Cancer is a major cause of death and one of the most
important global obstacles to improving life expectancy in the 21st
century (1). Despite significant
advances in cancer research, screening and treatment programs,
gastrointestinal (GI) tumors have a high morbidity and mortality
rate worldwide; according to the 2018 global cancer report, the
mortality rate of colorectal cancer was 9.2%, that of gastric
cancer was 8.2% and that of liver cancer was 8.2%, which account
for the top 5 cancer mortality rates in the world (2). The high incidence of cancer in the
digestive system, especially gastric, esophageal and colorectal
cancer (CRC), is a major health burden in Asia, particularly in
East Asia. Asia had the highest rate of CRC cases per 100,000
population (51.8%) and the highest mortality rate (52.4%) in 2018
(3). Additionally, >727,000 cases
of gastric cancer were diagnosed in Asia in 2008, accounting for
11.9% of all confirmed cancer cases (4). Morbidity and mortality rates are also
higher in East Asia than in other parts of the continent (4). China has the highest mortality rate of
gastric cancer (30.1 per 100,000), followed by Japan (20.5 per
100,000) and South Korea (13.8 per 100,000) (4).
Since Bayer AG distributed acetylsalicylic acid as
Aspirin™ in 1899, the drug has cornered the non-steroidal
anti-inflammatory drug (NSAID) market, and with time, aspirin has
become a generic name (5). Recently,
aspirin has received increasing research attention. The
effectiveness of low-dose aspirin (LDA) in preventing ischemic
cardiovascular events has been confirmed (6–8). There
is increasing evidence to support the role that aspirin may play in
chemical protection, especially in patients without cardiovascular
disease (CVD) (9–11). Using aspirin can reduce mortality
rates and the incidence of GI tumors (12). However, aspirin can cause a range of
GI side effects; aspirin taken in large doses has anti-inflammatory
effects similar to those caused by non-selective NSAIDs in the GI
tract (13). LDA is now widely used
for cardiovascular prevention, but even at these very low doses it
is still associated with upper and lower GI damage (14). In the upper GI tract, aspirin causes
a series of adverse GI events, ranging from asymptomatic lesions to
serious complications, such as peptic ulcer bleeding or even death
(15). The link between aspirin and
upper GI damage has been established, but the impact of aspirin on
the lower GI tract remains unclear, although evidence has been
mounting over the past few years (15,16).
The present review focuses on the advances made in
understanding the benefits and the risks of long-term use of
aspirin on the GI tract. To provide evidence for the rational use
of aspirin in clinical practice, the appropriate dose of aspirin to
protect the GI tract is analyzed and summarized.
The main benefit of aspirin in the GI tract is
manifested in the chemoprophylaxis of GI adenoma and numerous types
of cancer, such as CRC, gastric cancer and familial adenomatous
polyposis (FAP). The main pros of aspirin, as will now be
described, are also summarized in Table
I. Additionally, the present review identified that the
chemoprophylaxis dose of aspirin varied among studies. Therefore,
the appropriate preventive doses of aspirin used in different
studies are summarized in Table
I.
Adenomas are the most common polyps of the large
intestine and are a precursor to most CRC (17). The epidemiology of adenomas and CRC
is very similar, hence preventing adenomas can also prevent CRC
(18,19). Sandler et al (20), found that taking 325 mg aspirin daily
reduced the risk of adenomas and delayed progression in individuals
with a CRC history by 10%. However, the aforementioned study
contain bias, as it selected only high-risk patients. Baron et
al (21), conducted another
study in patients who had not previously ha5d CRC and found that 81
mg aspirin daily reduced the risk of recurrent adenomas by 19% in
patients with a recent history of adenomas. In the group
administered 81 mg aspirin daily, there was a >40% reduction in
the risk of advanced disease.
To the best of our knowledge, there are few reports
on the effect of aspirin on FAP, but several studies have reported
that aspirin can lessen the number of adenomas and delay the
development of the disease. In a double-blind, randomized study
where 34 patients with FAP were treated with LDA (100 mg/day) or
placebo post-colectomy, the size of colorectal polyps in patients
with FAP tended to be smaller when treated with LDA (27). In addition, the diameter and number
of polyps were markedly reduced (aspirin:placebo group response
ratio, 2.33:1) and polyp height also decreased (aspirin:placebo
group response ratio, 2:1) (27).
These results demonstrated that aspirin may have an impact on the
relatively early stage of CRC development. However, the
aforementioned study had limitations such as a small sample size
and limited fields of polyp counting, which may have hampered the
detection of responses. Another study by Burn et al
(28), treated patients with FAP
with aspirin (600 mg/day) and/or placebo for 1–12 years and
reported no side effects from aspirin, but also no reduction in
polyps. The differences between these 2 studies may be due to
differences in cohorts of patients and the dose of aspirin
given.
Current research has demonstrated that aspirin does
indeed affect adenomas; aspirin prevented the growth of adenomatous
polyps leading to the regression of existing polyps in several
randomized trials of patients with FAP (27). However, the degree of effect of
aspirin dose on adenoma is still controversial. As there are few
studies on the effect of aspirin on FAP, which are hampered by the
low incidence of the disease (1 in 8,300 at birth) (22) and small patient sample size, further
studies are required to explore and verify their findings.
CRC ranked third in terms of incidence, but second
in terms of mortality rate worldwide in 2018 (2). In patients with CRC with or without
known CVD, there is little debate about the preventive effects of
long-term aspirin use. Considerable experimental evidence supports
this view.
Numerous studies have demonstrated that regular
aspirin use does prevent or reduce CRC mortality rates. The effects
of aspirin may be related to the duration of use. Cea Soriano et
al (29) used The Health
Improvement Network to estimate the incidence of CRC in individuals
without CVD and demonstrated that regular LDA use is associated
with a reduction in the incidence of CRC in individuals without
CVD. In addition, incidence rate ratios demonstrated that starting
LDA at an age of 60–69 or 70–79 years significantly reduced the CRC
risk. However, starting LDA at 80–89 years did not reduce the risk
of CRC. A study that used data from two ongoing prospective
studies, the Nurses' Health Study and the Health Professionals
Follow-up Study, which contained follow-up data for patients with
CRC up to 32 years (30), discovered
a dose-dependent effect of aspirin on CRC, appearing at 0.5–1.5
standard aspirin tablets weekly or the equivalent of a daily dose
of LDA. A combined analysis of dose and duration demonstrated that
the apparent benefit of aspirin use for GI cancer and CRC comes
from taking 0.5–1.5 standard aspirin tablets weekly (30). Regular aspirin use could prevent 33
CRCs/100,000 person-years among individuals who are older >50
years (30).
The majority of studies have demonstrated a
decreasing risk of CRC or adenomas when aspirin therapy is stopped
(31–33). There are different opinions about the
duration of aspirin use. Some studies have demonstrated that this
effect does not appear until 5–10 years later, which is a
considerably delayed effect (34,35).
Gastric cancer was the fifth most commonly diagnosed
cancer in the world and the third leading cause of cancer death in
2018 (2). Among men, it is the most
common cancer in several western Asian countries, including Iran,
Turkmenistan and Kyrgyzstan, and is also the main cause of cancer
death (2).
A previous study using animal experiments suggested
that aspirin may inhibit not only the growth of gastric cancer but
also the migration of cancer cells (36). Li et al (36) used p53−/− mice
(n=20) that were randomly divided into 2 groups to understand the
effects of aspirin on gastric cancer. The aforementioned study
demonstrated that the proliferation capacity of tumor cells in the
experimental group (250 mg/kg aspirin daily added to food) was
significantly reduced compared with that of the control group, and
the number of cells was also markedly reduced.
To the best of our knowledge, there are few specific
studies on the effects of aspirin on gastric cancer. The extent of
the impact of aspirin on gastric cancer seems to be smaller than
that on CRC and colorectal adenoma; in addition, the data are less
comprehensive and more variable. However, it can be concluded from
multi-factor analysis in numerous studies that aspirin can inhibit
the growth of gastric cancer. Two cohort studies have found that
there was a 41% reduction in mortality in patients with gastric
cancer when aspirin was taken (37,38). In
a study involving several randomized controlled trials (RCTs),
reported deaths decreased by 31% in patients with gastric cancer
who took aspirin (P=0.11), and most significant decreases of up to
58% (P=0.007) were observed after 10 years of use (39).
The incidence and mortality of esophageal cancer
were ranked seventh and sixth among all types of cancer,
respectively, in the 2018 global cancer statistics (2). Due to the poor prognosis of esophageal
cancer, treatment options have been highlighted in this section of
the review.
The effect of long-term aspirin use in Barrett's
esophageal cancer has been studied by several clinical trials and
population-based observational studies, suggesting that aspirin may
slow down its progression to both squamous carcinoma and
adenocarcinoma (40–42). Another three independent studies
reported that in patients with esophageal cancer, aspirin had a
remarkable protective effect on all-cause mortality (43–45). In
all three studies, these effects were limited to patients with
esophageal cancer (44) and
esophageal squamous cell carcinoma (43), and in the most recent study (45), when methods to reduce immortal time
bias were employed, the effects were attenuated. A meta-analysis
indicated that aspirin does have a protective effect on esophageal
cancer (including gastric cardia cancer), regardless of squamous
cell or adenocarcinoma type (46).
In addition, in a recent study, in patients with Barrett's
esophageal cancer who did not have a history of NSAID use, aspirin
showed a significant protective effect (47).
However, opposing results were found by a study that
included two large independent population-based cohorts in the UK
(48). The study aforementioned
revealed that long-term aspirin use (75 mg/day) was not associated
with cancer-specific mortality after the diagnosis of esophageal or
gastric cancer (48). These
differences may be due to the aforementioned study investigating
the effects of using aspirin on cancer after a diagnosis of gastric
or esophageal cancer, whereas in other studies, patients were
taking aspirin prior to esophageal or gastric cancer diagnosis.
Aspirin can reduce cancer-related mortality in all
solid cancer types. One study found that this was mainly due to
fewer deaths after 5 years, including significant reductions in
pancreatic cancer deaths (39). In
the aforementioned study, aspirin had a significant effect on
pancreatic cancer death only after >7.5 years of planned
treatment [hazard ratio (HR), 0.28; 95% confidence interval (CI)
0.08–1.00; P=0.04]. Another study found that aspirin use was
associated with a reduced risk of pancreatic ductal adenocarcinoma
incidence in patients with risk factors (OR, 0.48; 95% CI,
0.31–0.67; P<0.001) (49).
Previous studies have suggested that aspirin may
have the potential to prevent liver cancer [including
hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma
(ICC)] (50,51). A prospective cohort study based on
data from 1,084,133 individuals (HCC, n=679; ICC, n=225) from 10
counties in the United States found that aspirin users who took the
drug once a day (>5 years; ≤163 mg) had a 32% reduction in the
risk of liver cancer (52). In
addition, aspirin use reduced ICC risk by 36% in men, but not in
women. For some patients with liver cancer who are at higher risk
of bleeding (due to, for example, cirrhosis of the liver and portal
hypertension with thrombocytopenia), aspirin should be avoided due
to the risk of GI bleeding and renal failure (53). Therefore, the use of aspirin in these
patients remains an important matter and should be investigated
further.
The process by which normal cells turn into cancer
cells is very complex and despite extensive study, the mechanisms
by which aspirin may affect carcinogenesis remain unknown. However,
in the early stages of cancer development, a common feature is that
cells no longer respond to anti-proliferation and -differentiation
signals, instead automatically producing signals to promote growth
(54). The role of aspirin may be
related to these processes.
One of the mechanisms involved in the anticancer
activity of aspirin is commonly thought to be its ability to
inhibit the activity of cyclooxygenase (COX) (55,56).
COX-2 is strongly and rapidly induced in response to growth
factors, cytokines, endotoxins and inflammation, and involves cell
proliferation and the promotion of tumor development (57). As aspirin is a potent inhibitor of
COX-2, it can reduce the production of prostaglandins and other
inflammatory mediators (58). The
deleterious effects of prostaglandins include promoting cell
survival, stimulating cell proliferation and promoting
angiogenesis, which can increase cancer metastasis (59,60).
However, the chemoprophylaxis of aspirin cannot be
explained by inhibiting prostaglandin synthesis only, since some
NSAIDs are still resistant to proliferation in cells that have no
COX activity (61). COX-independent
evidence has also been found in recent years, particularly in
high-dose aspirin (31,62–65),
which has been reported to induce apoptosis through the inhibition
of activation of nuclear factor κB (NF-κB), the upregulation of
tumor suppressor genes, such as TP53, CDKN1A and BAX, and the
downregulation of antiapoptotic genes such as BCL-2 (55). Maintaining homeostasis requires
apoptosis, or programmed cell death, to maintain a dynamic balance
of the total number of cells in a tissue (66). Previous studies (67,68)
reported reduced microsatellite instability and enhanced apoptosis
in mismatch repair (MMR)-deficient cells exposed to aspirin, and
suggested that aspirin may induce genetic selection for
microsatellite stability in a subset of MMR-deficient cells.
Aspirin may delete those aberrant stem cells most likely to
progress rapidly to cancer (69).
Recently, autophagy has been found to play a role in the
chemoprevention of cancer by aspirin. It has been reported that LDA
can induce autophagic death and inhibit the proliferation of
various tumor cells, including HCC and CRC cells (70,71).
Adenosine monophosphate-activated protein kinase (AMPK) can inhibit
the growth and proliferation of tumor cells by affecting autophagy
and inhibiting glycolysis. Recent studies have demonstrated that
aspirin can promote the autophagy and apoptosis of tumor cells by
activating AMPK (72,73). Aspirin can activate AMPK by the
allosteric effect and by inhibiting the dephosphorylation of AMPKα
at the Thr 172 site; AMPKα is an important activator of AMPK
(74).
In addition, it has been reported that aspirin can
stop or delay the growth and mutation of tumor cells instead of
killing them directly. Aspirin can reduce the abnormal accumulation
of genes in cancer tissues (75).
Aspirin may also play a role in the DNA mismatch-repair system, Wnt
signaling, NF-κB signaling and polyamine metabolism (76,77).
Despite several recognized mechanisms of action for the anticancer
effect of aspirin, the exact mechanism remains unknown.
Ulcers are lesions that extend throughout the
thickness of the mucosa and into the submucosa or deeper layers
(83). Evidence of aspirin-induced
peptic ulcers, particularly stomach ulcers began to emerge in the
1960s. Small ulcers are common even at the low doses of aspirin
currently used for cardiovascular protection (78,84). One
trial involving patients from four different countries who took
75–325 mg of aspirin daily for baseline endoscopic evaluation found
that the annualized incidence of new ulcers was 28%, and the
majority of ulcers were in the stomach (78). Another trial found similar rates in
LDA users (84). Helicobacter
pylori (H. pylori) infection and advanced age (>70
years) significantly increased the risk of ulcers (78). Other studies demonstrated that in
NSAID users, H. pylori infection increased the risk of
uncomplicated peptic ulcer by 2–3.5 times and GI bleeding by 2–2.5
times (85–87). Complications of peptic ulcers,
especially the risk of bleeding, are associated with aspirin
(88). A review analyzing studies
published between 1946 and 2015 on the risk between long-term LDA
and GI bleeding found that the incidence of GI bleeding with LDA
was 0.48–3.64 cases per 1,000 person-years (89). A recent study involving healthy
elderly individuals who did not have known CDV found that aspirin
was associated with a notably higher risk of bleeding (90). The main bleeding events involved the
upper GI tract and intracranial hemorrhage. A review of risk
analysis of prophylactic use of aspirin in the general population
demonstrated a significant increase in bleeding and ulcer events at
70 years of age, with long-term aspirin use reducing the risk of
aspirin-related excessive bleeding (87).
Perforation is also a serious GI side effect of
aspirin. A case-control study found that in the general population,
LDA used to prevent CVD conferred a two-fold increased risk of
upper GI perforation (91). Aspirin
had the same effect on the gastric and duodenal sites. The
aforementioned study reported that patients have the greatest risk
of serious GI complications in the first 2 months after starting
aspirin, following which, the risk falls and reaches a plateau at
~6 months. Aspirin is the most important independent risk factor
for perforation of the upper and lower alimentary tract, and a
history of smoking, alcohol consumption, arthritis or peptic ulcers
increases the risk of perforation (92).
The association between LDA use and upper GI
injuries has been well established, but effects of aspirin on the
lower GI tract remain unclear, despite increasing evidence in
recent years. A Japanese study reported that LDA (100 mg)
significantly increased the risk of lower GI bleeding, but the
number of bleeding cases (n=44) was relatively small (93). In a Spanish case-control study
(>1,000 bleeding observations), LDA increased the risk of lower
GI bleeding (including bleeding from the small and large intestine)
by 2.7 times compared with no aspirin use (94). A study in Japan reported that CVD
patients prescribed LDA for >1 year have a high risk of
hemorrhage, but few cases (5/701) of bleeding were observed, so the
CI was large and the finding not statistically significant
(95).
In addition, the association between LDA and the
development of diverticular bleeding and diverticulitis have been
evaluated by several studies (16,96,97). In
Japan, recent prospective research on diverticular disease has
assessed the efficacy of LDA and found a significant association
with diverticular bleeding (97). A
study by health professionals demonstrated an increase in the risk
of diverticular bleeding with LDA (2–5.9 tablets of 325 mg per
week; multivariate HR, 2.32; 95% CI, 1.34–4.02) compared with no
aspirin use (98).
Hepatotoxicity induced by NSAIDs is a rare but
potentially fatal complication that usually occurs within 12 weeks
of initiation of treatment; it can occur in all NSAIDs, but seems
to be more common when diclofenac and sulindac are used (99). Although there are few reports on the
association between aspirin and hepatotoxicity, the side effect of
hepatotoxicity in patients with hepatic dysfunction should be
noted. The patients may present with acute fulminant liver failure
or with no symptoms, but with the biochemical and histological
characteristics of chronic active hepatitis (99). The hepatotoxicity of aspirin is
dose-dependent and generally does not result in liver damage
(75-300 mg/day) unless the full anti-inflammatory doses are used
(99).
In general, the benefits of aspirin to the GI tract
are mainly reflected in cancer prevention. Aspirin can reduce the
incidence of gastric cancer, CRC, colorectal adenoma, live cancer
and pancreatic cancer, and reduce the risk of Barrett's esophageal
progression to esophageal adenocarcinoma. The protective effect of
aspirin on CRC and colorectal adenomas is almost certain,
especially in older adults at risk for CVD. In April 2016, the
United States Preventive Services Task Force formally issued
guidelines recommending LDA (75-100 mg/day) to prevent CVD and CRC
in people aged 50–69 years with CVD risk but no elevated hemorrhage
risk (11). However, the preventive
effect for other GI cancer types is still controversial. The effect
of aspirin on cancer prevention is mainly reflected after 4–5
years, even at low doses. However, a recent study (ASPREE trial)
found that aspirin did not help reduce all-cause mortality (mainly
cancer-related mortality, including GI cancer) (100). There are several possible reasons
why the results of this study differ from those of previous
studies: i) Most previous studies did not regard cancer as a
predefined secondary endpoint, nor did they establish systematic
approaches for the diagnosis and adjudication of cancer endpoints;
and ii) the participants in the aforementioned study were mainly
healthy individuals aged ≥70 years, with a median follow-up of 4.7
years, while previous studies mainly focused on people aged <70
and found that the effects of aspirin take 4–5 years to show. The
other primary prevention trials of aspirin did not find similar
results, suggesting that the deaths reported in the aforementioned
study should be interpreted with caution.
Speculation remains as to the risk-benefit ratio of
long-term aspirin use and the optimal dose required for effective
chemoprevention while minimizing side effects. One of the most
representative studies of the effects of different doses of aspirin
on the risk of GI cancer is that conducted by Rothwell et al
(35). The study found the same
effect for 75–300 mg doses of aspirin with regard to the reduction
of fatal CRC, with 75 mg daily being as effective as higher doses.
The group also observed an absolute risk reduction in colorectal
malignancy of ~1.5% after a 5-year period of treatment with at
least 75 mg aspirin. However, very low doses of aspirin (e.g., 30
mg/day) are associated with a higher risk of fatal CRC compared
with higher doses (34,35). The effective dose of aspirin in order
to obtain the associated benefits of the drug in the GI tract
varies between trials, although some studies have demonstrated that
high-dose aspirin (>500 mg/day) may confer stronger protection
than standard dose regimens (28,101).
As summarized in Table I, numerous
recent trials have challenged this notion, providing evidence for
the use of LDA in cancer prevention. This phenomenon may be related
to the different pharmacokinetics and pharmacodynamics of aspirin
in different environments, and the physiological differences among
patient populations (102,103).
The main harmful effects of aspirin on the digestive
system are bleeding, ulcers, perforation, dyspepsia and discomfort,
while hepatic dysfunction is rare (Table II). One study found that aspirin has
low toxicity and leads to a lower incidence of bleeding in the
upper GI tract, and that it mainly results in dyspepsia. This study
demonstrated that the beneficial effects of aspirin on cancer
outweigh the risk of aspirin-induced bleeding events (104). The main risk factors for bleeding
in aspirin users are age and H. pylori infection (7,105). Age
is a key factor when weighing the pros and cons of aspirin. Once an
individual approaches 60 years old, there is a marked increase in
the risk of aspirin-induced bleeding events, with a non-linear
relationship between increased risk and subsequent age (106,107).
Changing drug formulations would not alleviate the adverse effects
of aspirin on upper GI mucosa, and neither buffer nor
enteric-coated tablets can reduce the risk of massive upper GI
bleeding (107,108). According to previous studies,
long-term LDA use for >4–5 years still plays a role in the
prevention of GI cancer in healthy people aged 55–65 years. Since
aspirin takes 4–5 years to have an effect and there is an increased
risk of GI side effects in people aged >60, the prophylactic use
of aspirin alone in people aged >60 is not recommended. Numerous
studies have demonstrated that proton pump inhibitors (PPI)
significantly reduce the risk of GI adverse events in aspirin
patients (14,89,109–111).
H2-receptor antagonists can also inhibit the secretion of gastric
acid to a certain extent, but their effect may not be as good as
that of PPI preparation (112).
This superiority was observed uniformly in the separate clinical
circumstances in which these agents are used in peptic ulcer
disease, namely the prevention, healing and treatment of acute
upper GI bleeding (113). According
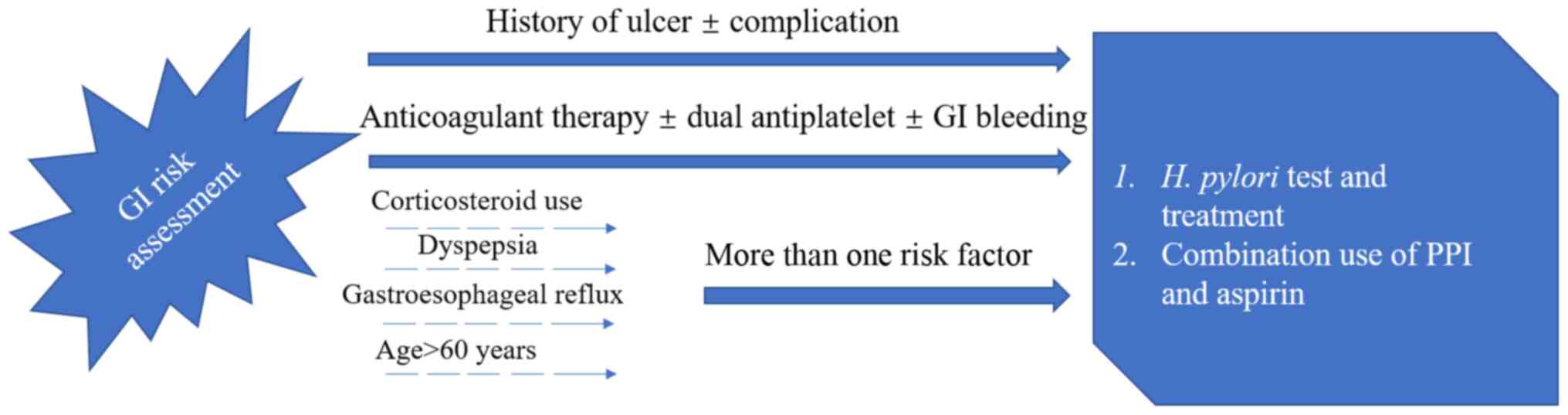
to the report by the American College of Cardiology Foundation Task
Force (Fig. 1) (107), PPI were recommended in association
with low-dose aspirin for patients with prior history of ulcer
diseases or complicated GI ulcer. For other patients who have more
than one risk factor among the categories of corticosteroid use,
dyspepsia or gastroesophageal reflux and age >60 years, PPI are
recommended. As H. pylori is an important risk factor for
ulcer and ulcer bleeding in patients on LDA, a systematic testing
for and eradication of H. pylori is recommended before
starting aspirin for patients with prior history of ulcer disease
(107). The value of PPI combined
with aspirin lies not only in its ability to decrease the incidence
of adverse events in the upper GI, but also in its ability to
decrease the risk of withdrawal of aspirin (114,115).
This has been confirmed in both RCTs and observational studies
(114,115).
Clinicians always face clinical dilemmas and need to
balance the risks and benefits of treatment. The use of aspirin in
preventing GI cancer (or adenoma) and the risk of GI damage is one
of these situations. In conclusion, the continued prophylactic use
of LDA (75–325 mg/day) for at least 4–5 years to prevent GI cancer
in non-high-risk populations aged 55–65 years should be considered
for several reasons: i) A large amount of evidence suggests that
LDA may play a prophylactic role in GI cancer. In addition, LDA
causes less damage to the GI tract compared with high-dose aspirin.
ii) The negative effects of aspirin to the GI tract are mainly the
damage to the upper GI tract. The efficacy of PPI in treating
LDA-related gastroduodenal ulcers and bleeding in most populations
has been well documented and recognized. iii) Although, there is no
effective preventive measure for lower GI bleeding, the clinical
significance of LDA-induced lower GI mucosal injury is still
unclear. Most studies investigating lower GI bleeding events had
small sample sizes with wide CIs. LDA is routinely used in the
primary and secondary prophylaxis of CVD. With a globally aging
population (116), the consumption
of LDA seems likely to increase in the future. Effects of aspirin
need to be seen from a risk-benefit perspective, and from all the
aforementioned evidence, we believe that the benefits outweigh the
risks. However, unanswered questions related to the exact mechanism
of cancer-related effects, optimal dose, duration, treatment
options, and the balance of risks and benefits among specific
populations need to be further investigated. The present review
will contribute to continued progress in this exciting area of
research.
Not applicable.
This study was supported by grants from the Natural
Science Foundation of Ningbo (grant no. 2016A610158), the Natural
Science Foundation of Ningbo (grant no. 2014A610226) and the
Scientific Benefit for People Project of Ningbo (grant no.
2014C51001).
Not applicable.
ZL wrote the paper and collected the data. BS and ZW
conceived and designed the review. CC and HS collected important
background information, prepared the preliminary work of the
manuscript and assisted in preliminary data collection. XD reviewed
and edited the manuscript. All authors have read and approved the
final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Jemal A, Center MM, DeSantis C and Ward
EM: Global patterns of cancer incidence and mortality rates and
trends. Cancer Epidemiol Biomarkers Prev. 19:1893–1907. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Onyoh EF, Hsu WF, Chang LC, Lee YC, Wu MS
and Chiu HM: The rise of colorectal cancer in asia: Epidemiology,
screening, and management. Curr Gastroenterol Rep. 21:362019.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rahman R, Asombang AW and Ibdah JA:
Characteristics of gastric cancer in Asia. World J Gastroenterol.
20:4483–4490. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wick JY: Aspirin: A history, A love story.
Consult Pharm. 27:322–329. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Amsterdam EA, Wenger NK, Brindis RG, Casey
DE, Ganiats TG, Holmes DR, Jaffe AS, Jneid H, Kelly RF, Kontos MC,
et al: 2014 AHA/ACC Guideline for the management of patients with
Non-ST-Elevation acute coronary syndromes: Executive summary: A
Report of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines. J Am Colle Cardiol.
64:2645–2687. 2014. View Article : Google Scholar
|
|
7
|
Antithrombotic Trialists' (ATT)
Collaboration, . Baigent C, Blackwell L, Collins R, Emberson J,
Godwin J, Peto R, Buring J, Hennekens C, Kearney P, et al: Aspirin
in the primary and secondary prevention of vascular disease:
Collaborative meta-analysis of individual participant data from
randomised trials. Lancet. 373:1849–1860. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Roffi M, Patrono C, Collet J, Mueller C,
Valgimigli M, Andreotti F, Bax J, Borger M, Brotons C, Chew DP, et
al: 2015 ESC Guidelines for the management of acute coronary
syndromes in patients presenting without persistent ST-segment
elevation. Task Force for the management of acute coronary
syndromes in patients presenting without persistent ST-Segment
Elevation of the European Society of Cardiology (ESC). G Ital
Cardiol (Rome). 17:831–872. 2016.(In Italian). PubMed/NCBI
|
|
9
|
Smith DK, Demetriou T and Weber C: Aspirin
for primary prevention: USPSTF recommendations for CVD and
colorectal cancer. J Fam Pract. 68:146–151. 2019.PubMed/NCBI
|
|
10
|
Ventura L, Miccinesi G, Barchielli A,
Manneschi G, Puliti D, Mantellini P, Orso F and Zappa M: Does
low-dose aspirin use for cardiovascular disease prevention reduce
colorectal cancer deaths? A comparison of two cohorts in the
Florence district, Italy. Eur J Cancer Prev. 27:134–139. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bibbins-Domingo K; U.S. Preventive
Services Task Force, : Aspirin use for the primary prevention of
cardiovascular disease and colorectal cancer: U.S. Preventive
Services Task Force recommendation statement. Ann Intern Med.
164:836–845. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cea Soriano L, Soriano-Gabarró M and
García Rodríguez LA: Incidence of colorectal cancer in new users
and non-users of low-dose aspirin without existing cardiovascular
disease: A cohort study using The Health Improvement Network. Int J
Cardiol. 248:376–381. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Soon S, Chia WJ, Redekop K and Wee HL: A
Cost-effectiveness analysis of aspirin in the primary prevention of
cardiovascular diseases and colorectal cancer. Value Health.
18:A4622015. View Article : Google Scholar
|
|
14
|
Lanas A and Gargallo CJ: Management of
low-dose aspirin and clopidogrel in clinical practice: A
gastrointestinal perspective. J Gastroenterol. 50:626–637. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lanas A and Scheiman J: Low-dose aspirin
and upper gastrointestinal damage: Epidemiology, prevention and
treatment. Curr Med Res Opin. 23:163–173. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yuhara H, Corley DA, Nakahara F, Nakajima
T, Koike J, Igarashi M, Suauki T and Mine T: Aspirin and
non-aspirin NSAIDs increase risk of colonic diverticular bleeding:
A systematic review and meta-analysis. J Gastroenterol.
49:992–1000. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Strum WB: Colorectal adenomas. N Engl J
Med. 374:1065–1075. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Giovannucci E, Rimm E, Stampfer M, Colditz
G, Ascherio A and Willett WC: Aspirin use and the risk for
colorectal cancer and adenoma in male health professionals. Ann
Intern Med. 121:241–246. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Thun MJ, Namboodiri MM and Heath C Jr:
Aspirin use and reduced risk of fatal colon cancer. N Engl J Med.
325:1593–1596. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sandler R, Halabi S, Baron J, Budinger S,
Paskett E, Keresztes R, Petrelli N, Pipas J, Karp D, Loprinzi CL,
et al: A randomized trial of aspirin to prevent colorectal adenomas
in patients with previous colorectal cancer. N Engl J Med.
348:883–890. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Baron JA, Cole BF, Sandler RS, Haile RW,
Ahnen D, Bresalier R, McKeown-Eyssen G, Summers RW, Rothstein R,
Burke CA, et al: A randomized trial of aspirin to prevent
colorectal adenomas. N Engl J Med. 348:891–899. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Half E, Bercovich D and Rozen P: Familial
adenomatous polyposis. Orphanet J Rare Dis. 4:222009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aihara H, Kumar N and Thompson CC:
Diagnosis, surveillance, and treatment strategies for familial
adenomatous polyposis: Rationale and update. Eur J Gastroenterol
Hepatol. 26:255–262. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Iwama T, Tamura K, Morita T, Hirai T,
Hasegawa H, Koizumi K, Shirouzu K, Sugihara K, Yamamura T, Muto T,
et al: A clinical overview of familial adenomatous polyposis
derived from the database of the polyposis registry of Japan. Int J
Clin Oncol. 9:308–316. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jasperson K and Burt RW: The genetics of
colorectal cancer. Surg Oncol Clin N Am. 24:683–703. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ishikawa H: Chemoprevention of
carcinogenesis in familial tumors. Int J Clin Oncol. 9:299–303.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ishikawa H, Wakabayashi K, Suzuki S, Mutoh
M, Hirata K, Nakamura T, Takeyama I, Kawano A, Gondo N, Abe T, et
al: Preventive effects of low-dose aspirin on colorectal adenoma
growth in patients with familial adenomatous polyposis:
Double-blind, randomized clinical trial. Cancer Med. 2:50–56. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Burn J, Bishop DT, Chapman PD, Elliott F,
Bertario L, Dunlop MG, Eccles D, Ellis A, Evans DG, Fodde R, et al:
A randomized placebo-controlled prevention trial of aspirin and/or
resistant starch in young people with familial adenomatous
polyposis. Cancer Prev Res (Phila). 4:655–665. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Cea Soriano L, Soriano-Gabarró M and
Garcia Rodríiguez LA: Incidence of colorectal cancer in new users
and non-users of low-dose aspirin without existing cardiovascular
disease: A cohort study using The Health Improvement Network. Int J
Cardiol. 248:376–381. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cao Y, Nishihara R, Wu K, Wang M, Ogino S,
Willett WC, Spiegelman D, Fuchs CS, Giovannucci EL and Chan AT:
Population-wide impact of long-term use of aspirin and the risk for
cancer. JAMA Oncol. 2:762–769. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Thun MJ, Henley SJ and Patrono C:
Nonsteroidal Anti-inflammatory drugs as anticancer agents:
Mechanistic, pharmacologic, and clinical issues. J Nat Cancer Inst.
94:252–266. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Rothwell PM, Price JF, Fowkes FG,
Zanchetti A, Roncaglioni MC, Tognoni G, Lee R, Belch JF, Wilson M,
Mehta Z and Meade TW: Short-term effects of daily aspirin on cancer
incidence, mortality, and non-vascular death: Analysis of the time
course of risks and benefits in 51 randomised controlled trials.
Lancet. 379:1602–1612. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chubak J, Whitlock EP, Williams SB,
Kamineni A, Burda BU, Buist DS and Anderson ML: Aspirin for the
prevention of cancer incidence and mortality: Systematic evidence
reviews for the U.S. Preventive Services Task Force. Ann Intern
Med. 164:814–825. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Flossmann E and Rothwell PM; British
Doctors Aspirin Trial and the UK-TIA Aspirin Trial, : Effect of
aspirin on long-term risk of colorectal cancer: Consistent evidence
from randomised and observational studies. Lancet. 369:1603–1613.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rothwell PM, Wilson M, Elwin CE, Norrving
B, Algra A, Warlow CP and Meade TW: Long-term effect of aspirin on
colorectal cancer incidence and mortality: 20-year follow-up of
five randomised trials. Lancet. 376:1741–1750. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Li XF, Xu BZ and Wang SZ: Aspirin inhibits
the proliferation and migration of gastric cancer cells in
p53-knockout mice. Oncol Lett. 12:3183–3186. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ratnasinghe LD, Graubard BI, Kahle L,
Tangrea JA, Taylor PR and Hawk E: Aspirin use and mortality from
cancer in a prospective cohort study. Anticancer Res. 24:3177–3184.
2004.PubMed/NCBI
|
|
38
|
Thun MJ, Namboodiri MM, Calle EE, Flanders
WD and Heath CW Jr: Aspirin use and risk of fatal cancer. Cancer
Res. 53:1322–1327. 1993.PubMed/NCBI
|
|
39
|
Rothwell PM, Fowkes FGR, Belch JFF, Ogawa
H, Warlow CP and Meade TW: Effect of daily aspirin on long-term
risk of death due to cancer: Analysis of individual patient data
from randomised trials. Lancet. 377:31–41. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Farrow DC, Vaughan TL, Hansten PD,
Stanford JL, Risch HA, Gammon MD, Chow WH, Dubrow R, Ahsan H, Mayne
ST, et al: Use of aspirin and other nonsteroidal anti-inflammatory
drugs and risk of esophageal and gastric cancer. Cancer Epidemiol
Biomarkers Prev. 7:97–102. 1998.PubMed/NCBI
|
|
41
|
Vaughan TL, Dong LM, Blount PL, Ayub K,
Odze RD, Sanchez CA, Rabinovitch PS and Reid BJ: Non-steroidal
anti-inflammatory drugs and risk of neoplastic progression in
Barrett's oesophagus: A prospective study. Lancet Oncol. 6:945–952.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
González-Pérez A, Rodríguez LAG and
LópezRidaura R: Effects of non-steroidal anti-inflammatory drugs on
cancer sites other than the colon and rectum: A meta-analysis. BMC
Cancer. 3:282003. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Liu JF, Jamieson GG, Wu TC, Zhu GJ and
Drew PA: A preliminary study on the postoperative survival of
patients given aspirin after resection for squamous cell carcinoma
of the esophagus or adenocarcinoma of the cardia. Ann Surg Oncol.
16:1397–1402. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Frouws MA, Bastiaannet E, Langley RE, Chia
WK, van Herk-Sukel MP, Lemmens VE, Putter H, Hartgrink HH, Bonsing
BA, Van de Velde CJ, et al: Effect of low-dose aspirin use on
survival of patients with gastrointestinal malignancies; an
observational study. Br J Cancer. 116:405–413. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Macfarlane TV, Murchie P and Watson MC:
Aspirin and other non-steroidal anti-inflammatory drug
prescriptions and survival after the diagnosis of head and neck and
oesophageal cancer. Cancer Epidemiol. 39:1015–1022. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Bosetti C, Rosato V, Gallus S, Cuzick J
and La Vecchia C: Aspirin and cancer risk: A quantitative review to
2011. Ann Oncol. 23:1403–1415. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Jankowski JAZ, de Caestecker J, Love SB,
Reilly G, Watson P, Sanders S, Ang Y, Morris D, Bhandari P, Brooks
C, et al: Esomeprazole and aspirin in Barrett's oesophagus
(AspECT): A randomised factorial trial. Lancet. 392:400–408. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Spence AD, Busby J, Johnston BT, Baron JA,
Hughes CM, Coleman HG and Cardwell CR: Low-Dose aspirin use does
not increase survival in 2 independent population-based cohorts of
patients with esophageal or gastric cancer. Gastroenterology.
154:849–860.e1. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Choi JH, Lee SH, Huh G, Chun JW, You MS,
Paik WH, Ryu JK and Kim YT: The association between use of statin
or aspirin and pancreatic ductal adenocarcinoma: A nested
case-control study in a Korean nationwide cohort. Cancer Med.
8:7419–7430. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Sahasrabuddhe VV, Gunja MZ, Graubard BI,
Trabert B, Schwartz LM, Park Y, Hollenbeck AR, Freedman ND and
McGlynn KA: Nonsteroidal Anti-inflammatory drug use, chronic liver
disease, and hepatocellular carcinoma. J Natl Cancer Inst.
104:1808–1814. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Coogan PF, Rosenberg L, Palmer JR, Strom
BL, Zauber AG, Stolley PD and Shapiro S: Nonsteroidal
anti-inflammatory drugs and risk of digestive cancers at sites
other than the large bowel. Cancer Epidemiol Biomarkers Prev.
9:119–123. 2000.PubMed/NCBI
|
|
52
|
Petrick JL, Sahasrabuddhe VV, Chan AT,
Alavanja MC, Beane-Freeman LE, Buring JE, Chen J, Chong DQ,
Freedman ND, Fuchs CS, et al: NSAID use and risk of hepatocellular
carcinoma and intrahepatic cholangiocarcinoma: The liver cancer
pooling project. Cancer Prev Res. 8:1156–1162. 2015. View Article : Google Scholar
|
|
53
|
Singh S, Singh PP, Roberts LR and Sanchez
W: Chemopreventive strategies in hepatocellular carcinoma. Nat Rev
Gastroenterol Hepatol. 11:45–54. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Hawk ET, Umar A and Viner JL: Colorectal
cancer chemoprevention-an overview of the science 1 1 This article
was prepared in our capacity as employees of the U.S. Federal
Government. Gastroenterology. 126:1423–1447. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Elwood PC, Gallagher AM, Duthie GG, Mur LA
and Morgan G: Aspirin, salicylates, and cancer. Lancet.
373:1301–1309. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Pasche B, Wang M, Pennison M and Jimenez
H: Prevention and treatment of cancer with aspirin: Where do we
stand? Semin Oncol. 41:397–401. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Mahboubi Rabbani SMI and Zarghi A:
Selective COX-2 inhibitors as anticancer agents: A patent review
(2014–2018). Expert Opin Ther Pat. 29:407–427. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Poorani R, Bhatt AN, Dwarakanath BS and
Das UN: COX-2, aspirin and metabolism of arachidonic,
eicosapentaenoic and docosahexaenoic acids and their physiological
and clinical significance. Eur J Pharmacol. 785:116–132. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Wang D and Dubois RN: Prostaglandins and
cancer. Gut. 55:115–122. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Chell S, Kaidi A, Williams AC and
Paraskeva C: Mediators of PGE2 synthesis and signalling downstream
of COX-2 represent potential targets for the prevention/treatment
of colorectal cancer. Biochim Biophys Acta. 1766:104–119.
2006.PubMed/NCBI
|
|
61
|
Chan AT, Ogino S and Fuchs CS: Aspirin and
the risk of colorectal cancer in relation to the expression of
COX-2. N Engl J Med. 356:2131–2142. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Zhang L, Yu J, Park BH, Kinzler KW and
Vogelstein B: Role of BAX in the apoptotic response to anticancer
agents. Science. 290:989–992. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zhang Z and Dubois RN: Par-4, a
proapoptotic gene, is regulated by NSAIDs in human colon carcinoma
cells. Gastroenterol. 118:1012–1017. 2000. View Article : Google Scholar
|
|
64
|
Kashfi K and Rigas B: Non-COX-2 targets
and cancer: Expanding the molecular target repertoire of
chemoprevention. Biochem Pharmacol. 70:969–986. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Shureiqi I, Xu X, Chen D, Lotan R, Morris
JS, Fischer SM and Lippman SM: Nonsteroidal anti-inflammatory drugs
induce apoptosis in esophageal cancer cells by restoring
15-lipoxygenase-1 expression. Cancer Res. 61:4879–4884.
2001.PubMed/NCBI
|
|
66
|
Elmore S: Apoptosis: A review of
programmed cell death. Toxicol Pathol. 35:495–516. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
McIlhatton MA, Tyler J, Burkholder S,
Ruschoff J, Rigas B, Kopelovich L and Fishel R: Nitric
Oxide-donating aspirin derivatives suppress microsatellite
instability in mismatch repair-deficient and hereditary
nonpolyposis colorectal cancer cells. Cancer Res. 67:10966–10975.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Rüschoff J, Wallinger S, Dietmaier W,
Bocker T, Brockhoff G, Hofstädter F and Fishel R: Aspirin
suppresses the mutator phenotype associated with hereditary
nonpolyposis colorectal cancer by genetic selection. Proc Natl Acad
Sci USA. 95:11301–11306. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Goel A, Chang DK, Ricciardiello L, Gasche
C and Boland CR: A novel mechanism for aspirin-mediated growth
inhibition of human colon cancer cells. Clin Cancer Res. 9:383–390.
2003.PubMed/NCBI
|
|
70
|
Huang Z, Fang W, Liu W, Wang L, Liu B and
Liu S and Liu S: Aspirin induces Beclin-1-dependent autophagy of
human hepatocellular carcinoma cell. Eur J Pharmacol. 823:58–64.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Bhattacharya A and Eissa NT: Autophagy and
autoimmunity crosstalks. Front Immunol. 4:882013. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Henry WS, Laszewski T, Tsang T, Beca F,
Beck AH, McAllister SS and Toker A: Aspirin suppresses growth in
PI3K-mutant breast cancer by activating AMPK and inhibiting mTORC1
signaling. Cancer Res. 77:790–801. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Liu W, Jiang Y, Sun J, Geng S, Pan Z,
Prinz RA, Wang C, Sun J, Jiao X and Xu X: Activation of
TGF-β-activated kinase 1 (TAK1) restricts Salmonella Typhimurium
growth by inducing AMPK activation and autophagy. Cell Death Dis.
9:5702018. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Hardie DG, Ross FA and Hawley SA:
AMP-Activated protein kinase: A target for drugs both ancient and
modern. Chem Biol. 19:1222–1236. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Kostadinov RL, Kuhner MK, Li X, Sanchez
CA, Galipeau PC, Paulson TG, Sather CL, Srivastava A, Odze RD,
Blount PL, et al: NSAIDs modulate clonal evolution in Barrett's
esophagus. PLoS Genet. 9:e10035532013. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Drew DA, Cao Y and Chan AT: Aspirin and
colorectal cancer: The promise of precision chemoprevention. Nat
Rev Cancer. 16:173–186. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Gala MK and Chan AT: Molecular pathways:
Aspirin and Wnt signaling-a molecularly targeted approach to cancer
prevention and treatment. Clin Cancer Res. 21:1543–1548. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Yeomans ND, Lanas AI, Talley NJ, Thomson
AB, Daneshjoo R, Eriksson B, Appelman-Eszczuk S, Långström G,
Naesdal J, Serrano P, et al: Prevalence and incidence of
gastroduodenal ulcers during treatment with vascular protective
doses of aspirin. Aliment Pharmacol Ther. 22:795–801. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Cayla G, Collet JP, Silvain J, Thiefin G,
Woimant F and Montalescot G: Prevalence and clinical impact of
Upper Gastrointestinal Symptoms in subjects treated with low dose
aspirin: The UGLA survey. Int J Cardiol. 156:69–75. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Biondi-Zoccai GG, Lotrionte M, Agostoni P,
Abbate A, Fusaro M, Burzotta F, Testa L, Sheiban I and Sangiorgi G:
A systematic review and meta-analysis on the hazards of
discontinuing or not adhering to aspirin among 50,279 patients at
risk for coronary artery disease. Eur Heart J. 27:2667–2674. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Baron JA, Senn S, Voelker M, Lanas A,
Laurora I, Thielemann W, Bruckner A and McCarthy D:
Gastrointestinal adverse effects of short-term aspirin use: A
meta-analysis of published randomized controlled trials. Drugs R D.
13:9–16. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Cayla G, Collet JP, Silvain J, Thiefin G,
Woimant F and Montalescot G: Prevalence and clinical impact of
Upper Gastrointestinal Symptoms in subjects treated with low dose
aspirin: The UGLA survey. Int J Cardiol. 156:69–75. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Yeomans ND and Naesdal J: Systematic
review: Ulcer definition in NSAID ulcer prevention trials. Aliment
Pharmacol Ther. 27:465–472. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Cryer B and Feldman M: Effects of very low
dose daily, long-term aspirin therapy on gastric, duodenal, and
rectal prostaglandin levels and on mucosal injury in healthy
humans. Gastroenterology. 117:17–25. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Papatheodoridis GV, Sougioultzis S and
Archimandritis AJ: Effects of Helicobacter pylori and
nonsteroidal anti-inflammatory drugs on peptic ulcer disease:
Systematic review. Clin Gastroenterol Hepatol. 4:130–142. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Huang JQ, Sridhar S and Hunt RH: Role of
Helicobacter pylori infection and non-steroidal
anti-inflammatory drugs in peptic-ulcer disease: A meta-analysis.
Lancet. 359:14–22. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Thorat MA and Cuzick J: Prophylactic use
of aspirin: Systematic review of harms and approaches to mitigation
in the general population. Eur J Epidemiol. 30:5–18. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Iwamoto J, Mizokami Y, Shimokobe K, Ito M,
Hirayama T, Saito Y, Ikegami T, Honda A and Matsuzaki Y: Clinical
features of gastroduodenal ulcer in Japanese patients taking
low-dose aspirin. Dig Dis Sci. 55:2270–2274. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Garcia Rodriguez LA, Martin-Perez M,
Hennekens CH, Rothwell PM and Lanas A: Bleeding Risk with long-term
low-dose aspirin: A systematic review of observational studies.
PLoS One. 11:e01600462016. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
McNeil JJ, Wolfe R, Woods RL, Tonkin AM,
Donnan GA, Nelson MR, Reid CM, Lockery JE, Kirpach B, Storey E, et
al: Effect of aspirin on cardiovascular events and bleeding in the
healthy elderly. N Engl J Med. 379:1509–1518. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
de Abajo FJ and García Rodríguez LA: Risk
of upper gastrointestinal bleeding and perforation associated with
low-dose aspirin as plain and enteric-coated formulations. BMC Clin
Pharmacol. 1:12001. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Lanas A, Serrano P, Bajador E, Esteva F,
Benito R and Sáinz R: Evidence of aspirin use in both upper and
lower gastrointestinal perforation. Gastroenterology. 112:683–689.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Yamada A, Sugimoto T, Kondo S, Ohta M,
Watabe H, Maeda S, Togo G, Yamaji Y, Ogura K, Okamoto M, et al:
Assessment of the risk factors for colonic diverticular hemorrhage.
Dis Colon Rectum. 51:116–120. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Lanas Á, Carrera-Lasfuentes P, Arguedas Y,
García S, Bujanda L, Calvet X, Ponce J, Perez-Aísa Á, Castro M,
Muñoz M, et al: Risk of upper and lower gastrointestinal bleeding
in patients taking nonsteroidal anti-inflammatory drugs,
antiplatelet agents, or anticoagulants. Clin Gastroenterol Hepatol.
13:906–912.e2. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Hirata Y, Kataoka H, Shimura T, Mizushima
T, Mizoshita T, Tanida S, Kamiya T and Joh T: Incidence of
gastrointestinal bleeding in patients with cardiovascular disease:
Buffered aspirin versus enteric-coated aspirin. Scand J
Gastroenterol. 46:803–809. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Nagata N, Niikura R, Aoki T, Shimbo T,
Kishida Y, Sekine K, Tanaka S, Watanabe K, Sakurai T, Yokoi C, et
al: Colonic diverticular hemorrhage associated with the use of
nonsteroidal anti-inflammatory drugs, low-dose aspirin,
antiplatelet drugs, and dual therapy. J Gastroenterol Hepatol.
29:1786–1793. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Reichert MC, Krawczyk M, Appenrodt B,
Casper M, Friesenhahn-Ochs B, Grünhage F, Jüngst C, Zimmer V,
Lammert F and Dauer M: Selective association of nonaspirin NSAIDs
with risk of diverticulitis. Int J Colorectal Dis. 33:423–430.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Strate LL, Liu YL, Huang ES, Giovannucci
EL and Chan AT: Use of aspirin or nonsteroidal anti-inflammatory
drugs increases risk for diverticulitis and diverticular bleeding.
Gastroenterology. 140:1427–1433. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
O'Connor N, Dargan PI and Jones AL:
Hepatocellular damage from non-steroidal anti-inflammatory drugs.
QJM. 96:787–791. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
McNeil JJ, Nelson MR, Woods RL, Lockery
JE, Wolfe R, Reid CM, Kirpach B, Shah RC, Ives DG, Storey E, et al:
Effect of aspirin on all-cause mortality in the healthy elderly. N
Engl J Med. 379:1519–1528. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Burn J, Gerdes AM, Macrae F, Mecklin JP,
Moeslein G, Olschwang S, Eccles D, Evans DG, Maher ER, Bertario L,
et al: Long-term effect of aspirin on cancer risk in carriers of
hereditary colorectal cancer: An analysis from the CAPP2 randomised
controlled trial. Lancet. 378:2081–2087. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Würtz M and Grove EL: Interindividual
variability in the efficacy of oral antiplatelet drugs:
Definitions, mechanisms and clinical importance. Curr Pharm Des.
18:5344–5361. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Rocca B and Petrucci G: Variability in the
responsiveness to low-dose aspirin: Pharmacological and
disease-related mechanisms. Thrombosis. 2012:3767212012. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Joharatnam-Hogan N, Cafferty F, Hubner R,
Swinson D, Sothi S, Gupta K, Falk S, Patel K, Warner N, Kunene V,
et al: Aspirin as an adjuvant treatment for cancer: Feasibility
results from the Add-Aspirin randomised trial. Lancet Gastroenterol
Hepatol. 4:854–862. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Kaufman DW, Kelly JP, Wiholm BE, Laszlo A,
Sheehan JE, Koff RS and Shapiro S: The risk of acute major upper
gastrointestinal bleeding among users of aspirin and ibuprofen at
various levels of alcohol consumption. Am J Gastroenterol.
94:3189–3196. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Hernández-Díaz S and García Rodríguez LA:
Cardioprotective aspirin users and their excess risk of upper
gastrointestinal complications. BMC Med. 4:22–20. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Bhatt DL, Scheiman J, Abraham NS, Antman
EM, Chan FK, Furberg CD, Johnson DA, Mahaffey KW and Quigley EM;
American College of Cardiology Foundation Task Force on Clinical
Expert Consensus Documents, : ACCF/ACG/AHA 2008 expert consensus
document on reducing the gastrointestinal risks of antiplatelet
therapy and NSAID use: A Report of the American College of
Cardiology Foundation Task Force on Clinical Expert Consensus
Documents. Circulation. 118:1894–1909. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Kelly JP, Kaufman DW, Jurgelon JM, Sheehan
J, Koff RS and Shapiro S: Risk of aspirin-associated major
upper-gastrointestinal bleeding with enteric-coated or buffered
product. Lancet. 348:1413–1416. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Lin KJ, Hernández-Díaz S and García
Rodríguez LA: Acid suppressants reduce risk of gastrointestinal
bleeding in patients on antithrombotic or anti-inflammatory
therapy. Gastroenterology. 141:71–79. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Sylvester KW, Cheng JW and Mehra MR:
Esomeprazole and aspirin fixed combination for the prevention of
cardiovascular events. Vasc Health Risk Manag. 9:245–254.
2013.PubMed/NCBI
|
|
111
|
Lanas A, Polo-Tomas M and Casado-Arroyo R:
The aspirin cardiovascular/gastrointestinal risk calculator-a tool
to aid clinicians in practice. Aliment Pharmacol Ther. 37:738–748.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Mo C, Sun G, Lu ML, Zhang L, Wang YZ, Sun
X and Yang YS: Proton pump inhibitors in prevention of low-dose
aspirin-associated upper gastrointestinal injuries. World J
Gastroenterol. 21:5382–5392. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Scally B, Emberson JR, Spata E, Reith C,
Davies K, Halls H, Holland L, Wilson K, Bhala N, Hawkey C, et al:
Effects of gastroprotectant drugs for the prevention and treatment
of peptic ulcer disease and its complications: A meta-analysis of
randomised trials. Lancet Gastroenterol Hepatol. 3:231–241. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Whellan DJ, Goldstein JL, Cryer BL, Eisen
GM, Lanas A, Miller AB, Scheiman JM, Fort JG, Zhang Y and O'Connor
C: PA32540 (a coordinated-delivery tablet of enteric-coated aspirin
325 mg and immediate-release omeprazole 40 mg) versus
enteric-coated aspirin 325 mg alone in subjects at risk for
aspirin-associated gastric ulcers: Results of two 6-month, phase 3
studies. Am Heart J. 168:495–502.e4. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Martín Merino E, Johansson S, Nagy P and
García Rodríguez LA: Effect of baseline gastrointestinal risk and
use of proton pump inhibitors on frequency of discontinuation of
aspirin for secondary cardiovascular prevention in united kingdom
primary care. Am J Cardiol. 112:1075–1082. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Dey AB: World report on ageing and health.
Indian J Med Res. 145:1502017. View Article : Google Scholar
|
|
117
|
Hull MA, Sprange K, Hepburn T, Tan W,
Shafayat A, Rees CJ, Clifford G, Logan RF, Loadman PM, Williams EA,
et al: Eicosapentaenoic acid and aspirin, alone and in combination,
for the prevention of colorectal adenomas (seAFOod Polyp Prevention
trial): A multicentre, randomised, double-blind,
placebo-controlled, 2×2 factorial trial. Lancet. 392:2583–2594.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Cole BF, Logan RF, Halabi S, Benamouzig R,
Sandler RS, Grainge MJ, Chaussade S and Baron JA: Aspirin for the
chemoprevention of colorectal adenomas: Meta-analysis of the
randomized trials. J Natl Cancer Inst. 101:256–266. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Cook NR, Lee IM, Zhang SM, Moorthy MV and
Buring JE: Alternate-day, low-dose aspirin and cancer risk:
Long-term observational follow-up of a randomized trial. Ann Intern
Med. 159:77–85. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Kuan YC, Huang KW, Lin CL, Luo JC and Kao
CH: Effects of aspirin or clopidogrel on colorectal cancer
chemoprevention in patients with type 2 diabetes mellitus. Cancers
(Basel). 11:14682019. View Article : Google Scholar
|
|
121
|
Rothwell PM, Wilson M, Price JF, Belch JF,
Meade TW and Mehta Z: Effect of daily aspirin on risk of cancer
metastasis: A study of incident cancers during randomised
controlled trials. Lancet. 379:1591–1601. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Chan FK, Leung Ki EL, Wong GL, Ching JY,
Tse YK, Au KW, Wu JC and Ng SC: Risks of bleeding recurrence and
cardiovascular events with continued aspirin use after lower
gastrointestinal hemorrhage. Gastroenterology. 151:271–277. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Casado Arroyo R, Polo-Tomas M, Roncales
MP, Scheiman J and Lanas A: Lower GI bleeding is more common than
upper among patients on dual antiplatelet therapy: Long-term
follow-up of a cohort of patients commonly using PPI co-therapy.
Heart. 98:718–723. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Smecuol E, Pinto Sanchez MI, Suarez A,
Argonz JE, Sugai E, Vazquez H, Litwin N, Piazuelo E, Meddings JB,
Bai JC and Lanas A: Low-dose aspirin affects the small bowel
mucosa: Results of a pilot study with a multidimensional
assessment. Clin Gastroenterol Hepatol. 7:524–529. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Moore RA, Derry S and McQuay HJ: Faecal
blood loss with aspirin, nonsteroidal anti-inflammatory drugs and
cyclo-oxygenase-2 selective inhibitors: Systematic review of
randomized trials using autologous chromium-labelled erythrocytes.
Arthritis Res Ther. 10:R72008. View
Article : Google Scholar : PubMed/NCBI
|
|
126
|
Endo H, Higurashi T, Hosono K, Sakai E,
Sekino Y, Iida H, Sakamoto Y, Koide T, Takahashi H, Yoneda M, et
al: Efficacy of Lactobacillus casei treatment on small bowel injury
in chronic low-dose aspirin users: A pilot randomized controlled
study. J Gastroenterol. 46:894–905. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Montalto M, Gallo A, Curigliano V,
D'Onofrio F, Santoro L, Covino M, Dalvai S, Gasbarrini A and
Gasbarrini G: Clinical trial: The effects of a probiotic mixture on
non-steroidal anti-inflammatory drug enteropathy-a randomized,
double-blind, cross-over, placebo-controlled study. Aliment
Pharmacol Ther. 32:209–214. 2010. View Article : Google Scholar : PubMed/NCBI
|