been observed in 15–60 and 3–5% of lung cancer cases,
respectively (11,12). Other reported oncogenic driver
mutations include KRAS, ROS1, BRAF, ERBB2 and MET (8,12). The
presence of EGFR mutations and ALK gene fusions in lung cancer are
associated with longer median survival times compared with the wild
type status (>24 months vs. 5–9 months) (13).
Obtaining a suitable specimen is the first step for
accurate gene alteration testing, allowing for histological and
molecular analysis, and preventing false-negative results and test
failures. The primary sample types currently used for diagnosis are
tissues and cytology samples, with surgical resections being the
first used for clinical molecular diagnosis (14). However, 50–70% of patients with
NSCLCs present with advanced stage cancer at diagnosis and are
unresectable (15). It is difficult
to obtain an adequate amount of tumor tissue from patients with
advanced NSCLC (7). Liquid biopsy is
a noninvasive method that overcomes the heterogeneity of tumor
tissues, and repeat biopsies and can be obtained throughout the
progression of NSCLC, and this may potentially improve early
detection and post-treatment monitoring of patients with lung
cancer (16,17). Liquid biopsy may be one of the most
influential techniques in the field of detecting and monitoring
cancer over the next decade (18).
Malignant pleural effusion (MPE), which is observed
in ~50% of advanced NSCLC cases and most frequently in lung
adenocarcinoma (19,20), is a common manifestation of stage IV
NSCLC. For a number of patients, it may be the only specimen
available for diagnostic and molecular testing (21,22).
With a high tumor content, most MPE samples contain numerous tumor
cells, which are sufficient for pathological diagnosis and for
determining driver gene status (23–25). MPE
samples can be obtained less invasively and repeatedly over time
compared with samples from the primary lesion. Furthermore,
previous studies have suggested that pleural effusions are a
suitable source for enrichment of putative cancer stem cells
(26,27).
NGS exceeds the limitations of traditional Sanger
sequencing, allowing a huge number of independent sequencing
reactions to run simultaneously, which has laid the foundation for
development of targeted therapies (40). This detection method has the power to
identify new single nucleotide variations (SNVs) or indel
mutations, and chromosomal rearrangements (41–44). Liu
et al evaluated the molecular profiling of lung
adenocarcinoma using MPE specimens utilizing NGS, illustrating 22
cases of EGFR mutations within 30 patients (73%), including L858R,
G719S, exon 20 insertion and exon 19 deletion, with an average
sequencing depth on target of 359X (45).
Although MPE is a potential candidate for molecular
testing, its use in multiplexed molecular profiling with NGS has
not been fully investigated. In the present study, multiple
oncogene mutations were detected, including 17 genes closely
associated with advanced lung cancer induction in 108 MPE samples
using deep sequencing methods.
Between December 2017 and July 2018, MPE samples
from 108 patients (51 males, 56 females, and 1 patient with unknown
gender; median age, 68 years; age range, 30–89 years) with
pathologically confirmed lung cancer were collected. Written
informed consent was obtained from all participants, and the
present study was approved by the Institutional Review Board of
Affiliated Changzhou No. 2 People's Hospital (Changzhou, China).
Pleural effusion samples, 20–50 ml, were obtained at the time of
diagnosis. All cell blocks of MPE samples contained tumor cells.
Clinical characteristics were obtained from medical records.
The pleural fluid sample was centrifuged for 10 min
in a 15-ml centrifuge tube at 268 × g. The supernatant was
discarded and 50% ethanol was added to 10 ml, and centrifuged for
10 min at 268 × g. After discarding the supernatant, 10% buffer
neutral formaldehyde solution was added to 10 ml, followed by
centrifugation for 10 min at 268 × g. The supernatant was discarded
and the cell precipitates were removed and wrapped in wrapping
paper. Subsequently, 10% buffer neutral formaldehyde solution was
added for internal fixation for 10 min, then placed into the
automatic dehydrator to dehydrate and transferred into a xylene
solution for transparency (15 min at room temperature). The samples
were subsequently waxed, embedded and cut into slices of 2–3-µm
thickness. HE staining was subsequently performed. Samples were
incubated in xylene for 5–10 min once, followed by: 3–5 min in 95%
ethanol twice; and 1–2 min in 80% ethanol. Following rinsing, the
samples were stained with hematoxylin for 10 min, rinsed and
differentiated using 1% ethanol hydrochloride for 2–5 sec. After
rinsing with running water for 10–15 min, the samples were stained
with 0.5% eosin solution for 3–5 min. Finally, the slides were
incubated with 80% ethanol for 1–2 sec, 95% ethanol for 1–2 sec,
100% ethanol for 2–5 sec (repeated twice), xylene for 1–2 min
(repeated once). Subsequently, the tissue sections were dried,
dropped neutral resins and covered with a cover slide. All the
above steps were at room temperature.
The tumor DNA was extracted using a human tissue DNA
extraction kit (YunYing Medical Technology Co. Ltd.) according to
the manufacturer's protocols. DNA was eluted in the elution buffer,
and concentration and purity were assessed using a NanoDrop
spectrophotometer. DNA was stored at −20°C until use. Library
preparation was constructed using the VAHTS Universal DNA Library
Prep kit for Illumina® sequencing (Illumina, Inc.).
Target enrichment was performed using optimized probes (YunYing
Medical Technology Co. Ltd.) that targeted the exons of 17 lung
cancer-associated genes and specific introns. Sequencing was
performed on an Illumina® NextSeq500 platform (Illumina,
Inc.) according to the manufacturer's protocols.
Pleural effusion samples from 108 patients with
advanced NSCLC were obtained between December 2017 and July 2018,
and patient characteristics are shown in Table I. A total of 51 patients (47.2%) were
male and 56 (51.8%) were female, and there was one patient whose
gender was unknown. The median age was 68 years (range, 30–89
years), with 11 patients between 30 and 50 years, 51 patients
between 50 and 70 years, 44 patients between 70 and 90 years, and 2
patients whose ages were unknown. Adenocarcinoma was the most
commonly observed histology, in 60.1% of cases. A total of six
representative hematoxylin and eosin stains of MPE samples with the
respective controls are shown in the supplemental materials
(Fig. S1).
ERBB2 (HER2), a known proto-oncogene located on the
long arm of human chromosome 17, is a member of the human EGFR
(HER/EGFR/ERBB) family (49). Among
the 108 MPE samples, there were only 2 cases (females aged 89 and
62 years old) with insertion of AYVM in M774_A775 in the ERBB2
amino acid sequence, which is sensitive to trastuzumab (Herceptin),
ado-trastuzumab emtansine (Kadcyla), and afatinib dimaleate
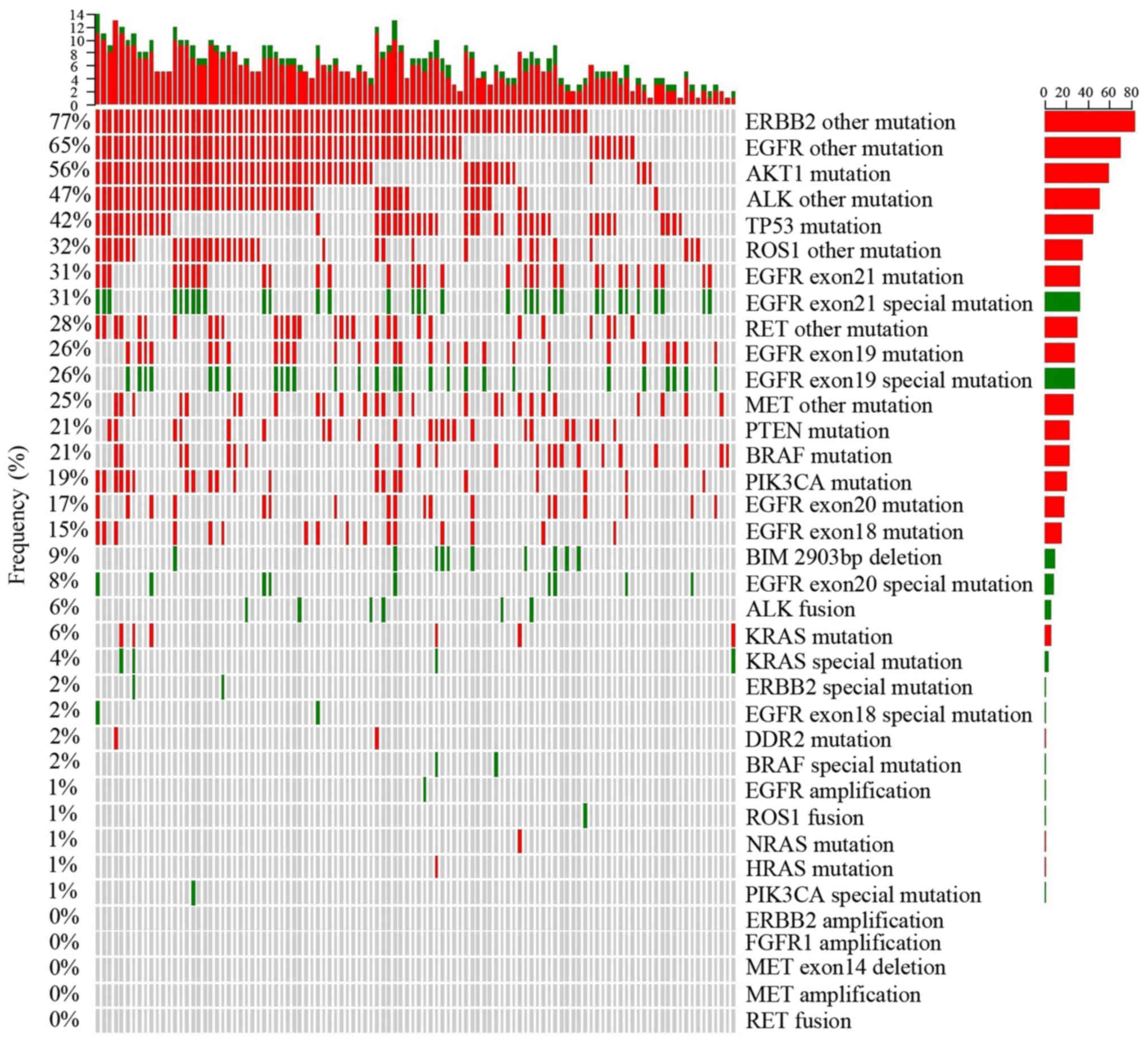
(Gilotrif) treatment. Special ERBB2 mutations are noted in Fig. 1 in green, which indicate that the
mutation is associated with a therapeutic agent. In addition to
these two cases of ERBB2 alterations, 83 patients (76.8%) were
identified as harboring other ERBB2 mutations of unknown present
significance, annotated as ‘ERBB2 other mutations’ in Fig. 1. Collectively, these unknown
mutations were observed more frequently compared with all other
mutations.
EGFR mutations were first identified as NSCLC driver
oncogenes by three independent groups in 2004 (50–52). In
the present study, analysis of 108 patients with MPE, demonstrated
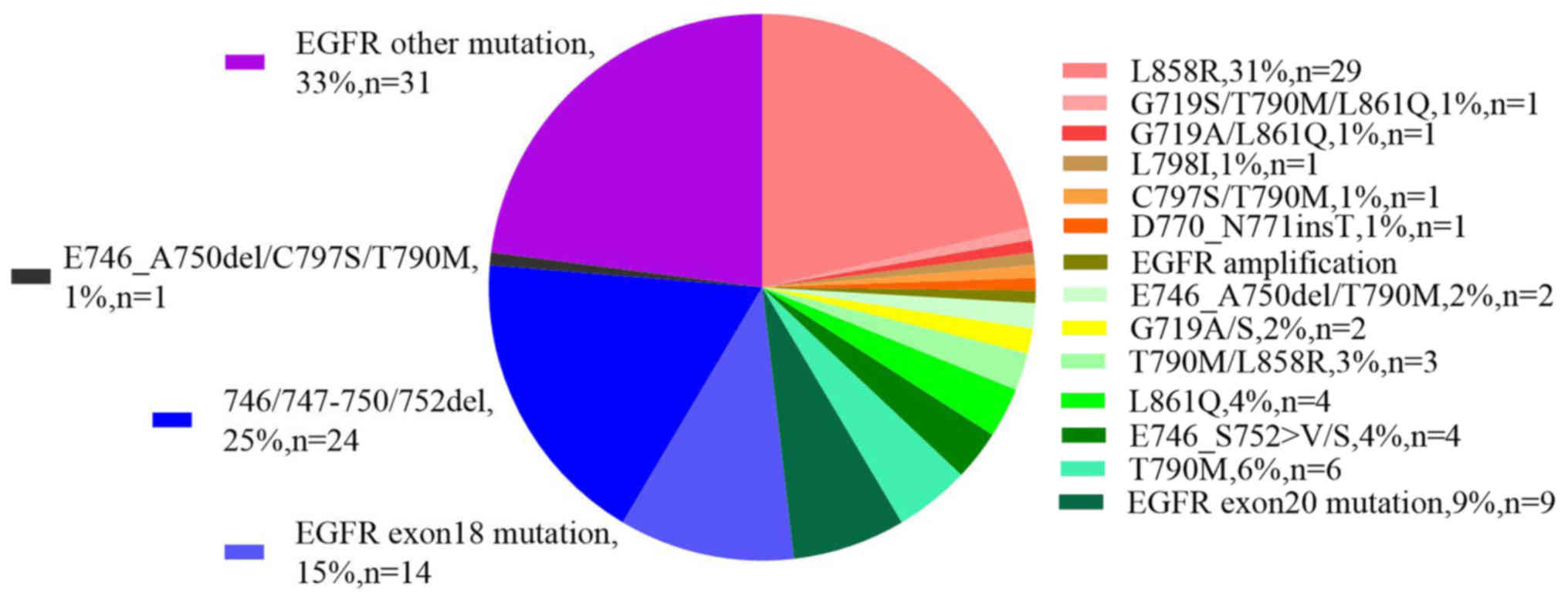
that 93 patients (86%) harbored EGFR mutations, the breakdown by
type of which is shown in Fig. 2 (or
Table SII). In particularly, 16
patients harbored mutations in EGFR exon 18, among which, only two
women possessed the G719A/G719S alterations. A total of 28 patients
(30%) were found to harbor exon 19 alterations, 24 of which were
deletion mutations, primarily in the KELREATS sequence, whereas
only one deletion was observed in the TSPKANKE sequence. A total of
3 patients exhibited a E746_S752>V mutation and 1 patient had a
L747_P753>S alteration on exon 19 of EGFR. A total of 18
abnormalities on exon 20 of EGFR were identified, among which, 1
patient had a L798I mutation, one had a T790M/C797S double
alteration (cis relationship), six had a T790M mutation and only
one had an insertion of threonine between D770 and N771. A total of
33 patients (35.5%) harbored mutations on exon 21, including L858R
(n=29) and L861Q (n=4). There was only one case of EGFR
amplification that simultaneously harbored a L858R mutation.
Altogether, 62 patients (66.7%) had EGFR mutations that are
associated with sensitivity to certain agents, such as icotinib,
gefitinib, erlotinib, afatinib and osimertinib. In addition to
these mutations, 31 patients (33.3%) possessed EGFR alterations
outside of exons 18–21 which do not currently have an available
targeted therapy (Fig. 2). It was
also observed that 15 patients possessed a wild type EGFR gene
among the 108 MPE samples.
AKT1 is a serine-threonine protein kinase that is
critical for transmitting growth-promoting signals, most likely via
the IGF1 receptor (53). An E17K
mutation of AKT1 is associated with AKT1 sensitivity to the
inhibitor, uprosertib (53). In the
present study the E17K mutation was not observed; however, other
alterations of the AKT1 gene were observed in 60 patients (55.6%)
(Fig. 1). The TP53 gene is the most
frequently mutated gene in cancer, indicating that TP53 serves a
crucial tumor suppressor role (54).
A total of 45 patients (41.7%) harbored TP53 gene mutations,
including SNVs and frameshifts (Fig.
1). BIM is a pro-apoptotic member of the B-cell CLL/lymphoma 2
(BCL2) family of proteins. A frequently observed intronic deletion
(2,903 bp) polymorphism in BIM is sufficient to confer intrinsic
tyrosine kinase inhibitor (TKI) resistance (55). This intronic deletion was identified
in 10 patients (9%) (Fig. 1). BRAF,
a human gene which encodes the B-Raf protein, is a member of the
Raf kinase family of growth signal transduction protein kinases
(56). In the present study, 23
patients (21.3%) harbored BRAF mutations, including two cases of
the N581I mutations, which are sensitive to Solafini (57). In 6 patients, KRAS mutations were
observed, four of whom had different mutations; G12D, G12S, G13C
and A146T. In addition, one mutation occurred in HRAS, and one in
NRAS, but these two mutations belonged to variants of unknown
significance (Fig. 1). PIK3CA
participates in a complex interaction within the tumor
microenvironment (58). The present
study demonstrated that 21 patients (19.4%) harbored PIK3CA
mutations, but only one patient harbored a E545K mutation, which is
sensitive to Sirolimus and Ivimos (59) (Fig.
1). PTEN acts as a tumor suppressor gene through its
phosphatase activity (60), and in
the present study, 23 patients (21.3%) exhibited PTEN mutations
(Fig. 1). DDR2 serves a key role in
the communication of cells with their microenvironment (61). In the present study, 2 patients
harbored DDR2 mutations (Fig. 1). No
amplifications of the FGFR1 gene were observed, but 20 patients
(18.5%) possessed SNVs in this gene (Fig. 1). There were no MET amplifications or
exon 14 skips among the samples, but 27 patients (25%) had SNVs of
unknown significance in the MET gene (Fig. 1). Additionally, no RET fusions were
detected; however, there were 30 patients (27.8%) with SNVs of
unknown significance in the RET gene (Fig. 1).
There was one case of an ROS1-CD74 fusion, where
ROS1 intron 33 and CD74 intron 6 were fused in a patient of 34
years old. This fusion resulted in the formation of a new gene, and
the corresponding sequences are listed in Table SIII. Meanwhile, 35 patients (32.4%)
exhibited SNVs of unknown significance in ROS1 (Fig. 1).
Overall, 6 cases (5.6%) of ALK-EML4 fusions, in 1
man and 5 women, were observed. Table
SIII shows the corresponding sequences, in particularly, a man
(77 years old) demonstrated gene fusion between ALK exon 20, and
EML4 intron 13. Meanwhile, 5 women possessed gene fusion between
ALK intron 19, and different EML4 introns (three cases of intron 6,
one case of intron 2, and one case of intron 20). A total of 51
patients (47.2%) possessed SNVs in the ALK gene, which have no
known significance at present.
Among MPE samples from 108 patients, there was only
one person without sex or age information, and this patient had
mutations of E746_A750 deletion, and T790M in the EGFR gene, as
well as TP53 abnormalities (Table
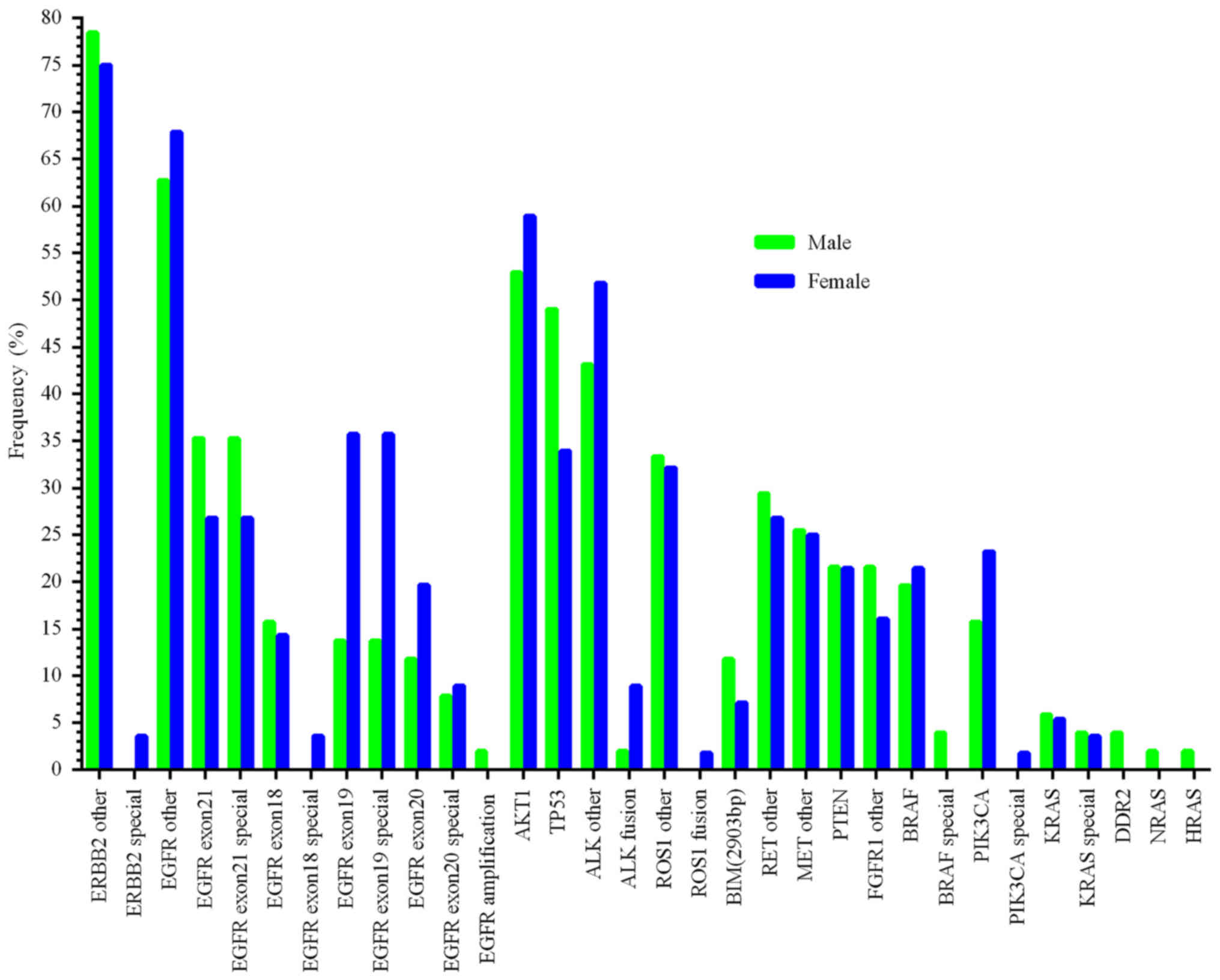
SII). Multiplexed molecular profiling in men (n=51), and women
(n=56) is shown in Fig. 3. The
mutation rate in females was higher than in males in the ERBB2
special mutations, EGFR exon 18 special mutations, EGFR exon 19
special mutations, ALK fusions, ROS1 fusions, and PIK3CA special
mutations. The abnormalities in males which were higher compared
with females were EGFR exon 21 special mutations, BIM, TP53
mutations, and BRAF special mutations. The rate of EGFR exon 20
special mutations and KRAS special mutations were ~6%, similar
between men and women (Fig. 3). In
particular, there were 36 female patients (64.3%) harboring EGFR
mutations with known significance, higher than in males
(50.9%).
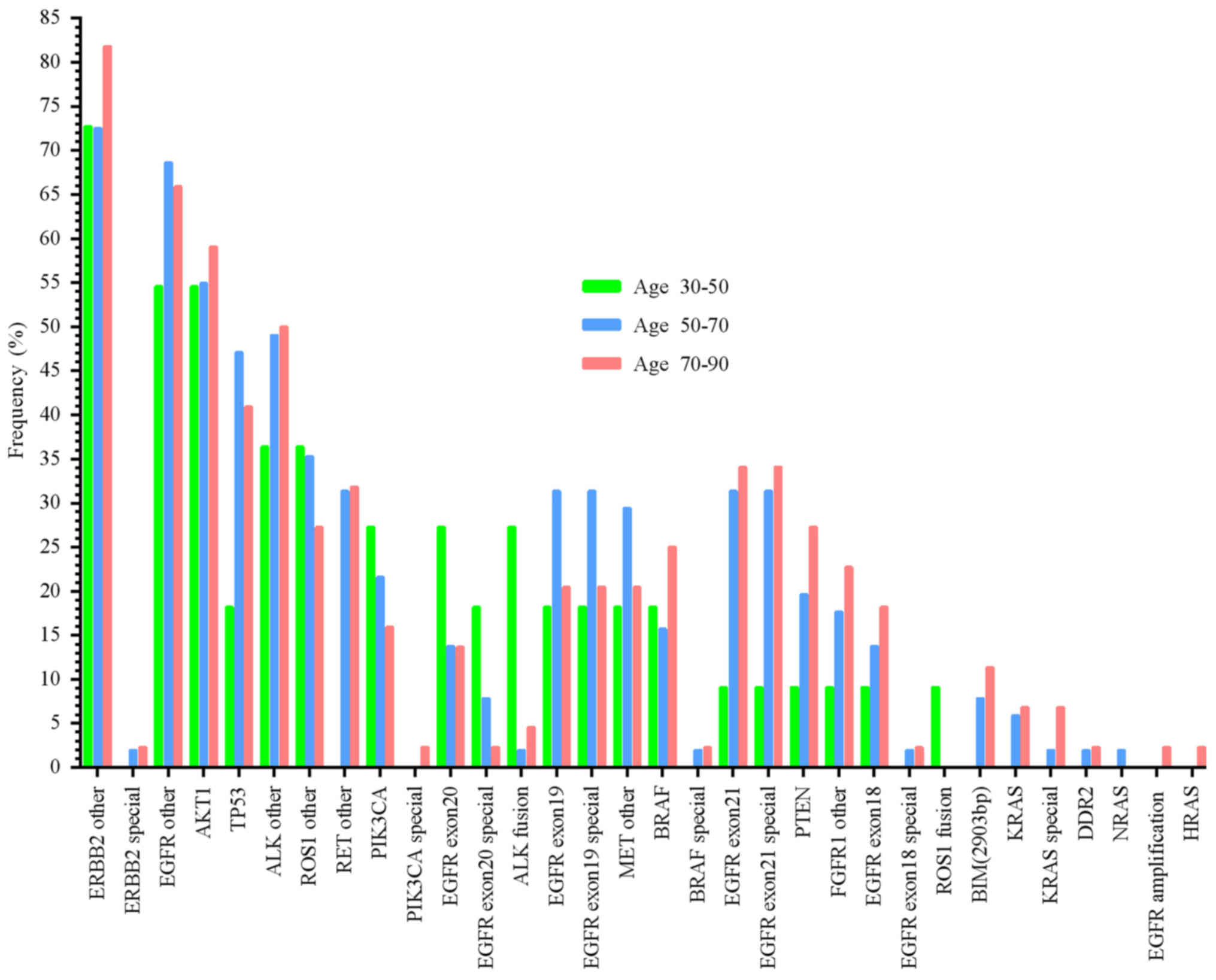
As mentioned above, one patient without age or sex
information harbored an E746_A750 deletion, and T790M mutations in
the EGFR gene and TP53 abnormalities. Another male patient's age
information was not available. The mutation distributions in
different ages are presented in Fig.
4. These results demonstrate that some mutation rates increased
with age, including ERBB2 special mutations, PIK3CA special
mutations, BRAF special mutations, EGFR exon 21 mutations, EGFR
exon 21 special mutations, PTEN mutations, FGFR1 other mutations,
EGFR exon 18 mutations, EGFR exon 18 special mutations, BIM
mutations, KRAS mutations, and KRAS special mutations. In contrast,
other mutation frequencies decreased with age, for example the
PIK3CA mutations, EGFR exon 20 special mutations and ROS1 fusions.
No significant difference in the other mutation rates and age were
observed (Fig. 4).
MPE, a common cause of symptoms, hospitalizations
and morbidities in patients with disseminated lung cancer, is a
cause of the lethal outcomes in various types of cancer originating
from the lung (20,62), breast (20), and metastasizes to the pleural cavity
(63). Increased tumor burden within
the pleural space is associated with reduced overall survival in
patients (64–66). However, the reasons why certain
patients with pleural tumors develop MPE, whereas others do not
remain unknown. In 2010, Stathopoulos et al (67) used two different models to
demonstrate that host-derived IL-5 promotes experimental MPE and
may be involved in the pathogenesis of human MPE. Stathopoulos
et al found that nuclear factor-κB affected tumor
progression in a mouse model of MPE by injecting Lewis lung cancer
cells directly into the pleural space of syngeneic C57B/6 mice
(68).
Varying types of mutations within certain genes may
result in proteins with a different conformation, thus providing
new insights into mutation-induced drug resistance and/or
sensitivity mechanisms, and conformational transitions connecting
active and/or inactive states (92–94).
Furthermore, these conformations are critical for
ligand-independent EGFR activation and downstream signaling
(95).
Accurate identification of predictive genetics is
crucial not just for patient therapy but also for increasing our
knowledge of treatment-induced tumor evolution. Thus far,
researchers have illustrated the feasibility of oncogene analysis
in MPE patient samples with advanced lung cancer (25,28–38).
However, these targeted identification approaches, for example
Sanger sequencing, ARMS-PCR, PNA clamping, or HRM analysis are
predominantly PCR-based methods, therefore are only suitable for
detecting mutations in small regions of DNA. The primary limitation
of these methods is that they require multiple PCRs and an adequate
amount of DNA. In addition, their sensitivity does not exceed 1:100
(14). Previously published studies
have investigated the use of molecular profiling of advanced lung
cancer samples with MPE using NGS (39,45).
These studies showed that EGFR mutation frequency was 80% (29/36
patients) (39) and 73% (22/30
patients) (45). However, the number
of enrolled patients with MPE was not sufficient (30–36
individuals) and the average sequencing depth on target was only
359X (45). In the present study,
108 patients with MPE were recruited between December 2017 and July
2018, and high-quality purified DNA was extracted from cell pellets
obtained from pleural effusions. Higher quality specimens, DNA,
higher quality libraries, more robust quality methods (for example,
sequences with Q<30 were removed; somatic mutations with ≥2%
mutant allele frequency, and with at least 20 supporting reads) and
controls are required to quantify the NGS results with greater
accuracy to reduce false negative and false positive detections.
The present study utilized the hybridization capture-based assay
(48) and the capture efficiency of
YunYing's optimized probes was ~65%, which is superior to Agilent
SureSelect, NimbleGen SeqCap EZ, or Illumina TruSeq Capture
(96). This higher capture
efficiency vastly reduced false negative NGS results. In addition,
raw data was screened with a 2% threshold for the mutant allele
frequency at every mutant site and most of these sites had at least
10 supporting reads, which greatly reduced the effects of false
positives.
Activating mutations in EGFR are the most well-known
among lung adenocarcinomas, which are associated with therapeutic
agents, and have been described in 15–60% of lung cancer cases in
different studies (11,97–103).
The two most common mutations of EGFR in lung cancer are exon 19
deletions (60%) and the L858R point mutation (35%) (104–108).
A retrospective single-center study reported that the frequency of
these specific EGFR mutations was higher in patients with MPE
compared with those without MPE in patients with stage IV lung
cancer (109). In the present
study, 93 patients (86%) with MPE harbored EGFR mutations (Table SII), and molecular profiling of the
mutation distribution within these 93 EGFR-positive patients is
shown in Fig. 2. Among these 93
patients, 31 (33.3%) presented with mutations holding no known
significance, including the rare mutations within exons 18–21 and
mutations outside exons 18–21. In total, 29 (31%) patients
possessed the L858R mutation, which was the most common mutation.
In 2015, Tsai et al (110)
reported that the expression of EGFR-L858R in lung cancer cells
resulted in the upregulation of CXCR4 using in vitro and
in vivo experiments, upregulation of CXCR4 is associated
with increased cancer cell invasive ability, promoting subsequent
MPE formation. In the present study, the indel mutation in exon 19
was the second most commonly observed mutation among all mutations
with 24 patients (25.8%) harboring exon 19 indel mutations. Other
studies demonstrated that the EGFR exon 19 deletion in lung cancer
cell lines resulted in high basal levels of MYC and HIF-1α
expression, which contributed to tumor angiogenesis and may
increase the probability of MPE formation (62,111).
The results of the present study indicate that higher EGFR mutation
frequency was associated with increased tendency for MPE. Overall,
in the present study, 62 patients exhibited mutations within EGFR
exons 18–21, who were treated with TKIs.
Pleural metastases are more frequently observed in
patients with lung adenocarcinoma compared with patients with wild
type KRAS (117,118). Previously, Agalioti et al
(119) demonstrated that
KRAS-mutant cells disseminated into the pleural cavity recruited
splenic mast cells, and CD11b + Gr1+ myeloid cells from bone marrow
to the pleural space via CCL2-CCR2 signaling, which promoted the
formation of MPE. The analysis of the present study identified 6
patients harboring KRAS mutations, only four of whom exhibited
mutations of glycine or alanine, for which there are available
treatment agents.
The BIM polymorphism has only been observed in East
Asian populations, to the best of our knowledge (120). A 2,903-bp deletion was discovered
in NSCLC cancer at a frequency of 12–18% using PCR (120–126).
Several studies have reported that the BIM deletion polymorphism
confers intrinsic resistance to EGFR-TKIs in cell lines (55,121–124).
However, other studies have reported that the BIM deletion
polymorphism did not account for intrinsic resistance to EGFR-TKIs
(120,125,126),
notably for MPE in patients with lung adenocarcinoma (120). The present study also suggested
that lung cancer development was not completely dependent upon the
BIM pathway. NGS analysis in the present study of MPE samples
demonstrated that 10 patients (9.2%) possessed the BIM
polymorphism, but the role of this mutation in the development or
treatment of lung cancer remains unclear.
In patients with lung cancer, there is a consensus
among studies that EGFR mutations are more frequent in female than
in male patients (127–131). In the present study, the EGFR
mutant frequency in female patients was 64.3% (36/56 patients),
higher than in male patients, 50.9% (26/51 patients). This was
consistent with previous studies, but EGFR exon 21 special
mutations, BIM mutations, TP53 and BRAF special mutations were
higher in males than in females in the present study.
Aging is a major risk factor for the development of
cancer. The incidence of cancer is positively associated with age
and is relatively rare in younger individuals, except for leukemia
(132). Aging and cancer either
share or diverge with respect to several disease mechanisms
(132). Such mechanisms include the
role of genomic instability, telomere attrition, epigenetic
changes, loss of proteostasis, decreased nutrient sensing and
altered metabolism, but also cellular senescence and stem cell
function. Cancer cells and aged cells are also fundamentally
different, as cancer cells can be thought of as hyperactive cells
with advantageous mutations, rapid cell division and increased
energy consumption, whereas aged cells are hypoactive with
accumulated disadvantageous mutations, cell division inability and
a decreased ability for energy production and consumption. A
previous study investigating MPE from lung adenocarcinoma
demonstrated that fewer Asian patients aged ≤50 years possessed
EGFR mutations, but the EGFR mutation types observed were more
uncommon (127). Most mutation
rates observed in the NGS results in the present study increased
with age, but the frequencies of other mutations decreased with
age, for example, PIK3CA, EGFR exon 20 special mutation and ROS1
fusions.
The present study has certain limitations.
Therapeutic information for the 108 patients was not available.
Additionally, there were no control specimens for comparison of
pleural effusion.
In conclusion, multiplexed molecular profiling of
MPE from lung cancer using NGS was investigated, and due to the
higher capture efficiency and deeper sequencing depth of NGS, MPE
may be a reliable specimen for NGS detection of somatic mutations
using NGS.
Not applicable.
The present study was supported by the National
Natural Science Foundation of China (grant no. 81472199) and by the
National Natural Science Foundation of Jiangsu Province of China
(grant no. BK20141162).
All data generated or analyzed during this study are
included in this published article.
YS and XR designed the study and the experiments. MY
contributed to the conception of the study. WW and JY were
responsible for data collection and the extraction of DNA. DZ and
ZG analyzed the data. YS, XR and MY drafted the manuscript. All
authors read, critically revised, and approved the final
manuscript.
Written informed consent was obtained from all
participants and the present study was approved by the
Institutional Review Board of Affiliated Changzhou No. 2 People's
Hospital (Changzhou, China; approval no. 201400101).
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Spiro SG and Silvestri GA: One hundred
years of lung cancer. Am J Respir Crit Care Med. 172:523–529. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular profiling of lung adenocarcinoma. Nature.
511:543–550. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cancer Genome Atlas Research Network, .
Comprehensive genomic characterization of squamous cell lung
cancers. Nature. 489:519–525. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Imielinski M, Berger AH, Hammerman PS,
Hernandez B, Pugh TJ, Hodis E, Cho J, Suh J, Capelletti M,
Sivachenko A, et al: Mapping the hallmarks of lung adenocarcinoma
with massively parallel sequencing. Cell. 150:1107–1120. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Govindan R, Ding L, Griffith M,
Subramanian J, Dees ND, Kanchi KL, Maher CA, Fulton R, Fulton L,
Wallis J, et al: Genomic landscape of non-small cell lung cancer in
smokers and never-smokers. Cell. 150:1121–1134. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Campbell JD, Alexandrov A, Kim J, Wala J,
Berger AH, Pedamallu CS, Shukla SA, Guo G, Brooks AN, Murray BA, et
al: Distinct patterns of somatic genome alterations in lung
adenocarcinomas and squamous cell carcinomas. Nat Genet.
48:607–616. 2016. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Weinstein IB and Joe A: Oncogene
addiction. Cancer Res. 68:3077–3080; discussion 3080. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Inamura K: Lung Cancer: Understanding its
molecular pathology and the 2015 WHO classification. Front Oncol.
7:1932017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kohno T, Nakaoku T, Tsuta K, Tsuchihara K,
Matsumoto S, Yoh K and Goto K: Beyond ALK-RET, ROS1 and other
oncogene fusions in lung cancer. Transl Lung Cancer Res. 4:156–164.
2015.PubMed/NCBI
|
|
13
|
Tan L, Alexander M, Officer A, MacManus M,
Mileshkin L, Jennens R, Herath D, de Boer R, Fox SB, Ball D and
Solomon B: Survival difference according to mutation status in a
prospective cohort study of Australian patients with metastatic
non-small-cell lung carcinoma. Intern Med J. 48:37–44. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Han Y and Li J: Sample types applied for
molecular diagnosis of therapeutic management of advanced non-small
cell lung cancer in the precision medicine. Clin Chem Lab Med.
55:1817–1833. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Molina JR, Yang P, Cassivi SD, Schild SE
and Adjei AA: Non-small cell lung cancer: Epidemiology, risk
factors, treatment, and survivorship. Mayo Clin Proc. 83:584–594.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Diaz LA Jr and Bardelli A: Liquid
biopsies: Genotyping circulating tumor DNA. J Clin Oncol.
32:579–586. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Heitzer E, Ulz P and Geigl JB: Circulating
tumor DNA as a liquid biopsy for cancer. Clin Chem. 61:112–123.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Masters GA, Krilov L, Bailey HH, Brose MS,
Burstein H, Diller LR, Dizon DS, Fine HA, Kalemkerian GP, Moasser
M, et al: Clinical cancer advances 2015: Annual report on progress
against cancer from the American society of clinical oncology. J
Clin Oncol. 33:786–809. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Froudarakis ME: Pleural effusion in lung
cancer: More questions than answers. Respiration. 83:367–376. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Roberts ME, Neville E, Berrisford RG,
Antunes G and Ali NJ; BTS Pleural Disease Guideline Group, :
Management of a malignant pleural effusion: British thoracic
society pleural disease guideline 2010. Thorax. 65 (Suppl
2):ii32–ii40. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen YL, Lee CT, Lu CC, Yang SC, Chen WL,
Lee YC, Yang CH, Peng SL, Su WC, Chow NH and Ho CL: Epidermal
growth factor receptor mutation and anaplastic lymphoma kinase gene
fusion: Detection in malignant pleural effusion by RNA or PNA
analysis. PLoS One. 11:e01581252016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zarogoulidis K, Zarogoulidis P, Darwiche
K, Tsakiridis K, Machairiotis N, Kougioumtzi I, Courcoutsakis N,
Terzi E, Zaric B, Huang H, et al: Malignant pleural effusion and
algorithm management. J Thorac Dis. 5 (Suppl 4):S413–S419.
2013.PubMed/NCBI
|
|
23
|
Akamatsu H, Koh Y, Kenmotsu H, Naito T,
Serizawa M, Kimura M, Mori K, Imai H, Ono A, Shukuya T, et al:
Multiplexed molecular profiling of lung cancer using pleural
effusion. J Thorac Oncol. 9:1048–1052. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Agalioti T, Giannou AD and Stathopoulos
GT: Pleural involvement in lung cancer. J Thorac Dis. 7:1021–1030.
2015.PubMed/NCBI
|
|
25
|
Tsai TH, Wu SG, Hsieh MS, Yu CJ, Yang JC
and Shih JY: Clinical and prognostic implications of RET
rearrangements in metastatic lung adenocarcinoma patients with
malignant pleural effusion. Lung Cancer. 88:208–214. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tiran V, Stanzer S, Heitzer E, Meilinger
M, Rossmann C, Lax S, Tsybrovskyy O, Dandachi N and Balic M:
Genetic profiling of putative breast cancer stem cells from
malignant pleural effusions. PLoS One. 12:e01752232017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Al-Hajj M, Wicha MS, Benito-Hernandez A,
Morrison SJ and Clarke MF: Prospective identification of
tumorigenic breast cancer cells. Proc Natl Acad Sci USA.
100:3983–3988. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jian G, Songwen Z, Ling Z, Qinfang D, Jie
Z, Liang T and Caicun Z: Prediction of epidermal growth factor
receptor mutations in the plasma/pleural effusion to efficacy of
gefitinib treatment in advanced non-small cell lung cancer. J
Cancer Res Clin Oncol. 136:1341–1347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Han HS, Eom DW, Kim JH, Kim KH, Shin HM,
An JY, Lee KM, Choe KH, Lee KH, Kim ST, et al: EGFR mutation status
in primary lung adenocarcinomas and corresponding metastatic
lesions: Discordance in pleural metastases. Clin Lung Cancer.
12:380–386. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wu SG, Gow CH, Yu CJ, Chang YL, Yang CH,
Hsu YC, Shih JY, Lee YC and Yang PC: Frequent epidermal growth
factor receptor gene mutations in malignant pleural effusion of
lung adenocarcinoma. Eur Respir J. 32:924–930. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhang X, Zhao Y, Wang M, Yap WS and Chang
AY: Detection and comparison of epidermal growth factor receptor
mutations in cells and fluid of malignant pleural effusion in
non-small cell lung cancer. Lung Cancer. 60:175–182. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kimura H, Fujiwara Y, Sone T, Kunitoh H,
Tamura T, Kasahara K and Nishio K: EGFR mutation status in
tumour-derived DNA from pleural effusion fluid is a practical basis
for predicting the response to gefitinib. Br J Cancer.
95:1390–1395. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wu SG, Yu CJ, Tsai MF, Liao WY, Yang CH,
Jan IS, Yang PC and Shih JY: Survival of lung adenocarcinoma
patients with malignant pleural effusion. Eur Respir J.
41:1409–1418. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Carter J, Miller JA, Feller-Kopman D,
Ettinger D, Sidransky D and Maleki Z: Molecular profiling of
malignant pleural effusion in metastatic non-small-cell lung
carcinoma. The effect of preanalytical factors. Ann Am Thorac Soc.
14:1169–1176. 2017.PubMed/NCBI
|
|
35
|
Lin J, Gu Y, Du R, Deng M, Lu Y and Ding
Y: Detection of EGFR mutation in supernatant, cell pellets of
pleural effusion and tumor tissues from non-small cell lung cancer
patients by high resolution melting analysis and sequencing. Int J
Clin Exp Pathol. 7:8813–8822. 2014.PubMed/NCBI
|
|
36
|
Yang J, Lee OJ, Son SM, Woo CG, Jeong Y,
Yang Y, Kwon J, Lee KH and Han HS: EGFR mutation status in lung
adenocarcinoma-associated malignant pleural effusion and efficacy
of EGFR tyrosine kinase inhibitors. Cancer Res Treat. 50:908–916.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yeo CD, Kim JW, Kim KH, Ha JH, Rhee CK,
Kim SJ, Kim YK, Park CK, Lee SH, Park MS and Yim HW: Detection and
comparison of EGFR mutations in matched tumor tissues, cell blocks,
pleural effusions, and sera from patients with NSCLC with malignant
pleural effusion, by PNA clamping and direct sequencing. Lung
Cancer. 81:207–212. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Han HS, Lim SN, An JY, Lee KM, Choe KH,
Lee KH, Kim ST, Son SM, Choi SY, Lee HC and Lee OJ: Detection of
EGFR mutation status in lung adenocarcinoma specimens with
different proportions of tumor cells using two methods of
differential sensitivity. J Thorac Oncol. 7:355–364. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Buttitta F, Felicioni L, Del Grammastro M,
Filice G, Di Lorito A, Malatesta S, Viola P, Centi I, D'Antuono T,
Zappacosta R, et al: Effective assessment of egfr mutation status
in bronchoalveolar lavage and pleural fluids by next-generation
sequencing. Clin Cancer Res. 19:691–698. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Biankin AV, Piantadosi S and Hollingsworth
SJ: Patient-centric trials for therapeutic development in precision
oncology. Nature. 526:361–370. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Celesti F, Celesti A, Wan J and Villari M:
Why deep learning is changing the way to approach NGS data
processing: A review. IEEE Rev Biomed Eng. 11:68–76. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kamps R, Brandão RD, Bosch BJ, Paulussen
AD, Xanthoulea S, Blok MJ and Romano A: Next-generation sequencing
in oncology: Genetic diagnosis, risk prediction and cancer
classification. Int J Mol Sci. 18:E3082017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhu YC, Zhou YF, Wang WX, Xu CW, Zhuang W,
Du KQ and Chen G: CEP72-ROS1: A novel ROS1 oncogenic fusion variant
in lung adenocarcinoma identified by next-generation sequencing.
Thorac Cancer. 9:652–655. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhang X, Li Y, Liu C, Wang W, Li M, Lv D,
Sun G, Chen H, Dong X, Miao Z, et al: Identification of a novel
KIF13A-RET fusion in lung adenocarcinoma by next-generation
sequencing. Lung Cancer. 118:27–29. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Liu L, Shao D, Deng Q, Tang H, Wang J, Liu
J, Guo F, Lin Y, Peng Z, Mao M, et al: Next generation
sequencing-based molecular profiling of lung adenocarcinoma using
pleural effusion specimens. J Thorac Dis. 10:2631–2637. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
R Core Team, . A language and environment
for statistical computing. R Foundation for Statistical Computing;
Vienna, Austria: 2014, http://www.R-project.org/
|
|
47
|
RStudio Team, . RStudio: Integrated
Development for R. RStudio, Inc., Boston, MA, 2015. http://www.rstudio.com/
|
|
48
|
Bai H, Xia J, Zhao X, Gong Z, Zhang D and
Xiong L: Detection of EGFR mutations using target capture
sequencing in plasma of patients with non-small-cell lung cancer. J
Clin Pathol. 72:379–385. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Chmielecki J, Ross JS, Wang K, Frampton
GM, Palmer GA, Ali SM, Palma N, Morosini D, Miller VA, Yelensky R,
et al: Oncogenic alterations in ERBB2/HER2 represent potential
therapeutic targets across tumors from diverse anatomic sites of
origin. Oncologist. 20:7–12. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Pao W, Miller V, Zakowski M, Doherty J,
Politi K, Sarkaria I, Singh B, Heelan R, Rusch V, Fulton L, et al:
EGF receptor gene mutations are common in lung cancers from ‘never
smokers’ and are associated with sensitivity of tumors to gefitinib
and erlotinib. Proc Natl Acad Sci USA. 101:13306–13311. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Hyman DM, Smyth LM, Donoghue MTA, Westin
SN, Bedard PL, Dean EJ, Bando H, El-Khoueiry AB, Pérez-Fidalgo JA,
Mita A, et al: AKT Inhibition in Solid Tumors With AKT1 Mutations.
J Clin Oncol. 35:2251–2259. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Kim J, Yu L, Chen W, Xu Y, Wu M, Todorova
D, Tang Q, Feng B, Jiang L, He J, et al: Wild-type p53 promotes
cancer metabolic switch by inducing PUMA-dependent suppression of
oxidative phosphorylation. Cancer Cell. 35:191–203.e8. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Ng KP, Hillmer AM, Chuah CT, Juan WC, Ko
TK, Teo AS, Ariyaratne PN, Takahashi N, Sawada K, Fei Y, et al: A
common BIM deletion polymorphism mediates intrinsic resistance and
inferior responses to tyrosine kinase inhibitors in cancer. Nat
Med. 18:521–528. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
BRAF fusions in clinically advanced
non-small cell lung cancer, . An emerging target for anti-BRAF
therapies. J Clin Oncol. 35 (Suppl. 15):S90722017. View Article : Google Scholar
|
|
57
|
Caris Life Sciences, . BRAF mutations are
potentially targetable alterations in a wide variety of solid
cancers. https://www.carislifesciences.com/documents/braf-mutations-are-potentially-targetable-alterations-in-a-wide-variety-of-solid-cancers/December
2–2016
|
|
58
|
Samuels Y and Waldman T: Oncogenic
mutations of PIK3CA in human cancers. Curr Top Microbiol Immunol.
347:21–41. 2010.PubMed/NCBI
|
|
59
|
Ng PK, Li J, Jeong KJ, Shao S, Chen H,
Tsang YH, Sengupta S, Wang Z, Bhavana VH, Tran R, et al: Systematic
functional annotation of somatic mutations in cancer. Cancer Cell.
33:450–462.e10. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Wang LH, Wu CF, Rajasekaran N and Shin YK:
Loss of tumor suppressor gene function in human cancer: An
overview. Cell Physiol Biochem. 51:2647–2693. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Hammerman PS, Sos ML, Ramos AH, Xu C, Dutt
A, Zhou W, Brace LE, Woods BA, Lin W, Zhang J, et al: Mutations in
the DDR2 kinase gene identify a novel therapeutic target in
squamous cell lung cancer. Cancer Discov. 1:78–89. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Lui MMS, et al: Malignant pleural effusion
from lung cancers with driver mutations. Curr Pulmonol Rep.
7:13–18. 2018. View Article : Google Scholar
|
|
63
|
Davies HE, Mishra EK, Kahan BC, Wrightson
JM, Stanton AE, Guhan A, Davies CW, Grayez J, Harrison R, Prasad A,
et al: Effect of an indwelling pleural catheter vs. chest tube and
talc pleurodesis for relieving dyspnea in patients with malignant
pleural effusion: The TIME2 randomized controlled trial. JAMA.
307:2383–2389. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Sahn SA and Good JT Jr: Pleural fluid pH
in malignant effusions. Diagnostic, prognostic, and therapeutic
implications. Ann Intern Med. 108:345–349. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Heffner JE, Nietert PJ and Barbieri C:
Pleural fluid pH as a predictor of survival for patients with
malignant pleural effusions. Chest. 117:79–86. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Heffner JE, Heffner JN and Brown LK:
Multilevel and continuous pleural fluid pH likelihood ratios for
evaluating malignant pleural effusions. Chest. 123:1887–1894. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Stathopoulos GT, Sherrill TP, Karabela SP,
Goleniewska K, Kalomenidis I, Roussos C, Fingleton B, Yull FE,
Peebles RS Jr and Blackwell TS: Host-derived interleukin-5 promotes
adenocarcinoma-induced malignant pleural effusion. Am J Respir Crit
Care Med. 182:1273–1281. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Stathopoulos GT, Zhu Z, Everhart MB,
Kalomenidis I, Lawson WE, Bilaceroglu S, Peterson TE, Mitchell D,
Yull FE, Light RW and Blackwell TS: Nuclear factor-kappaB affects
tumor progression in a mouse model of malignant pleural effusion.
Am J Respir Cell Mol Biol. 34:142–150. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Stathopoulos GT, Psallidas I, Moustaki A,
Moschos C, Kollintza A, Karabela S, Porfyridis I, Vassiliou S,
Karatza M, Zhou Z, et al: A central role for tumor-derived monocyte
chemoattractant protein-1 in malignant pleural effusion. J Natl
Cancer Inst. 100:1464–1476. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Giannou AD, Marazioti A, Spella M,
Kanellakis NI, Apostolopoulou H, Psallidas I, Prijovich ZM, Vreka
M, Zazara DE, Lilis I, et al: Mast cells mediate malignant pleural
effusion formation. J Clin Invest. 125:2317–2334. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Chen Y, Mathy NW and Lu H: The role of
VEGF in the diagnosis and treatment of malignant pleural effusion
in patients with nonsmall cell lung cancer (Review). Mol Med Rep.
17:8019–8030. 2018.PubMed/NCBI
|
|
72
|
Wu XZ, Zhou Q, Lin H, Zhai K, Wang XJ,
Yang WB and Shi HZ: Immune regulation of toll-like receptor 2
engagement on CD4+ T cells in murine models of malignant
pleural effusion. Am J Respir Cell Mol Biol. 56:342–352. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Stathopoulos GT and Kalomenidis I:
Malignant pleural effusion: Tumor-host interactions unleashed. Am J
Respir Crit Care Med. 186:487–492. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Psallidas I, Stathopoulos GT, Maniatis NA,
Magkouta S, Moschos C, Karabela SP, Kollintza A, Simoes DC, Kardara
M, Vassiliou S, et al: Secreted phosphoprotein-1 directly provokes
vascular leakage to foster malignant pleural effusion. Oncogene.
32:528–535. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Cui R, Takahashi F, Ohashi R, Yoshioka M,
Gu T, Tajima K, Unnoura T, Iwakami S, Hirama M, Ishiwata T, et al:
Osteopontin is involved in the formation of malignant pleural
effusion in lung cancer. Lung Cancer. 63:368–374. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Thomas R, Cheah HM, Creaney J, Turlach BA
and Lee YC: Longitudinal measurement of pleural fluid biochemistry
and cytokines in malignant pleural effusions. Chest. 149:1494–1500.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Ho CC, Liao WY, Wang CY, Lu YH, Huang HY,
Chen HY, Chan WK, Chen HW and Yang PC: TREM-1 expression in
tumor-associated macrophages and clinical outcome in lung cancer.
Am J Respir Crit Care Med. 177:763–770. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Gopinathan G, Milagre C, Pearce OM,
Reynolds LE, Hodivala-Dilke K, Leinster DA, Zhong H, Hollingsworth
RE, Thompson R, Whiteford JR and Balkwill F: Interleukin-6
stimulates defective angiogenesis. Cancer Res. 75:3098–3107. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Yeh HH, Lai WW, Chen HH, Liu HS and Su WC:
Autocrine IL-6-induced Stat3 activation contributes to the
pathogenesis of lung adenocarcinoma and malignant pleural effusion.
Oncogene. 25:4300–4309. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Liu Q, Yu YX, Wang XJ and Wang Z and Wang
Z: Diagnostic accuracy of interleukin-27 between tuberculous
pleural effusion and malignant pleural effusion: A meta-analysis.
Respiration. 95:469–477. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Ye ZJ, Zhou Q, Yin W, Yuan ML, Yang WB,
Xiang F, Zhang JC, Xin JB, Xiong XZ and Shi HZ: Interleukin
22-producing CD4+ T cells in malignant pleural effusion. Cancer
Lett. 326:23–32. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Sriram KB, Relan V, Clarke BE, Duhig EE,
Yang IA, Bowman RV, Lee YC and Fong KM: Diagnostic molecular
biomarkers for malignant pleural effusions. Future Oncol.
7:737–752. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Palaoro LA, Blanco AM, Gamboni M, Rocher
AE and Rotenberg RG: Usefulness of ploidy, AgNOR and
immunocytochemistry for differentiating benign and malignant cells
in serous effusions. Cytopathology. 18:33–39. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Nam HS: Malignant pleural effusion:
Medical approaches for diagnosis and management. Tuberc Respir Dis
(Seoul). 76:211–217. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Light RW: Pleural effusions. Med Clin
North Am. 95:1055–1070. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Jiang B, Wu GP, Zhao YJ and Wang SC:
Transcription expression and clinical significance of TTF-1 mRNA in
pleural effusion of patients with lung cancer. Diagn Cytopathol.
36:849–854. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Woo CG, Son SM, Han HS, Lee KH, Choe KH,
An JY, Man Lee K, Lim YH, Lee HC and Lee OJ: Diagnostic benefits of
the combined use of liquid-based cytology, cell block, and
carcinoembryonic antigen immunocytochemistry in malignant pleural
effusion. J Thorac Dis. 10:4931–4939. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Zhang F, Wang J, Zheng X, Hu L, Chen J,
Jiang F and Wang Y: Clinical value of jointly detection pleural
fluid Midkine, pleural fluid adenosine deaminase, and pleural fluid
carbohydrate antigen 125 in the identification of nonsmall cell
lung cancer-associated malignant pleural effusion. J Clin Lab Anal.
32:e225762018. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Han L, Jiang Q, Yao W, Fu T and Zeng Q:
Thoracic injection of low-dose interleukin-2 as an adjuvant therapy
improves the control of the malignant pleural effusions: A
systematic review and meta-analysis base on Chinese patients. BMC
Cancer. 18:7252018. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Xu L, Wang B, Gao M, Zhang Y, Qi Q, Li T,
Li C, Wang A and Li Y: Intrapleural combination therapy with
lobaplatin and erythromycin for non-small cell lung cancer-mediated
malignant pleural effusion. Thorac Cancer. 9:950–955. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Tseng YH, Ho HL, Lai CR, Luo YH, Tseng YC,
Whang-Peng J, Lin YH, Chou TY and Chen YM: PD-L1 expression of
tumor cells, macrophages, and immune cells in non-small cell lung
cancer patients with malignant pleural effusion. J Thorac Oncol.
13:447–453. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Li Y, Li X, Ma W and Dong Z:
Conformational transition pathways of epidermal growth factor
receptor kinase domain from multiple molecular dynamics simulations
and bayesian clustering. J Chem Theory Comput. 10:3503–3511. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Pan AC, Weinreich TM, Shan Y, Scarpazza DP
and Shaw DE: Assessing the accuracy of two enhanced sampling
methods using EGFR kinase transition pathways: The influence of
collective variable choice. J Chem Theory Comput. 10:2860–2865.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Sutto L and Gervasio FL: Effects of
oncogenic mutations on the conformational free-energy landscape of
EGFR kinase. Proc Natl Acad Sci USA. 110:10616–10621. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Ruan Z and Kannan N: Altered
conformational landscape and dimerization dependency underpins the
activation of EGFR by αC-β4 loop insertion mutations. Proc Natl
Acad Sci USA. 115:E8162–E8171. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Sims D, Sudbery I, Ilott NE, Heger A and
Ponting CP: Sequencing depth and coverage: Key considerations in
genomic analyses. Nat Rev Genet. 15:121–132. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Yu HA, Arcila ME, Rekhtman N, Sima CS,
Zakowski MF, Pao W, Kris MG, Miller VA, Ladanyi M and Riely GJ:
Analysis of tumor specimens at the time of acquired resistance to
EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers.
Clin Cancer Res. 19:2240–2247. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Yang M, Topaloglu U, Petty WJ, Pagni M,
Foley KL, Grant SC, Robinson M, Bitting RL, Thomas A, Alistar AT,
et al: Circulating mutational portrait of cancer: Manifestation of
aggressive clonal events in both early and late stages. J Hematol
Oncol. 10:1002017. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Wang Z, Yang JJ, Huang J, Ye JY, Zhang XC,
Tu HY, Han-Zhang H and Wu YL: Lung adenocarcinoma harboring EGFR
T790M and in trans C797S responds to combination therapy of first-
and third-generation EGFR TKIs and shifts allelic configuration at
resistance. J Thorac Oncol. 12:1723–1727. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Lin YT, Liu YN, Wu SG, Yang JC and Shih
JY: Epidermal growth factor receptor tyrosine kinase
inhibitor-sensitive exon 19 insertion and exon 20 insertion in
patients with advanced non-small-cell lung cancer. Clin Lung
Cancer. 18:324–332.e1. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Ibrahim U, Saqib A and Atallah JP: EGFR
exon 18 delE709_T710insD mutated stage IV lung adenocarcinoma with
response to afatinib. Lung Cancer. 108:45–47. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Rosell R, Moran T, Queralt C, Porta R,
Cardenal F, Camps C, Majem M, Lopez-Vivanco G, Isla D, Provencio M,
et al: Screening for epidermal growth factor receptor mutations in
lung cancer. N Engl J Med. 361:958–967. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Chic N, Mayo-de-Las-Casas C and Reguart N:
Successful treatment with gefitinib in advanced non-small cell lung
cancer after acquired resistance to osimertinib. J Thorac Oncol.
12:e78–e80. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Ganesan P, Ali SM, Wang K, Blumenschein
GR, Esmaeli B, Wolff RA, Miller VA, Stephens PJ, Ross JS, Palmer GA
and Janku F: Epidermal growth factor receptor P753S mutation in
cutaneous squamous cell carcinoma responsive to cetuximab-based
therapy. J Clin Oncol. 34:e34–37. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Costa DB: Kinase inhibitor-responsive
genotypes in EGFR mutated lung adenocarcinomas: Moving past common
point mutations or indels into uncommon kinase domain duplications
and rearrangements. Transl Lung Cancer Res. 5:331–337. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Thress KS, Paweletz CP, Felip E, Cho BC,
Stetson D, Dougherty B, Lai Z, Markovets A, Vivancos A, Kuang Y, et
al: Acquired EGFR C797S mutation mediates resistance to AZD9291 in
non-small cell lung cancer harboring EGFR T790M. Nat Med.
21:560–562. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Zou J, Bella AE, Chen Z, Han X, Su C, Lei
Y and Luo H: Frequency of EGFR mutations in lung adenocarcinoma
with malignant pleural effusion: Implication of cancer biological
behaviour regulated by EGFR mutation. J Int Med Res. 42:1110–1117.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Tsai MF, Chang TH, Wu SG, Yang HY, Hsu YC,
Yang PC and Shih JY: EGFR-L858R mutant enhances lung adenocarcinoma
cell invasive ability and promotes malignant pleural effusion
formation through activation of the CXCL12-CXCR4 pathway. Sci Rep.
5:135742015. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Lee JG and Wu R: Erlotinib-cisplatin
combination inhibits growth and angiogenesis through c-MYC and
HIF-1α in EGFR-mutated lung cancer in vitro and in vivo. Neoplasia.
17:190–200. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Mertens F and Tayebwa J: Evolving
techniques for gene fusion detection in soft tissue tumours.
Histopathology. 64:151–162. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Martinengo C, Poggio T, Menotti M, Scalzo
MS, Mastini C, Ambrogio C, Pellegrino E, Riera L, Piva R, Ribatti
D, et al: ALK-dependent control of hypoxia-inducible factors
mediates tumor growth and metastasis. Cancer Res. 74:6094–6106.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Wang Z, Wu X, Han X, Cheng G, Mu X, Zhang
Y, Cui D, Liu C, Liu D and Shi Y: ALK gene expression status in
pleural effusion predicts tumor responsiveness to crizotinib in
Chinese patients with lung adenocarcinoma. Chin J Cancer Res.
28:606–616. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Liu L, Zhan P, Zhou X, Song Y, Zhou X, Yu
L and Wang J: Detection of EML4-ALK in lung adenocarcinoma using
pleural effusion with FISH, IHC, and RT-PCR methods. PLoS One.
10:e01170322015. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Zhong J, Li X, Bai H, Zhao J, Wang Z, Duan
J, An T, Wu M, Wang Y, Wang S and Wang J: Malignant pleural
effusion cell blocks are substitutes for tissue in EML4-ALK
rearrangement detection in patients with advanced non-small-cell
lung cancer. Cytopathology. 27:433–443. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Raparia K, Villa C, Raj R and Cagle PT:
Peripheral lung adenocarcinomas with KRAS mutations are more likely
to invade visceral pleura. Arch Pathol Lab Med. 139:189–193. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Renaud S, Seitlinger J, Falcoz PE,
Schaeffer M, Voegeli AC, Legrain M, Beau-Faller M and Massard G:
Specific KRAS amino acid substitutions and EGFR mutations predict
site-specific recurrence and metastasis following non-small-cell
lung cancer surgery. Br J Cancer. 115:346–353. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Agalioti T, Giannou AD, Krontira AC,
Kanellakis NI, Kati D, Vreka M, Pepe M, Spella M, Lilis I, Zazara
DE, et al: Mutant KRAS promotes malignant pleural effusion
formation. Nat Commun. 8:152052017. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Wu SG, Liu YN, Yu CJ, Yang PC and Shih JY:
Association of BIM deletion polymorphism with intrinsic resistance
to EGFR tyrosine kinase inhibitors in patients with lung
adenocarcinoma. JAMA Oncol. 2:826–828. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Lee JH, Lin YL, Hsu WH, Chen HY, Chang YC,
Yu CJ, Shih JY, Lin CC, Chen KY, Ho CC, et al: Bcl-2-like protein
11 deletion polymorphism predicts survival in advanced
non-small-cell lung cancer. J Thorac Oncol. 9:1385–1392. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Cardona AF, Rojas L, Wills B, Arrieta O,
Carranza H, Vargas C, Otero J, Corrales-Rodriguez L, Martín C,
Reguart N, et al: BIM deletion polymorphisms in Hispanic patients
with non-small cell lung cancer carriers of EGFR mutations.
Oncotarget. 7:68933–68942. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Xia J, Bai H, Yan B, Li R, Shao M, Xiong L
and Han B: Mimicking the BIM BH3 domain overcomes resistance to
EGFR tyrosine kinase inhibitors in EGFR-mutant non-small cell lung
cancer. Oncotarget. 8:108522–108533. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Zhao M, Zhang Y, Cai W, Li J, Zhou F,
Cheng N, Ren R, Zhao C, Li X, Ren S, et al: The Bim deletion
polymorphism clinical profile and its relation with tyrosine kinase
inhibitor resistance in Chinese patients with non-small cell lung
cancer. Cancer. 120:2299–2307. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Lee JK, Shin JY, Kim S, Lee S, Park C, Kim
JY, Koh Y, Keam B, Min HS, Kim TM, et al: Primary resistance to
epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors
(TKIs) in patients with non-small-cell lung cancer harboring
TKI-sensitive EGFR mutations: An exploratory study. Ann Oncol.
24:2080–2087. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Isobe K, Hata Y, Tochigi N, Kaburaki K,
Kobayashi H, Makino T, Otsuka H, Sato F, Ishida F, Kikuchi N, et
al: Clinical significance of BIM deletion polymorphism in
non-small-cell lung cancer with epidermal growth factor receptor
mutation. J Thorac Oncol. 9:483–487. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Wu SG, Chang YL, Yu CJ, Yang PC and Shih
JY: Lung adenocarcinoma patients of young age have lower EGFR
mutation rate and poorer efficacy of EGFR tyrosine kinase
inhibitors. ERJ Open Res. 3:00092–2016. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Wu M, Pan X, Xu Y, Wu S, Wu X and Chen B:
Methodological comparison of the allele refractory mutation system
and direct sequencing for detecting EGFR mutations in NSCLC, and
the association of EGFR mutations with patient characteristics.
Oncol Lett. 16:1087–1094. 2018.PubMed/NCBI
|
|
129
|
Shi Y, Au JS, Thongprasert S, Srinivasan
S, Tsai CM, Khoa MT, Heeroma K, Itoh Y, Cornelio G and Yang PC: A
prospective, molecular epidemiology study of EGFR mutations in
Asian patients with advanced non-small-cell lung cancer of
adenocarcinoma histology (PIONEER). J Thorac Oncol. 9:154–162.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Tseng CH, Chiang CJ, Tseng JS, Yang TY,
Hsu KH, Chen KC, Wang CL, Chen CY, Yen SH, Tsai CM, et al: EGFR
mutation, smoking, and gender in advanced lung adenocarcinoma.
Oncotarget. 8:98384–98393. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Kota R, Gundeti S, Gullipalli M, Linga VG,
Maddali LS and Digumarti R: Prevalence and outcome of epidermal
growth factor receptor mutations in non-squamous non-small cell
lung cancer patients. Lung India. 32:561–565. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Aunan JR, Cho WC and Soreide K: The
biology of aging and cancer: A brief overview of shared and
divergent molecular hallmarks. Aging Dis. 8:628–642. 2017.
View Article : Google Scholar : PubMed/NCBI
|