Introduction
According to statistics from the World Health
Organization (WHO) in 2015, esophageal cancer ranks seventh in
terms of global cancer incidence (572,000 new cases per year) and
sixth overall in global cancer-associated mortality (509,000
deaths) (1). Approximately 85% of all
esophageal cancer cases are esophageal squamous cell carcinoma
(ESCC), and the most common cause of death is metastasis (2). Tumor staging and grading systems are
important in the clinical diagnosis of cancer, but are currently
not adequate for prognosis and prediction of the disease (3). Frequently, when patients with ESCC are
diagnosed in clinical practice, the majority have already
progressed to advanced stage and/or lymphatic metastasis.
Furthermore, the survival rate in patients with ESCC is very poor,
and there is a lack of specific biomarkers for early diagnosis and
prognosis (4). Therefore, more
efficient and accurate ESCC diagnostic and prognostic biomarkers
are urgently required in order to improve these areas, including
screening for the early stages of ESCC, as well as new effective
treatment methods.
Accumulating evidence has revealed that dysregulated
long non-coding RNAs (lncRNAs) play a number of key biological
roles in the progression of various types of cancer (5,6). An
increasing number of studies have suggested that aberrant
expression of lncRNAs in ESCC is closely associated with
histological type, tumor-node-metastasis (TNM) stage, lymph node
metastasis and prognosis (7,8).
ESCC is a multistep disease, which involves multiple
interactions between genetic and environmental factors.
Furthermore, lncRNAs play an important regulatory role in
epigenetics. Investigating the ESCC-associated alterations of
lncRNAs may aid the identification of valuable biomarkers for ESCC
diagnosis and prognosis. Previous studies have primarily focused on
the diagnostic and prognostic performance of a small portion of
lncRNAs in ESCC, but a larger number of lncRNAs remain unexplored.
Therefore, elucidating the functions of dysregulated lncRNAs,
particularly in ESCC, is currently an important research topic.
Currently, high-throughput RNA sequencing
technologies are being widely used for the detection of lncRNA
alterations in carcinogenesis and screening for potential
biomarkers of numerous diseases (9).
However, the small sample sizes used for microarray detection often
present a bias toward the identification of ESCC-associated lncRNAs
due to lack of RNA sequencing data and, therefore, often generate
errors (10). By using large sample
sizes that integrate multiple RNA sequencing datasets, sufficient
information regarding patients with ESCC can be obtained, thereby
providing more convincing results. Thus far, with the advent of
high-throughput RNA sequencing technologies, The Cancer Genome
Atlas (TCGA; http://portal.gdc.cancer.gov/) and Gene Expression
Omnibus (GEO; http://www.ncbi.nlm.nih.gov/geo/) database platforms
have allowed the collected RNA sequencing data from microarray
chips to be uploaded and standardized for quality control (11). Therefore, identification of the
ESCC-associated lncRNAs would be more reliable with the use of
large sample sizes integrating multiple analyses from different RNA
sequencing databases.
The RNA sequencing databases obtained from the
tissues of patients with ESCC are expected to provide a novel
analysis strategy to identify diagnostic and prognostic biomarkers
for this disease. In the present study, data mining analyses for
ESCC were performed by integrating the significant differences in
RNA obtained from the GEO and TCGA databases. Through these
efforts, co-differentially expressed lncRNAs in ESCC may be
identified. Based on these lncRNAs, subsequent analyses were
performed, including gene functional enrichment analyses, competing
endogenous RNA network construction, assessment of the association
between differentially expressed lncRNAs and the
clinicopathological characteristics of patients with ESCC, and
survival analyses. Finally, reverse transcription-quantitative PCR
(RT-qPCR) was used to validate the bioinformatics analysis results
in the tumor and adjacent non-tumor tissues of 30 patients with
newly diagnosed ESCC. This new approach may contribute to an
improved method for identifying potential lncRNA biomarkers for the
diagnosis of ESCC, as well as its classification and prediction of
prognosis.
Materials and methods
Microarray dataset collection
The present study collected RNA sequencing
expression datasets (lncRNAs, miRNAs and mRNAs) comprising tissue
samples from 802 patients with ESCC, which included cancer tissues
and adjacent normal esophageal tissues from the GEO genomics
database. The RNA sequencing datasets of patients with ESCC were
downloaded from the GSE23400 (12)
(208 tissue samples: http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE23400),
GSE26886 (13) (69 tissue samples:
http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE26886),
GSE45670 (14) (38 tissue samples:
http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE45670),
GSE97049 (14 tissue samples: http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE97049),
GSE6188 (15) (257 tissue samples:
http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE6188)
and GSE55856 (16) (216 tissue
samples: http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE55856)
datasets. All the aforementioned GEO datasets were obtained from
Affymetrix Human Genome Array platforms. A total of 312 patients
with ESCC were obtained from the TCGA database (up to November 1,
2018). Annotation information of the RNA sequencing datasets was
obtained using the Affymetrix Human Genome Array platforms. The
present study was fully compliant with the publication guidelines
provided by the GEO and TCGA databases. The details of GEO and TCGA
database ESCC patient tissue RNA sequencing datasets, sample
descriptions and clinicopathological characteristics are provided
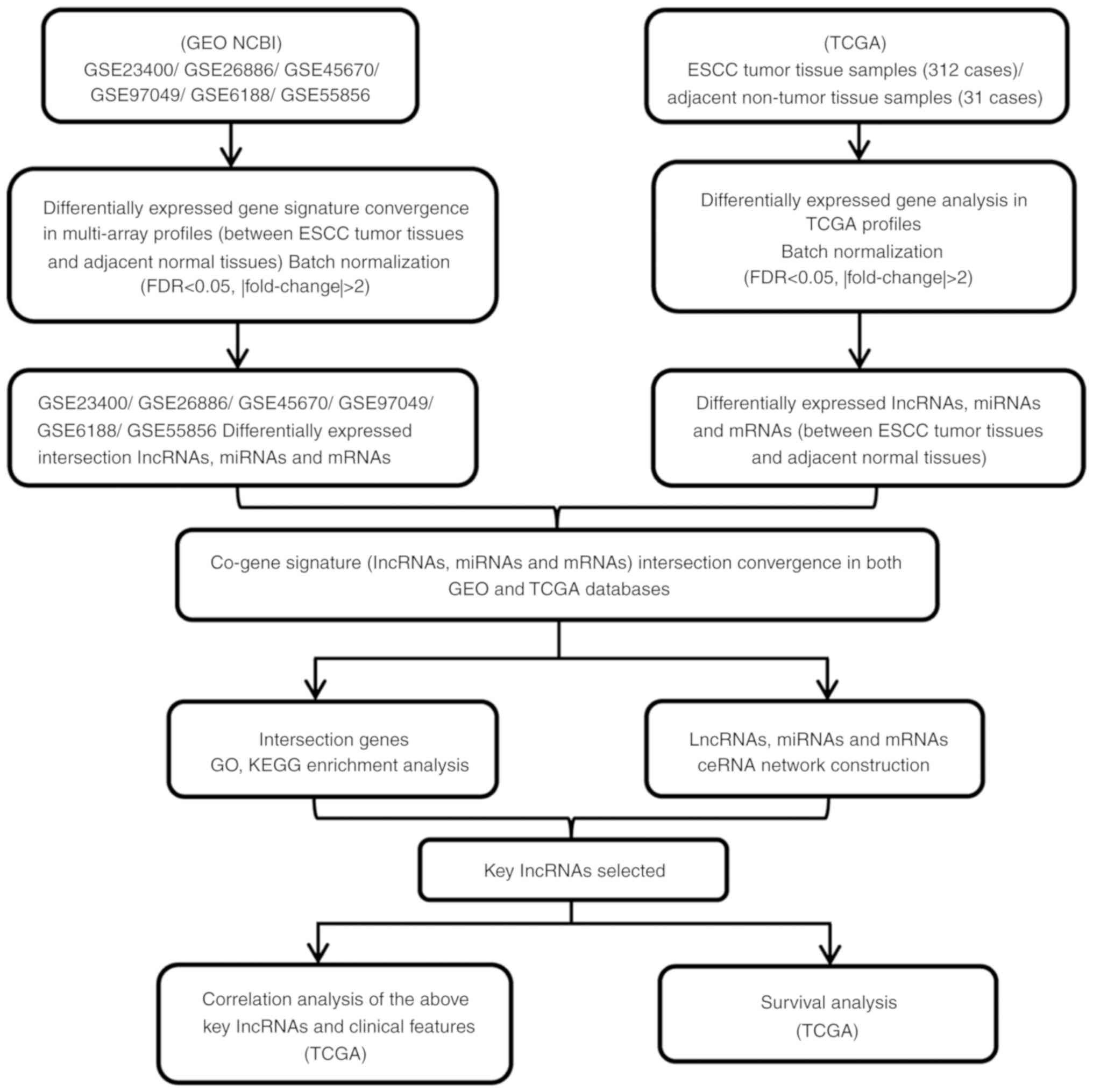
in Tables I and II. A flow diagram of the integrated
bioinformatics analysis from the GEO and TCGA databases is provided
in Fig. 1.
 | Table I.Details of ESCC studies and RNA
sequencing microarray datasets from the GEO database. |
Table I.
Details of ESCC studies and RNA
sequencing microarray datasets from the GEO database.
| GSE | Publication | RNA sequencing
styles | Sample size for
each group |
|---|
| GSE23400 | Clinical cancer
research | lncRNA | Tumor, 104 |
|
|
| mRNA | Adjacent normal
tissues, 104 |
| GSE26886 | BMC Cancer | lncRNA | Tumor, 35 |
|
|
| mRNA | Adjacent normal
tissues, 34 |
| GSE45670 | Annals of
oncology | lncRNA | Tumor, 28 |
|
|
| mRNA | Adjacent normal
tissues, 10 |
| GSE97049 | Unrecorded | miRNA | Tumor, 7 |
|
|
|
| Adjacent normal
tissues, 7 |
| GSE6188 | Cancer
research | miRNA | Tumor, 153 |
|
|
|
| Adjacent normal
tissues, 104 |
| GSE55856 | Gut | miRNA | Tumor, 108 |
|
|
|
| Adjacent normal
tissues, 108 |
| Table II.Clinical information and samples size
for TCGA ESCC datasets. |
Table II.
Clinical information and samples size
for TCGA ESCC datasets.
| Variables | Total cases, n=312
(%) | Alive, n=138
(%) | Deceased, n=174
(%) |
|---|
| Sex |
|
|
|
|
Male | 211 (67.63) | 83 (60.14) | 128 (73.56) |
|
Female | 101 (32.37) | 55 (39.86) | 46 (26.44) |
| Race |
|
|
|
|
White | 162 (51.92) | 5 (39.86) | 107 (61.49) |
|
Asia | 127 (40.71) | 68 (49.28) | 59 (33.91) |
|
Black | 23 (7.37) | 15 (10.87) | 8 (4.60) |
| Age, years |
|
|
|
|
≤50 | 86 (27.56) | 53 (38.41) | 33 (18.97) |
|
>50 | 226 (72.44) | 85 (61.59) | 141 (81.03) |
| Tumor grade |
|
|
|
| GI | 49 (15.71) | 31 (22.46) | 18 (10.34) |
|
GII | 146 (46.79) | 48 (34.78) | 98 (56.32) |
|
GIII–IV | 117 (37.50) | 59 (42.75) | 58 (33.33) |
| TNM stage |
|
|
|
|
I/II | 99 (31.73) | 30 (21.74) | 69 (39.66) |
|
III/IV | 213 (68.27) | 108 (78.26) | 105 (60.34) |
| Lymph node
status |
|
|
|
| No
metastasis | 35 (11.22) | 32 (23.19) | 3 (1.72) |
|
Metastasis | 277 (88.78) | 106 (76.81) | 171 (98.28) |
Annotation of microarray probes
In order to enhance the comparability of the GEO
database RNA sequencing data, the signature values of the GSE23400,
GSE26886, GSE45670, GSE97049, GSE6188 and GSE55856 RNA sequencing
datasets were downloaded and converted to new comparable
transcripts. Probe reannotation methods were used to obtain a
standard measurement of the RNA sequencing expression profiles.
Once the aforementioned ESCC RNA sequencing probe signature values
and probe IDs were downloaded from the GEO database, they underwent
a mapped detection analysis in a database of human genomes, and
those that were mismatched were excluded. The remaining probe
positions on the chromosomes were identified using the GENCODE tool
(https://www.gencodegenes.org/). Probes
matched to both protein-coding genes and lncRNAs were also
excluded. If multiple probes matched the same gene, the median
values were instead used as the expression level of that gene. In
addition, prior to any further analyses, RNA sequencing data
normalization was performed to ensure the data were fully compliant
with the publication guidelines of TCGA.
Integration of microarray data and
differential expression analysis
All the ESCC tissue samples from the GEO database
were downloaded from three or more datasets in order to enlarge the
sample number and avoid generating less reliable results. A
differential analysis was then separately performed for each
dataset, comparing ESCC tumor tissues to adjacent normal tissues
using the limma R 3.4.4 software (https://www.r-project.org/) [false discovery rate
(FDR) <0.05, fold change >2, P<0.05]. Subsequently,
overlapping subclass analyses were used to identify the separate
co-differentially expressed genes in each dataset, including
lncRNAs, miRNAs and mRNAs, with the Venn 2.1 tool (http://bioinfogp.cnb.csic.es/tools/venny/index.html).
The integrated ESCC tissue dysregulated lncRNA, miRNA and mRNA
lists were saved for further analysis.
TCGA database provided the normalized RNA sequencing
data, which included lncRNAs and mRNAs from patients with ESCC
using the RNASeqV2 system. Furthermore, ESCC level 3 normalized
miRNA sequencing data (Illumina HiSeq 2000 microRNA sequencing
platforms) were also downloaded from TCGA. The significantly
differentially expressed lncRNAs, mRNAs and miRNAs in the 312 tumor
tissues and 47 adjacent non-tumor esophageal epithelial tissues in
patients with ESCC were then analyzed (FDR<0.05, fold change
>2, P<0.05). The significantly different lncRNAs, mRNAs and
miRNAs were selected for further analysis.
Finally, according to the fold changes of
differentially expressed lncRNAs, mRNAs and miRNAs in ESCC tissues
from the GEO and TCGA databases, the common genes were selected for
subsequent analysis.
Construction of the competing
endogenous (ce) RNA network
In the present study, an lncRNA, miRNA and mRNA
ceRNA network was built based on the theory that lncRNAs can
regulate miRNA abundance by sequestration binding, acting as ‘miRNA
sponges’ through miRNA binding to the mRNAs and negatively
regulating gene expression. Common ESCC tissues with significantly
differentially expressed lncRNAs, mRNAs and miRNAs (FDR<0.05,
fold change >2, P<0.05) were selected to build the ceRNA
network, in which the fold changes of genes were rooted in the TCGA
database, in order to investigate whether these intersection
lncRNAs, mRNAs and miRNAs were involved in ceRNA regulation.
MiRcode (https://omictools.com/mircode-tool), miRanda
(http://www.microrna.org/microrna/home.do) and
Targetscan (http://www.targetscan.org/) were used to predict the
miRNA target lncRNAs and miRNA-mRNA interactions in the different
databases. Finally, the predicted miRNA target genes and the
significantly differentially expressed intersection genes in the
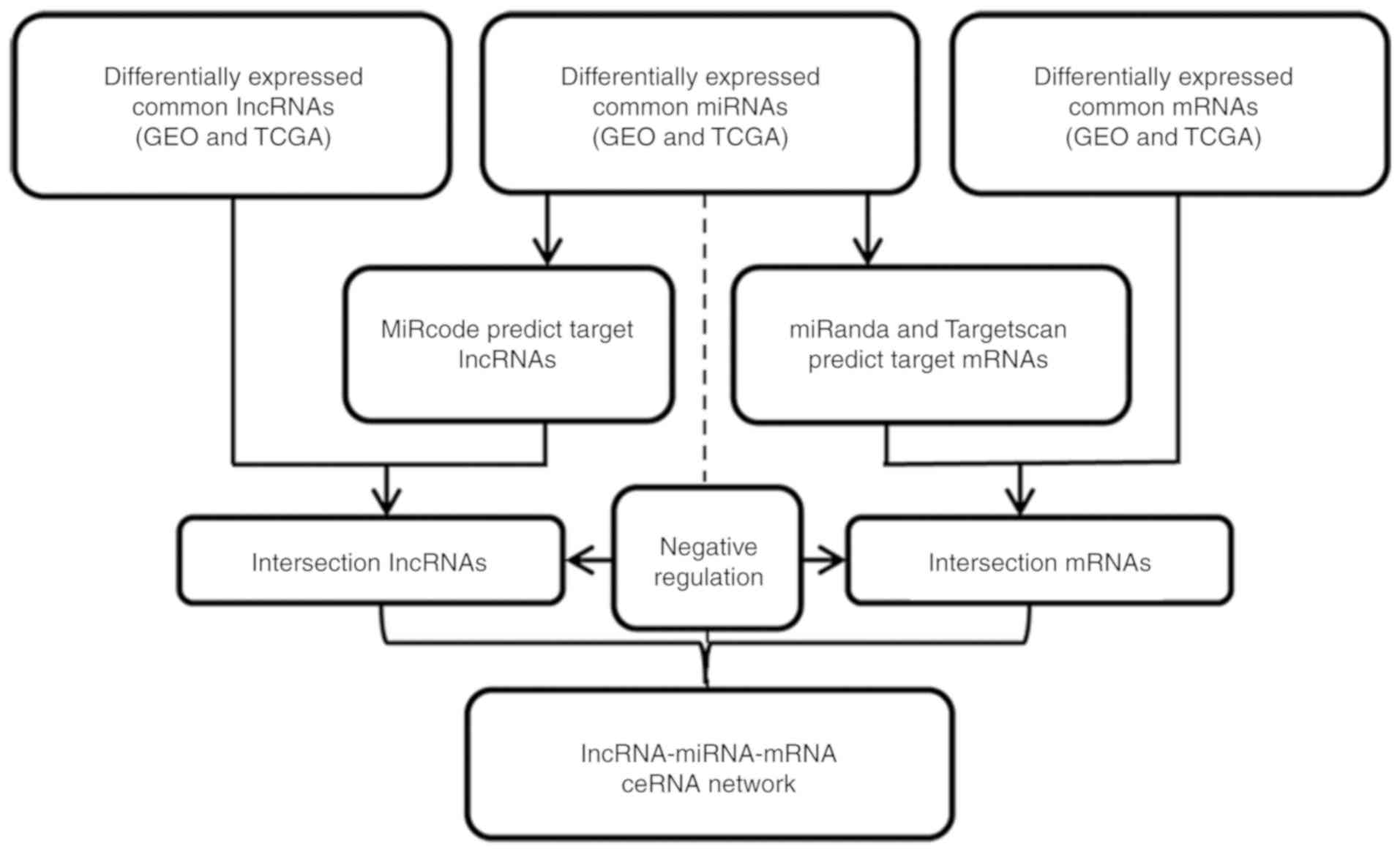
GEO and TCGA databases were used to build the ceRNA network. A flow
chart for the lncRNA, miRNA and mRNA ceRNA network construction is
presented in Fig. 2.
During this process, the lncRNA, miRNA and mRNA
ceRNA network was constructed using the fold change data of the
significantly expressed RNA of patients with ESCC from TCGA
database using the R package. Pearson's correlation matrix models
were used to identify the potential relevance of all pair-wise
genes. Finally, based on the weighted adjacency matrix, the network
connectivity of genes with other genes was investigated, and the
ceRNA network was built using Cytoscape software (version
3.0.).
Gene Ontology (GO) and Kyoto
Encyclopedia of Genes and Genomes (KEGG) pathway analysis
In order to investigate the potential gene
functional enrichment and signaling pathway regulation of the
consensus mRNAs that were involved in the ceRNA network, GO
(http://www.geneontology.org) and KEGG
pathway analyses were performed. The mRNAs that were involved in
the ceRNA network were uploaded to the GO database to investigate
the enriched molecular functions of these mRNAs. Upregulated and
downregulated mRNAs from the ceRNA network were analyzed.
Furthermore, the KEGG tool (http://www.kegg.jp/) was used to identify the
potential regulated signaling pathways of these genes. R software
was used to visualize the GO and KEGG results.
Association between ceRNA network key
lncRNAs and ESCC clinical status from TCGA
Based on the co-expression of the lncRNAs, miRNAs
and mRNAs in the ceRNA network, the key lncRNAs that were involved
in the network were selected as target lncRNAs potentially
associated with ESCC progression. Subsequently, the potential
association between ceRNA network key lncRNAs and TCGA ESCC
patients' clinicopathological characteristics were investigated,
which included sex, TNM stage, tumor grade, lymphatic metastasis
status and pathological stage using multiple linear regression
analysis.
Kaplan-Meier survival analysis
In order to investigate whether the key lncRNAs that
were involved in the ceRNA network were associated with the TCGA
database status, a Kaplan-Meier survival analysis of the ESCC
patients from TCGA was performed. Based on the TCGA ESCC patient
datasets, the fold changes of the aforementioned selected key
lncRNAs in the cancer tissues and overall survival rates of
patients with ESCC were determined using the GEPIA tool (http://gepia.cancer-pku.cn/). Kaplan-Meier survival
analysis parameters were calculated using the publicly available
TCGA ESCC patient datasets and GEPIA tools. The survival
distributions of different TCGA with ESCC, and the expression
changes in key lncRNAs, were examined using Kaplan-Meier analysis,
log-rank test and hazard ratio (HR).
Preparation of human ESCC samples and
RT-qPCR validation of bioinformatics analysis results
Next, 30 tumor and paired non-tumor esophageal
tissues from patients with ESCC were collected from the Gansu Wuwei
Tumor Hospital (Wuwei, China); the patients were aged 40–75 years.
The samples were collected and stored at −80°C. All patients were
diagnosed with ESCC according to their pathological examination
results. Clinical basic information and informed consent forms were
obtained from all ESCC patients (Table
III). The collection of the tumor samples from patients with
ESCC was approved by the Ethics Committee of the Gansu Wuwei Tumor
Hospital.
| Table III.Demographic and clinical
characteristics of 30 patients with ESCC. |
Table III.
Demographic and clinical
characteristics of 30 patients with ESCC.
| Variables | Total cases, n=30
(%) |
|---|
| Age, years | 59±9.72 |
| (mean ± standard
deviation) |
|
| Sex |
|
|
Male | 20 (66.67) |
|
Female | 10 (33.33) |
| TNM stage |
|
|
I/II | 8 (26.67) |
|
III/IV | 22 (73.33) |
| Lymph node
status |
|
| No
metastasis | 9 (30.00) |
|
Metastasis | 21 (70.00) |
Total RNA was isolated from tissue samples using
TRIzol® reagent (Invitrogen; Thermo Fisher Scientific,
Inc.). Reverse Transcription Kit (Promega Corporation) and
GoTaq® qPCR Master Mix of Power SYBR® Green
(Promega Corporation) were used to synthesize cDNA and perform
RT-qPCR analysis. The reaction was performed at 95°C for 2 min,
followed by 40 cycles at 95°C for 15 sec, 60°C for 30 sec and 72°C
for 30 sec. A dissociation curve was analyzed from 60–95°C.
Finally, RT-qPCR was performed using the Step One Plus™ PCR System
(Applied Biosystems; Thermo Fisher Scientific, Inc.). RT-qPCR
relative fold change results were calculated using the
2−ΔΔCq method (17).
Statistical analysis
All ESCC tissue RNA sequencing datasets from the GEO
database were obtained from at least three independent datasets. R
software was used to normalize the RNA sequencing data and compare
significantly differentially expressed genes. Cytoscape 3.0 and
GEPIA software tools were used to construct the ceRNA network and
perform the survival analysis. Two-tailed Student's t-test was used
to assess the differences between subgroups. P<0.05 was
considered to indicate a statistically significant difference.
Results
Convergence of gene expression
signatures across the different datasets of patients with ESCC from
GEO
The ESCC RNA sequencing data and other information
were obtained from the GEO database. In order to increase the
veracity and reliability of the signal values, and also decrease
the possibility of false-positives, three independent datasets were
downloaded, including ESCC tissue lncRNA, miRNA and mRNA sequencing
results. Differentially expressed genes were identified using the
limma package according to the threshold of FDR<0.05, fold
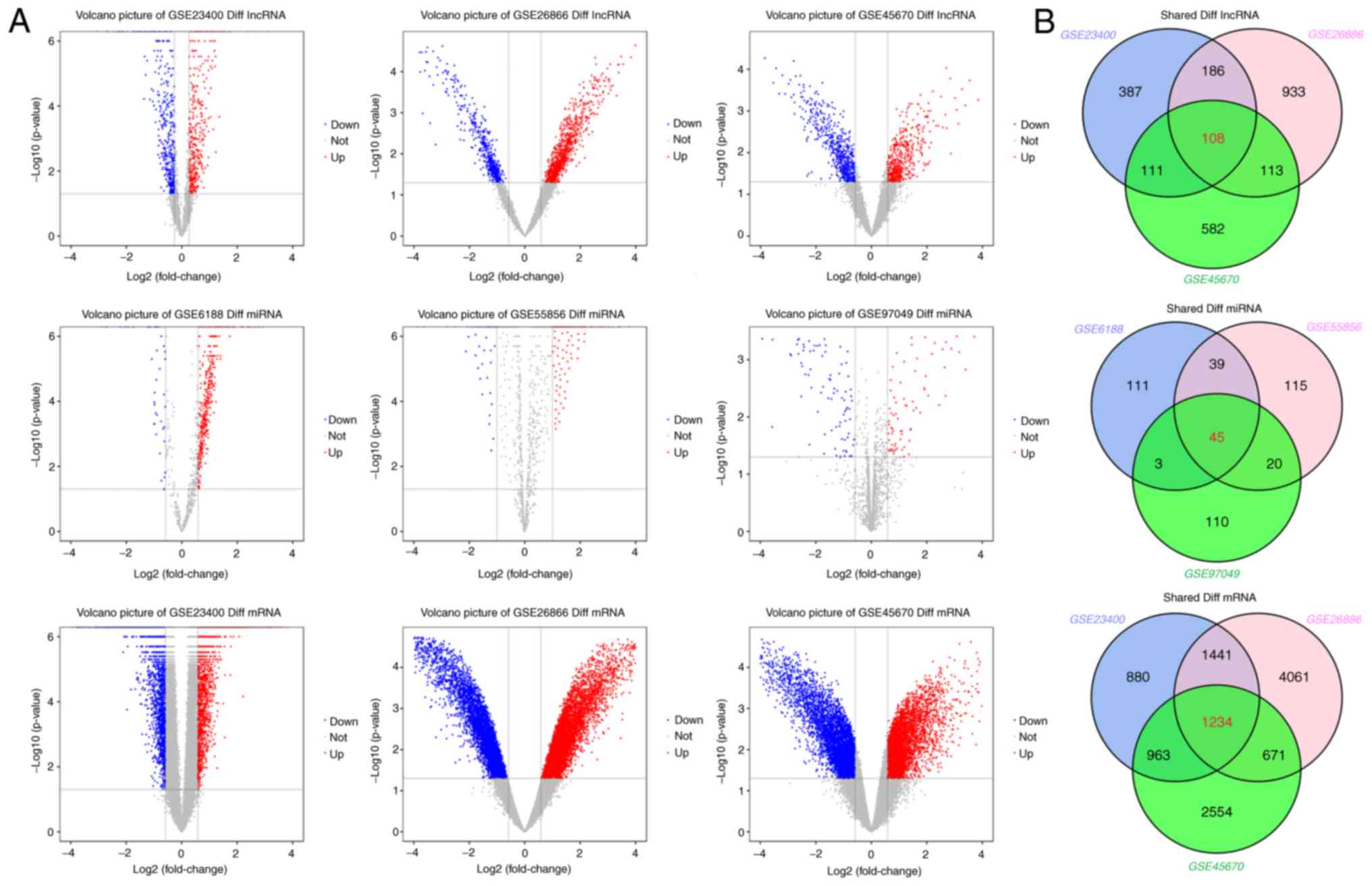
change >2 and P<0.05. Volcano plots and Venn analysis
revealed the number of differentially expressed genes identified
from each dataset (Fig. 3). The
GSE23400 dataset contained 5,310 differentially expressed genes,
including 792 differentially expressed lncRNAs and 4,518 mRNAs. The
GSE26886 dataset contained 8,747 differentially expressed genes,
including 1,340 differentially expressed lncRNAs and 7,407 mRNAs.
The GSE45670 dataset contained 6,336 differentially expressed
genes, including 914 differentially expressed lncRNAs and 5,422
mRNAs. The GSE97049 dataset contained 178 differentially expressed
miRNAs. The GSE6188 dataset contained 198 differentially expressed
miRNAs. Finally, the GSE55856 dataset contained 198 differentially
expressed miRNAs. The detailed information of these six datasets
and the number of differentially expressed genes identified from
each dataset are presented in Table
IV.
| Table IV.Details information of differentially
expressed genes in GEO database. |
Table IV.
Details information of differentially
expressed genes in GEO database.
| GSE | Differentially
expressed genes | Upregulated | Downregulated | Intersection
differentially expressed genes |
|---|
| GSE23400 | lncRNA | 792 | 378 | 414 | 108 |
| GSE26886 | lncRNA | 1340 | 599 | 741 |
|
| GSE45670 | lncRNA | 914 | 508 | 406 |
|
| GSE23400 | mRNA | 4518 | 2219 | 2299 | 1234 |
| GSE26886 | mRNA | 7407 | 3933 | 3474 |
|
| GSE45670 | mRNA | 5422 | 2599 | 2823 |
|
| GSE97049 | miRNA | 178 | 68 | 110 | 45 |
| GSE6188 | miRNA | 198 | 48 | 150 |
|
| GSE55856 | miRNA | 219 | 109 | 110 |
|
Following the Venn tool intersection, differentially
expressed genes were analyzed, and it was demonstrated that there
were 108 common lncRNAs, 1,234 mRNAs and 45 miRNAs with
significantly changed levels in ESCC tissues from the GEO database
(Fig. 3; Table IV). Among those, 59 lncRNAs, 779
mRNAs and 30 miRNAs were upregulated, whereas 49 lncRNAs, 455 mRNAs
and 15 miRNAs were downregulated. Detailed information on these
common significantly differentially expressed genes in ESCC tissues
from GEO database can be found in Tables
SI–SII.
ESCC tissues with co-differentially
expressed genes identified in the GEO and TCGA databases
The ESCC patient tissues RNA sequencing results and
their clinicopathological information were collected from TCGA
database. Compared with the tumor and non-tumor tissue RNA
sequencing results of patients with ESCC from TCGA, we identified a
total of 889 differentially expressed lncRNAs (597 upregulated and
292 downregulated, 4,796 differentially expressed mRNAs (3,170
upregulated and 1,626 downregulated), and 438 differentially
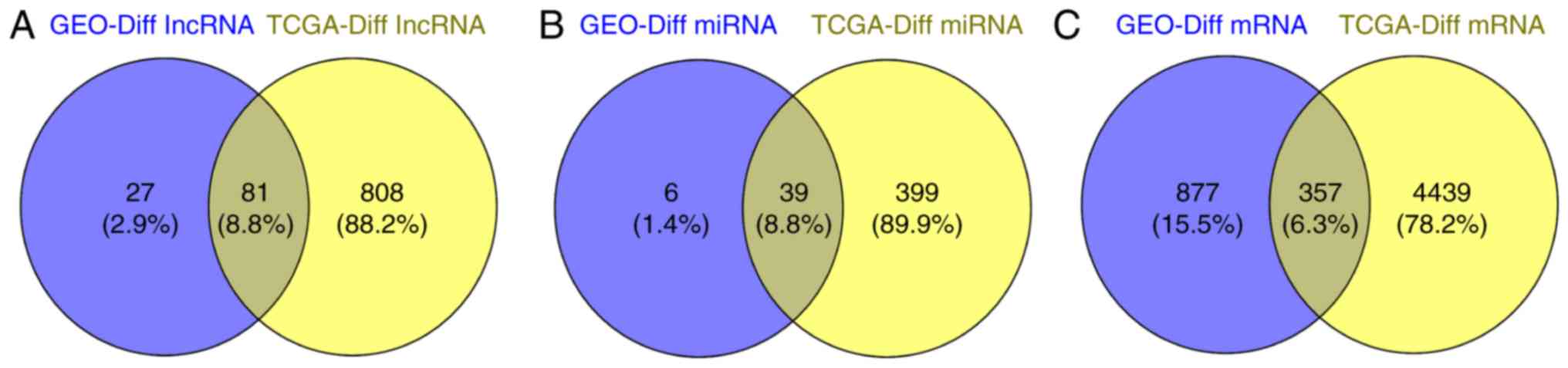
expressed mRNAs (299 upregulated and 139 downregulated) (Table IV). The Venn diagram in Fig. 4 presents the intersections of genes
between the GEO and TCGA databases. A total of 81 co-differentially
expressed lncRNAs, 39 miRNAs and 357 mRNAs were identified
(Fig. 4 and Table V).
| Table V.ESCC-related intersection
co-differentially expressed lncRNAs, miRNAs and mRNAs in GEO and
TCGA. |
Table V.
ESCC-related intersection
co-differentially expressed lncRNAs, miRNAs and mRNAs in GEO and
TCGA.
| Genes | Co-differentially
expressed lncRNAs, miRNAs and mRNAs |
|---|
| lncRNAs | ALOX12P2, AOC4P,
BTN2A3P, C20orf166-AS1, C21orf62-AS1, CMAHP, CYP2D7, CYP4Z2P,
DDX12P, DIRC3, DUSP5P1, ENST00000570167.1, ENST00000584492.5,
FAM66A, FAM86HP, FAM86JP, FAR2P1, FIRRE, FOXD2-AS1, GUCY1B2,
HAND2-AS1, HAVCR1P1, HCP5, HNRNPA3P1, IPW, LINC00176, LINC00341,
LINC00346, LINC00472, LINC00476, LINC00663, LINC00689, LINC00887,
LINC00889, LINC00950, LINC00982, LINC01001, LINC01105, LINC01588,
LOC100128164, LOC100499484-C9ORF174, LOC101928316, LOC148696,
LOC202181, LOC283856, LOC399815, LOC728743, MBL1P, MEG3,
MIR4435-2HG, MIR503HG, MIR600HG, NONHSAT068116.2, NONHSAT075748.2,
NONHSAT179718.1, NONHSAT198787.1, PART1, PCAT18, PSMG3-AS1,
PTGES2-AS1, PVT1, PWAR5, PWARSN, RAMP2-AS1, RPLP0P2, SBF1P1,
SLC26A4-AS1, SLC8A1-AS1, SMIM10L2A, SMIM10L2B, SNHG4, TCAM1P,
TP73-AS1, UCA1, UG0898H09, XR_253656.2, XR_946740.1, ZFAS1,
ZFP91-CNTF, ZNF300P1, ZNF542P |
| miRNAs | let-7c-5p,
let-7g-3p, miR-101-3p, miR-101-5p, miR-106b-5p, miR-125a-5p,
miR-130b-3p, miR-133a-3p, miR-135b-5p, miR-141-3p, miR-143-3p,
miR-145-5p, miR-15b-3p, miR-15b-5p, miR-16-5p, miR-182-5p,
miR-183-5p, miR-185-5p, miR-18a-5p, miR-195-5p, miR-200a-3p,
miR-200b-3p, miR-200c-3p, miR-200c-5p, miR-205-5p, miR-20b-5p,
miR-21-3p, miR-224-5p, miR-28-5p, miR-31-5p, miR-320a, miR-32-5p,
miR-328-3p, miR-330-5p, miR-33a-5p, miR-425-5p, miR-484,
miR-497-5p, miR-93-5p |
| mRNAs | ABCA8, ABCC8,
ACACB, ACADL, ACADSB, ACTG2, ACVR2A, ADAMTSL1, ADCY2, ADCY5, ADCY6,
ADGRD1, ADH1B, ADHFE1, AFF3, AGPS, ALAD, ALDH6A1, ALDH7A1, ANGPTL1,
ANK2, AOX1, APLP1, AQP4, AR, ARHGDIG, ARHGEF6, ARRB1, ASPA, ASXL3,
ATP1A2, ATP4A, ATP4B, AZI2, B3GAT1, B4GALNT2, BID, BIRC5, BMP3,
BMP8B, BMPER, BMS1, C16orf89, C2orf40, C6, C7, CA4, CAB39L,
CACNA2D2, CADM2, CADM3, CALM1, CASQ2, CCBE1, CCKAR, CCKBR, CD1E,
CD44, CDC6, CDH19, CDH2, CDK6, CELF4, CFLAR, CGNL1, CHGA, CHGB,
CHMP2B, CHRDL1, CHST11, CKB, CKM, CKMT2, CLCNKA, CLDN1, CLDN16,
CNKSR2, CNN1, CNTFR, CNTN2, CNTN3, COL2A1, COL4A3, CPA2, CPEB1,
CPEB3, CPLX2, CTNND2, CTSC, CUX2, CYBRD1, CYFIP2, CYP2U1, CYP4B1,
DES, DHX36, DIRAS1, DLG2, DLG3, DNER, DPP10, DPP6, DPT, E2F2, E2F3,
EDA, EDNRB, EFNA5, EIF4EBP2, ELOVL6, EME1, ENAM, ENPP5, EPHA5,
EPHB1, ERBB4, ESPL1, ESRRB, ESRRG, ETNPPL, EXO1, FAM107A, FAR1,
FAXDC2, FGA, FGF2, FGFR1, FGG, FNDC5, FRMD1, FXYD1, FZD4, GAB1,
GAB2, GALNT2, GALNT6, GATA5, GC, GFRA1, GHRL, GIF, GKN1, GKN2,
GNAQ, GPD1L, GPER1, GPM6A, GPR155, GREM2, GRIA1, GRIA3, GRIA4,
GRIK3, GRIK5, GRIN2A, GSTM5, H2AFJ, H2AFX, HCFC2, HDC, HIPK2,
HMGA2, HMGCS2, HMP19, HOXA10, HPN, HPSE2, HS6ST3, HSPB6, HSPB7,
ICOS, ID4, IGF1R, IGF2BP1, IKBKE, IL1RAP, IL6ST, INPP5A, IQSEC3,
IRS1, ITGA8, ITGB8, ITPR2, KAT2B, KCNB1, KCNE2, KCNJ10, KCNJ11,
KCNJ16, KCNK2, KCNMA1, KCNMB2, KCTD8, KIAA0408, KIAA2022, KIF5A,
KLF15, KSR1, LAMC2, LAMTOR3, LDB3, LIFR, LIPF, LMOD1, LONRF2,
MAGI1, MAGI3, MAMDC2, MAOA, MAP3K13, MAP4K4, MAPK4, MAPT, MARVELD3,
MASP1, MFAP5, MFSD4A, MME, MMP14, MOCS1, MT1M, MYH11, MYLK, MYO18B,
MYOC, MYOCD, MYRIP, NBEA, NCAM1, NEGR1, NRXN1, NTN4, OAS2, OGN,
OMD, P2RX2, PANX1, PCDH9, PCSK2, PDCD4, PDCD6IP, PDE1A, PDE2A,
PDE7B, PDZRN4, PEBP4, PGA3, PGA4, PGA5, PGM5, PGR, PI16, PKHD1L1,
PLAU, PLCXD3, PLN, PLP1, PML, PPP1R12B, PPP1R1A, PPP1R9A, PPP2R3A,
PRICKLE2, PRIMA1, PRKAA2, PRKACB, PRKAR2B, PRKCB, PRSS1, PSAPL1,
PSMB2, PSME4, PTGER3, PTGIS, PTGS1, PTPN2, PTPRN, RAB11A,
RAB11FIP2, RAB2A, RAD51, RAG1, RANBP3L, RAP1A, RAPGEF2, RBL1,
RBPMS2, RELN, RGN, RIC3, RIMS4, RNF125, RORC, RPRM, RPS6KA2,
RPS6KA6, RSPO2, RYR2, S1PR1, SCARA5, SCG3, SCIN, SCN7A, SCUBE2,
SEMA3E, SERPINA5, SESN3, SFRP1, SGCA, SH3GL2, SH3GLB1, SIGLEC11,
SIX4, SLC1A2, SLC26A7, SLC2A1, SLC2A4, SLC5A7, SLC9A4, SLIT2, SLK,
SORCS1, SORT1, SOX10, SOX4, SST, STMN1, STMN2, STUM, SYNPO2, SYT4,
TACR1, TCEAL2, TCF3, TFDP2, TGFBR2, THRB, TMEM132C, TNFAIP3,
TNFRSF10B, TNXB, TP53INP2, TRA2B, TRIM50, VAMP2, VIP, VIPR2, WASF3,
WDR17, WISP2, XKR4, YWHAZ, ZBTB16, ZFP36, ZFP36L2, ZNF385B,
ZNF471 |
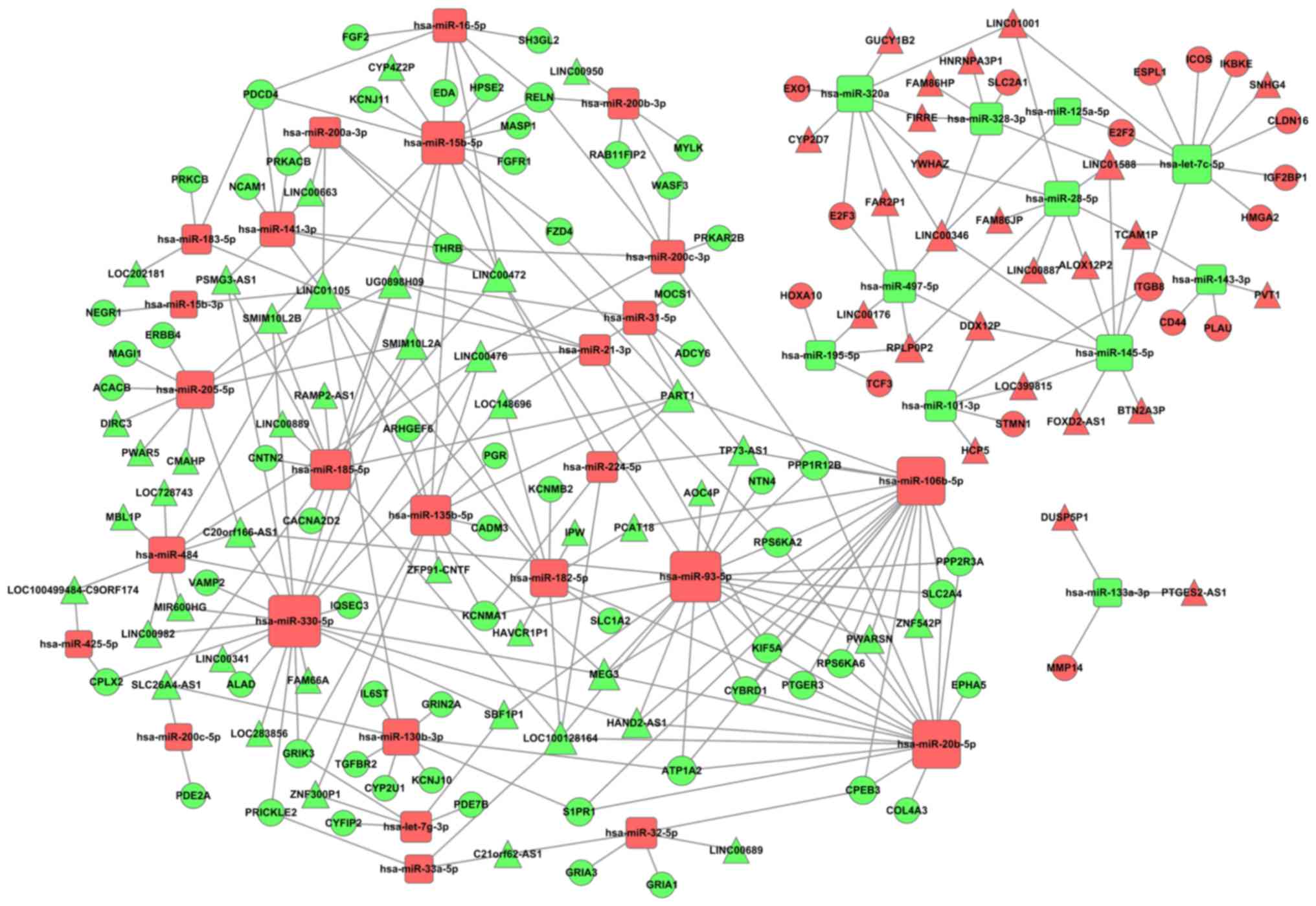
Construction of ceRNA network
In order to determine whether the intersection of
co-differentially expressed lncRNAs, miRNAs and mRNAs in GEO and
TCGA (Table V) exist in competing
endogenous regulating relationships, the intersected 81 lncRNAs, 39
miRNAs and 357 mRNAs were applied to construct the ceRNA network.
The aforementioned 39 miRNAs target lncRNAs and mRNAs were then
predicted based on MiRcode, miRanda and Targetscan. Subsequently,
the intersection genes of the abovementioned miRNAs target
predicted the lncRNAs and mRNAs to build the ceRNA network
(Table V). The ceRNA network was
visualized using Cytoscape software (version 3.0). The results
revealed that there were 67 lncRNAs, 37 miRNAs and 80 mRNAs
involved in the ceRNA network (Fig.
5). The detailed information of ceRNA network is presented in
Table SIII.
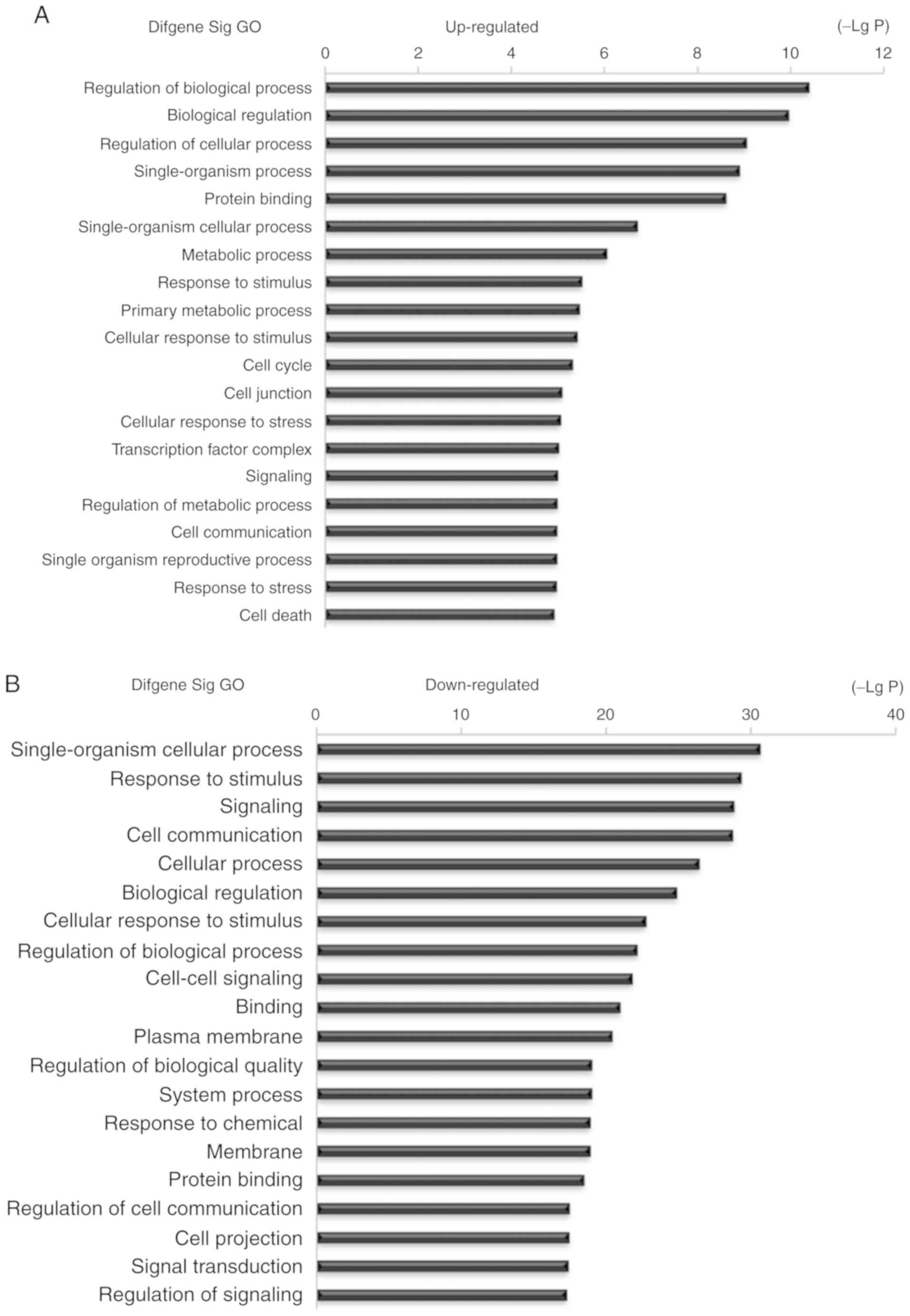
Functional analysis of mRNAs in the
ceRNA network
The present study identified 67 lncRNAs, 37 miRNAs
and 80 mRNAs involved in the ceRNA network. Therefore, it may be
suggested that the co-differentially expressed genes in the ESCC
tissues that were included in the ceRNA network may play key roles
in ESCC progression. Based on these suggestions, the present study
investigated the potential biological regulatory functions of these
80 mRNAs that were involved in the ceRNA network via GO enrichment
of functions and KEGG pathway analyses. The upregulated and
downregulated intersected mRNAs were further analyzed. The results
suggested that the most enriched GO function by upregulated mRNAs
was ‘Regulation of biological process (GO:0050789)’. The most
enriched GO function by downregulated mRNAs was ‘Single-organism
cellular process (GO:0044763)’ (Fig.
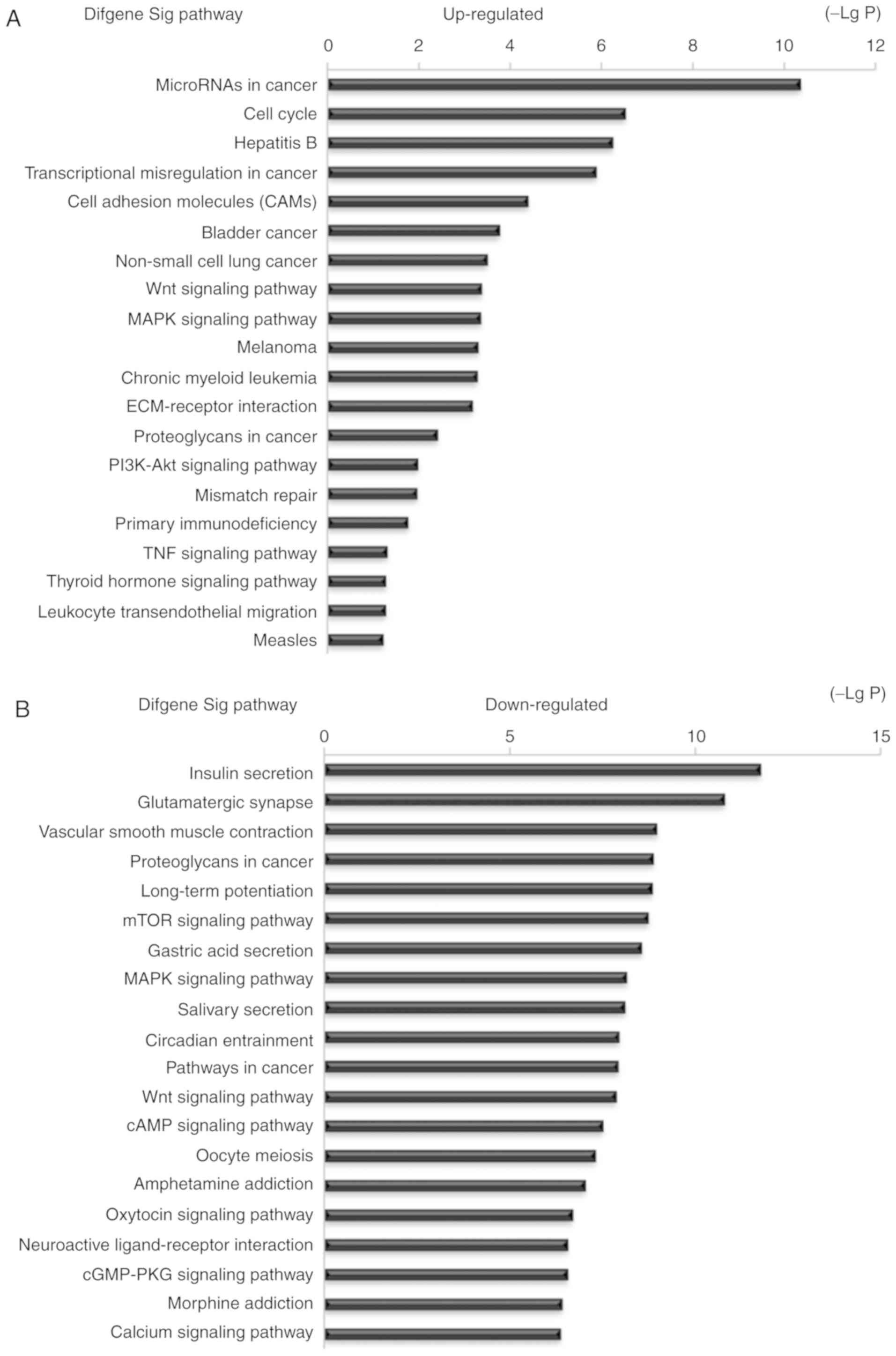
6). The KEGG pathway analysis indicated 25 signaling pathways
involved in regulating upregulated mRNAs, and the most enriched
pathway was ‘MicroRNAs in cancer (hsa05206)’. In addition, 95
signaling pathways were involved in regulating downregulated mRNAs,
and the most enriched pathway was ‘Insulin secretion (hsa04911)’.
Some of these signaling pathways, such as the ‘Wnt signaling
pathway’, were involved in the progression of ESCC (18), the ‘MAPK signaling pathway’ was
revealed as a key pathway affecting esophageal carcinoma cell
proliferation and apoptosis (19),
and the ‘mTOR signaling pathway’ was involved in the progression of
ESCC (20). Furthermore, ‘Bladder
cancer, Non-small-cell lung cancer, Pathways in cancer and PI3K-AKT
signaling pathway’ were also reported as cancer-associated
signaling pathways (21–24) (Fig.
7).
Association between lncRNA signature
and the clinical characteristics of patients with ESCC
The aforementioned 67 lncRNAs that were involved in
the ceRNA network were selected and further investigated in order
to identify the association between these key lncRNAs and TCGA
database with the clinicopathological characteristics of the 312
patients with ESCC. The ESCC patients' clinicopathological
characteristics included age, sex, race, tumor grade, TNM stage and
lymphatic metastasis, and were obtained from TCGA database. The
relevance analysis results suggested that 31 lncRNAs were
significantly differentially expressed in ESCC patients with
different clinicopathological characteristics (P<0.05). It was
revealed that PTGES2-AS1, CMAHP, LINC00472, LINC01105, BTN2A3P,
LOC728743, LINC00346, PSMG3-AS1, SBF1P1, LINC01588, DIRC3, RPLPOP2,
SMIM10L2A, ZNF300P1 and TP73-AS1 were associated with tumor grade;
LOC148696, HCP5, LOC148696, LINC00472, RPLP0P2, DDX12P, SMIM10L2A,
PVT1, ZNF300P1, SMIM10L2B and HAND2-AS1 were associated with TNM
stage; and PTGES2-AS1, FOXD2-AS1, LOC148696, TCAM1P, LINC00982,
LINC00176, DIRC3, ALOX12P2 and SBF1P1 were associated with
lymphatic metastasis in patients with ESCC. Furthermore, it was
indicated that PART1 and LINC00341 may be associated with sex and
race, respectively (Table VI).
| Table VI.Associations between lncRNA signature
and ESCC patients' clinicopathological characteristics. |
Table VI.
Associations between lncRNA signature
and ESCC patients' clinicopathological characteristics.
| Comparisons | Upregulated | Downregulated |
|---|
| Sex (male vs.
female) |
| C20orf166-AS1,
UG0898H09, PART1 |
| Race (Caucasian vs.
Asian) | ALOX12P2,
DUSP5P1 | PART1, LINC00341,
LINC00982, DIRC3 |
| Tumor grade | PTGES2-AS1,
LINC01588, BTN2A3P, | PSMG3-AS1, CMAHP,
LINC00472, LINC01105, |
| (GIII–IV vs.
GI–II) | LOC728743, RPLPOP2,
LINC00346 | SBF1P1, DIRC3,
SMIM10L2A, ZNF300P1, TP73-AS1 |
| TNM stage (T3 + T4
vs. T1 + T2) | RPLP0P2, DDX12P,
PVT1, HCP5 | LINC00472,
LOC148696, SMIM10L2A, ZNF300P1, SMIM10L2B, HAND2-AS1 |
| Lymphatic
metastasis (yes vs. no) | PTGES2-AS1,
FOXD2-AS1, TCAM1P, LINC00176 | DIRC3, LINC00982,
LOC148696, SBF1P1 |
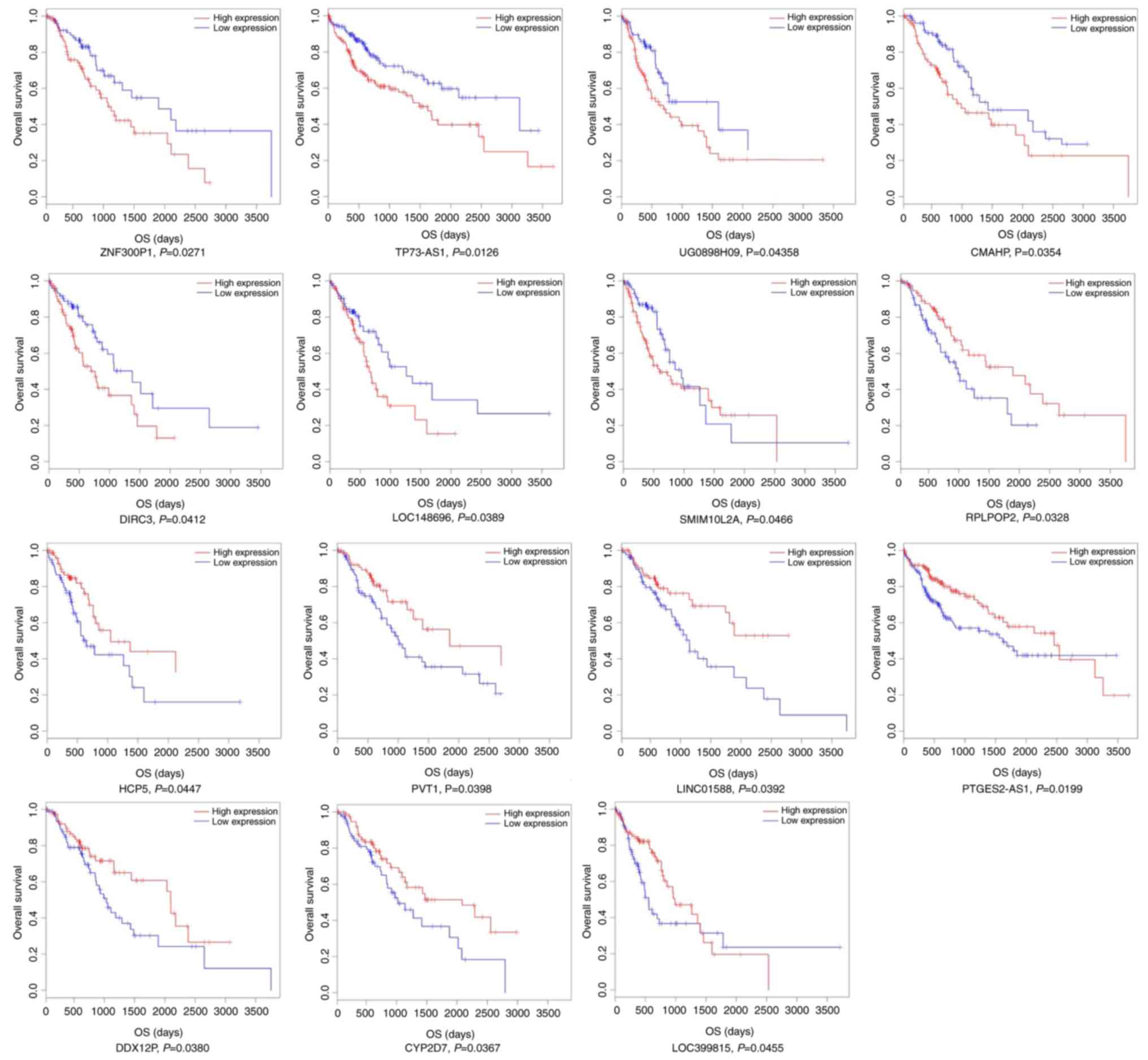
Prognostic analysis of lncRNA
expression levels and survival of patients with ESCC
Based on the RNA sequencing data and clinical
information of the patients with ESCC from TCGA, a Kaplan-Meier
survival analysis was used to identify the associations between the
ceRNA network 67 key lncRNAs and overall survival time of the ESCC
patients. The expression levels of these 67 key lncRNAs and ESCC
prognosis data in TCGA database were synthetically calculated using
a Cox proportional hazard regression model and it was revealed that
there were 15 lncRNAs statistically associated with the overall
survival rate (log-rank P<0.05). Among these 15 lncRNAs, 7
(ZNF300P1, TP73-AS1, UG0898H09, CMAHP, DIRC3, LOC148696 and
SMIM10L2A) were negatively associated with the prognosis of
patients with ESCC (P<0.05), and 8 (RPLPOP2, HCP5, PVT1,
LINC01588, PTGES2-AS1, DDX12P, CYP2D7 and LOC399815) were
positively associated with the prognosis of patients with ESCC
(P<0.05) (Fig. 8).
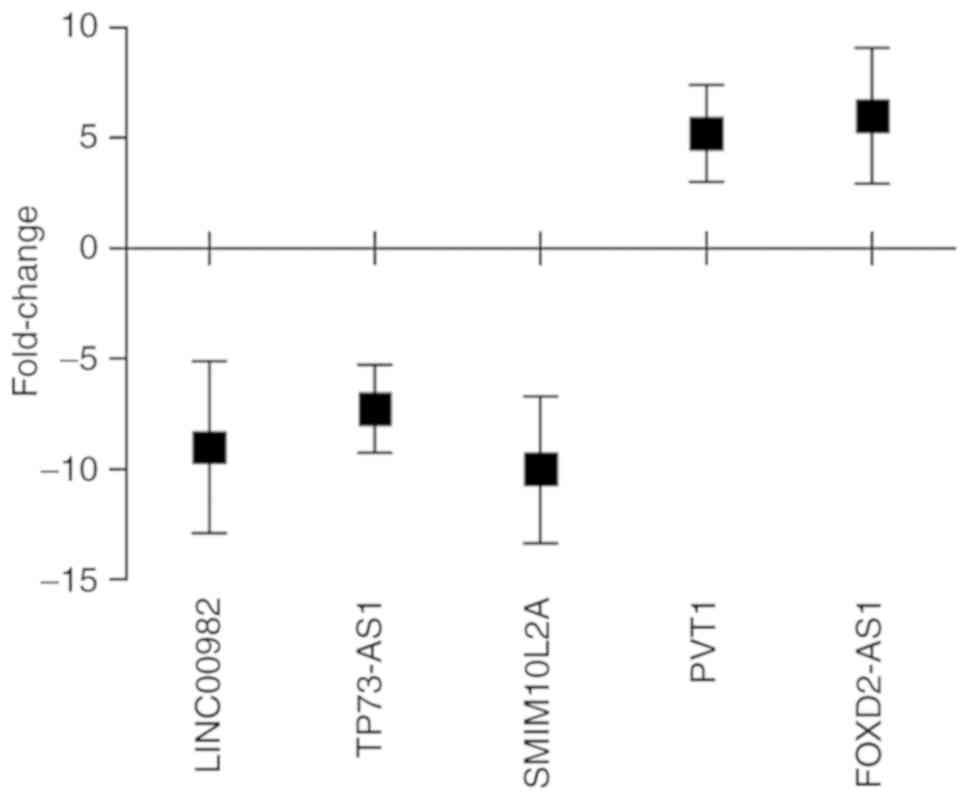
RT-qPCR validation
Through comprehensive analysis of the aforementioned
results, it was inferred that LINC00982, TP73-AS1, SMIM10L2A, PVT1
and FOXD2-AS1 may play important roles in ESCC progression.
Therefore, these five lncRNAs were selected and their actual
expression levels were detected in 30 patients with newly diagnosed
ESCC and paired non-tumor esophageal epithelial tissue samples via
RT-qPCR to assess the reliability and validity of the
bioinformatics analysis results (Tables
III and VII). The results
revealed that LINC00982, TP73-AS1 and SMIM10L2A were downregulated,
whereas PVT1 and FOXD2-AS1 were upregulated in ESCC tumor tissues
(Fig. 9). The results suggested that
the RT-qPCR validation in 30 newly diagnosed patients with ESCC and
the aforementioned bioinformatics analysis results (Table VII) exhibited the same trends
(Fig. 5).
| Table VII.Randomly selected lncRNAs with
absolute FC>2, P<0.05. |
Table VII.
Randomly selected lncRNAs with
absolute FC>2, P<0.05.
| Name (lncRNAs) | Gene ID | Regulation | TCGA (mean FC) | GEO (mean FC) |
|---|
| LINC00982 | 440556 | Down | −17.539 | −3.991 |
| TP73-AS1 | 57212 | Down | −3.845 | −5.579 |
| SMIM10L2A | 399668 | Down | −7.850 | −4.852 |
| PVT1 | 5820 | Up | 7.193 | 9.997 |
| FOXD2-AS1 | 84793 | Up | 6.470 | 14.211 |
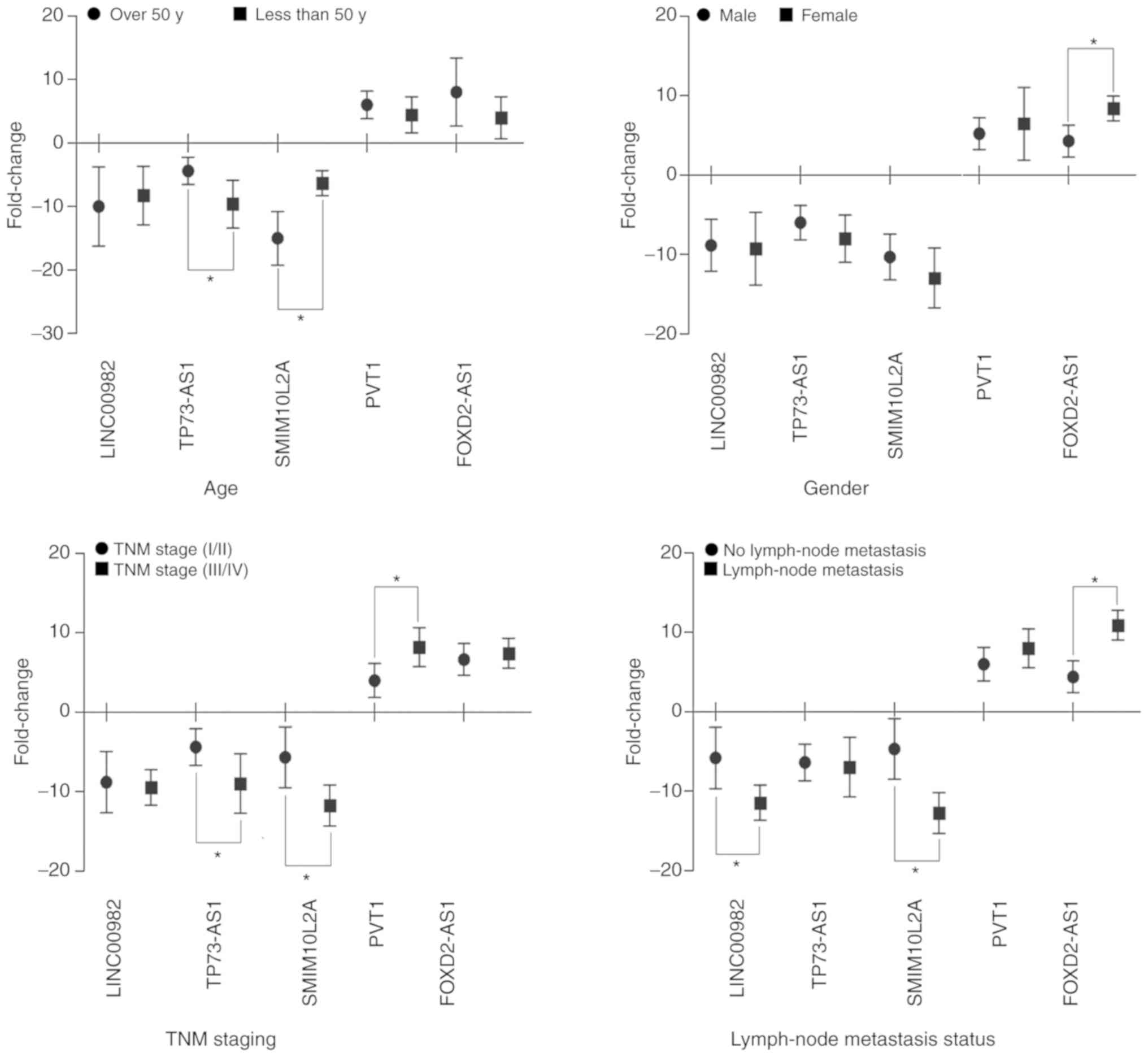
Subsequently, the association between the real
expression levels of the aforementioned 5 lncRNAs and the clinical
characteristics of the 30 newly diagnosed patients with ESCC was
assessed. The results revealed that TP73-AS1, SMIM10L2A and PVT1
were significantly associated with TNM stage (P<0.05), whereas
LINC00982, SMIM10L2A and FOXD2-AS1 were significantly associated
with lymph node metastasis status (P<0.05). In addition, it was
also revealed that TP73-AS1, SMIM10L2A and FOXD2-AS1 were
correlated with the age and sex of the patients with ESCC
(P<0.05; Fig. 10). The expression
levels of the 5 lncRNAs were detected, and the results from the
clinically relevant analysis and the aforementioned bioinformatics
analysis (Tables V and VII) were similar, suggesting that the
bioinformatics analysis used in the present study was credible.
Discussion
ESCC is a common malignant tumor originating from
the mucosa of the esophagus at vulnerable sites, including the
pharyngoesophageal junction, the part of the esophagus crossing
with the posterior surface of the left bronchus, and the part of
the esophagus passing through the diaphragmatic esophageal hiatus
(25). Gastrointestinal endoscopy
detection cannot identify all precancerous conditions or the early
stages of ESCC. The incidence and mortality rate of ESCC in the
general population are high, and a large number of patients are
usually diagnosed late and have a poor prognosis (26). In addition, ESCC lymph node metastasis
may be regional, bidirectional, continuous or jumping, and
effective complete eradication methods are currently lacking
(27). In order to improve survival
rate and the detection and treatment of early-stage ESCC, more
effective therapeutic tools are required, including the
identification of novel diagnostic and prognostic biomarkers.
Recent studies that have focused on the abnormal expression of
lncRNAs have revealed a new investigative approach to the
pathological changes observed in ESCC, and have also indicated that
the search for novel biomarkers may hold promise for ESCC diagnosis
and prognosis (28–30). The main concern is that small amounts
of RNA sequencing samples may not accurately reflect the abnormal
changes in lncRNAs when used as biomarkers that are associated with
the diagnosis and prognosis of ESCC (31,32).
Therefore, the ESCC-associated dysregulated lncRNA expression
profiles should be identified based on large sample sizes in order
to improve their accuracy and reliability as diagnostic and
prognostic markers.
The development of high throughput RNA sequencing
technologies has allowed thousands of dysregulated RNAs to be
observed in a number of diseases (33–36). The
present study identified abnormally expressed lncRNAs implicated in
the pathogenesis of ESCC by synthetically analyzing RNA sequencing
datasets obtained from the GEO and TCGA databases. A number of
studies have proved that integration of multiple RNA sequencing
datasets is a better method for enhancing the accuracy and
reliability of results compared with using individual small samples
(37). RNA sequencing allows
reannotation, identification of differentially expressed RNAs in
the GEO and TCGA databases, ceRNA network construction based on
gene discovery, association between key lncRNAs and clinical
characteristics of ESCC patients and survival analysis, in order to
investigate the potential biomarkers for the diagnosis and
prognosis of ESCC.
A multiple subset analysis and integrated
bioinformatics approach was applied in order to identify
dysregulated RNAs in ESCC in the present study. In order to
increase the gene information accuracy, the RNA sequencing signals
from the GEO database were matched to their chromosomal position
using the GENCODE tool. All dataset samples were used in order to
increase the sample numbers so as to avoid errors in the results
and narrow the gene objects range. In addition, to avoid errors
occurring from different ESCC individual tissues, only paired RNA
sequencing sample datasets were included in the GEO database.
According to the integrated bioinformatics approach,
it was revealed that there were 81 lncRNAs, 39 miRNAs and 357 mRNAs
co-differentially expressed ESCC-associated intersection genes
between the GEO and TCGA database. Among these 81 dysregulated
lncRNAs, some have been indicated to exhibit significantly
different expression levels in ESCC, including downregulated lncRNA
HAND2-AS1 which may act as an anti-oncogene that can inhibit ESCC
cell proliferation, migration and invasion (38). Dong et al (39) and Huang et al (40) have reported that downregulated MEG3 in
ESCC tissues can inhibit ESCC cell growth and induce apoptosis. In
addition, upregulated lncRNAs PVT1, TP73-AS1, UCA1 and ZFAS1 were
also reported to be significantly differentially expressed in
esophageal cancer, and also to be involved in regulating the
progression of this disease (41–44). To
the best of our knowledge, the functions of the remaining
dysregulated lncRNAs in the development and progression of ESCC
have not yet been reported.
Based on the theory that lncRNAs can regulate miRNA
abundance by sequestration binding, acting as ‘miRNA sponges’, and
the fact that miRNAs can bind to mRNAs and negatively regulate gene
expression (45), the present study
built an lncRNA-miRNA-mRNA ceRNA network according to their
negative regulatory associations. Among 81 ESCC-associated
intersection lncRNAs, a total of 67 key lncRNAs were included in
the lncRNA-miRNA-mRNA ceRNA network. The ceRNA network construction
can reveal the potential regulatory associations between lncRNAs,
miRNAs and mRNAs in ESCC. According to the ceRNA network created in
the present study, some of these 67 lncRNAs, such as FIRRE,
FOXD2-AS1, IPW and LINC00472, were also reported as potential
diagnostic and prognostic biomarkers in numerous human diseases,
including ESCC (46–49). In order to investigate the potential
regulatory functions of these 67 key lncRNAs, the present study
further analyzed the 80 negatively regulated mRNAs in the ceRNA
network, and revealed that some of those also play important roles
in the progression of ESCC, including CYBRD1, EDA, ERBB4, FGF2 and
IKBKE (50–52). Subsequently, the present study
analyzed the 67 key lncRNAs in the ceRNA network and identified
enrichment of the functions of 80 mRNAs that were indirectly
involved in signaling pathways. The GO analysis results revealed
that the enriched GOs primarily targeted the metabolism and cell
biological process. The KEGG analysis revealed that certain
pathways were also associated with cancer, such as the Wnt
signaling pathway, the MAPK signaling pathway, non-small cell lung
cancer, pathways in cancer and the PI3K-AKT signaling pathway
(53). Therefore, the present
bioinformatics analysis results revealed that these 67 key lncRNAs
in the ceRNA network may be implicated in the progression of
ESCC.
The associations between the expression levels of
the 67 aforementioned key lncRNAs and the clinicopathological
characteristics from TCGA database were analyzed, and it was
revealed that 32 lncRNAs were associated with the characteristics
of the 312 patients with ESCC. These lncRNAs were primarily
associated with tumor grade, TNM stage and lymphatic metastasis
status. Among these 31 lncRNAs, PVT1, FOXD2-AS1 and PART1 have been
reported to be the key genes involved in lymphatic metastasis and
invasion and as diagnostic biomarkers for ESCC (54–56).
However, the functions of other lncRNAs have not yet been reported
in association with ESCC progression. Therefore, the present study
also analyzed the association between the 67 key lncRNAs in the
ceRNA network and overall survival of patients with ESCC in TCGA
database. It was revealed that 15 lncRNAs were associated with
overall survival time. Among these 15 lncRNAs, only TP73-AS1 and
PVT1 have been reported to be associated with survival in ESCC
(42,57), whereas other lncRNAs have not been
reported to date. The bioinformatics analysis results in the
present study revealed potential lncRNAs biomarkers for the
diagnosis, classification and prognosis of ESCC.
Subsequently, RT-qPCR validation of 5 randomly
selected lncRNAs in 30 ESCC tissue samples was performed and the
accuracy and credibility of the bioinformatics results were
assessed. The results of the RT-qPCR validation were almost the
same as the expression data in the GEO and TCGA databases. The
present study then analyzed the association between these 5
randomly selected lncRNAs and the collected clinicopathological
data of the patients with ESCC. The results also suggested that the
results with these 5 lncRNAs were similar to the aforementioned
bioinformatics analysis results. Therefore, the synthetic
bioinformatics analysis results of the present study are
reliable.
In summary, the present study has successfully
identified specific ESCC-associated lncRNAs from large-scale
samples through integrated analysis of RNA expression profile
datasets of patients with ESCC from the GEO and TCGA databases.
Differentially expressed lncRNAs and their potential functions in
ESCC were investigated in the present study, along with specific
ESCC-associated lncRNAs by different clinicopathological
characteristics and overall survival time of patients with ESCC.
Overall, these 67 lncRNAs are worth investigating further in terms
of their applicability as biomarkers in the diagnosis,
clinicopathological classification and prognosis of patients with
ESCC.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by the Fundamental
Research Funds for the Central Universities (grant no.
lzujbky-2018-13), the National Natural Science Foundation of China
(grant no. 81803188), and the Gansu Province Science and Technology
Project (grant no. 1606RJYA270).
Availability of data and materials
The authors declare that all relevant raw data will
be made freely available to any researchers who wish to use them
for non-commercial purposes, whilst preserving any necessary
confidentiality and anonymity. All data generated or analyzed
during this study are included in this published article.
Authors' contributions
CYL conceived and designed the study. CYL and XHW
performed the experiments. WWZ, JLW and JL analyzed and interpreted
the results. JLX and XHW performed the patient tissue sample
collection and quality control. CYL performed analysis and quality
control, and was a major contributor to writing the manuscript. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Gansu Wuwei Tumor Hospital. All patients provided
written informed consent to participate in the present study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jiang C, Chen Y, Zhu Y and Xu Y:
Systematic review and meta-analysis of the accuracy of 18F-FDG
PET/CT for detection of regional lymph node metastasis in
esophageal squamous cell carcinoma. J Thorac Dis. 10:6066–6076.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kim M: Evaluation of a web-based App
demonstrating an exclusionary algorithmic approach to TNM cancer
staging. JMIR Cancer. 1:e32015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang X, Wang Y, Zhao L, Sang S and Zhang
L: Prognostic value of platelet-to-lymphocyte ratio in oncologic
outcomes of esophageal cancer: A systematic review and
meta-analysis. Int J Biol Markers. Apr 1–2018.(Epub ahead of
print). View Article : Google Scholar
|
|
5
|
Quan J, Pan X, Zhao L, Li Z, Dai K, Yan F,
Liu S, Ma H and Lai Y: LncRNA as a diagnostic and prognostic
biomarker in bladder cancer: A systematic review and meta-analysis.
Onco Targets Ther. 11:6415–6424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tian T, Wang M, Lin S, Guo Y, Dai Z, Liu
K, Yang P, Dai C, Zhu Y, Zheng Y, et al: The impact of lncRNA
dysregulation on clinicopathology and survival of breast cancer: A
systematic review and meta-analysis. Mol Ther Nucleic Acids.
12:359–369. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liu W, Zhang Y, Chen M, Shi L, Xu L and
Zou X: A genome-wide analysis of long noncoding RNA profile
identifies differentially expressed lncRNAs associated with
Esophageal cancer. Cancer Med. 7:4181–4189. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khadirnaikar S, Narayanan SP and Shukla
SK: Decoding the LncRNA transcriptome of esophageal cancer:
Identification of clinically relevant LncRNAs. Biomark Med.
12:1083–1093. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ji S, Yang W, Liu J, Zhao J, Chen L, Ni Q,
Long J and Yu X: High throughput gene sequencing reveals altered
landscape in DNA damage responses and chromatin remodeling in
sporadic pancreatic neuroendocrine tumors. Pancreatology.
18:318–327. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Krishnamurthy A, Ferl RJ and Paul AL:
Comparing RNA-Seq and microarray gene expression data in two zones
of the Arabidopsis root apex relevant to spaceflight. Appl Plant
Sci. 6:e011972018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hu J, Zhou L, Song Z, Xiong M, Zhang Y,
Yang Y, Chen K and Chen Z: The identification of new biomarkers for
bladder cancer: A study based on TCGA and GEO datasets. J Cell
Physiol. Feb 18–2019.(Epub ahead of print). View Article : Google Scholar
|
|
12
|
Su H, Hu N, Yang HH, Wang C, Takikita M,
Wang QH, Giffen C, Clifford R, Hewitt SM, Shou JZ, et al: Global
gene expression profiling and validation in esophageal squamous
cell carcinoma and its association with clinical phenotypes. Clin
Cancer Res. 17:2955–2966. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang Q, Ma C and Kemmner W: Wdr66 is a
novel marker for risk stratification and involved in
epithelial-mesenchymal transition of esophageal squamous cell
carcinoma. BMC Cancer. 13:1372013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wen J, Yang H, Liu MZ, Luo KJ, Liu H, Hu
Y, Zhang X, Lai RC, Lin T, Wang HY and Fu JH: Gene expression
analysis of pretreatment biopsies predicts the pathological
response of esophageal squamous cell carcinomas to
neo-chemoradiotherapy. Ann Oncol. 25:1769–1774. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Guo Y, Chen Z, Zhang L, Zhou F, Shi S,
Feng X, Li B, Meng X, Ma X, Luo M, et al: Distinctive microRNA
profiles relating to patient survival in esophageal squamous cell
carcinoma. Cancer Res. 68:26–33. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jang HJ, Lee HS, Burt BM, Lee GK, Yoon KA,
Park YY, Sohn BH, Kim SB, Kim MS, Lee JM, et al: Integrated genomic
analysis of recurrence-associated small non-coding RNAs in
oesophageal cancer. Gut. 66:215–225. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cao B, Yang W, Jin Y, Zhang M, He T, Zhan
Q, Herman JG, Zhong G and Guo M: Silencing NKD2 by promoter region
hypermethylation promotes esophageal cancer progression by
activating Wnt signaling. J Thorac Oncol. 11:1912–1926. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang X, Zhu Y, Zhu L, Chen X, Xu Y, Zhao
Y, Shao Y, Li F, Jiang Y, Lu J, et al: Eupatilin inhibits the
proliferation of human esophageal cancer TE1 cells by targeting the
Akt-GSK3β and MAPK/ERK signaling cascades. Oncol Rep. 39:2942–2950.
2018.PubMed/NCBI
|
|
20
|
Jiang JH, Pi J, Jin H and Cai JY:
Oridonin-induced mitochondria-dependent apoptosis in esophageal
cancer cells by inhibiting PI3K/AKT/mTOR and Ras/Raf pathways. J
Cell Biochem. 120:3736–3746. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
He J, Zhao J, Zhu W, Qi D, Wang L, Sun J,
Wang B, Ma X, Dai Q and Yu X: MicroRNA biogenesis pathway genes
polymorphisms and cancer risk: A systematic review and
meta-analysis. PeerJ. 4:e27062016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hu M, Zhu S, Xiong S, Xue X and Zhou X:
MicroRNAs and the PTEN/PI3K/Akt pathway in gastric cancer (Review).
Oncol Rep. 41:1439–1454. 2019.PubMed/NCBI
|
|
23
|
Xiao YF, Yong X, Tang B, Qin Y, Zhang JW,
Zhang D, Xie R and Yang SM: Notch and Wnt signaling pathway in
cancer: Crucial role and potential therapeutic targets (Review).
Int J Oncol. 48:437–449. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Toren P and Zoubeidi A: Targeting the
PI3K/Akt pathway in prostate cancer: Challenges and opportunities
(Review). Int J Oncol. 45:1793–1801. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hayashi Y, Nishida T, Tsujii M, Tsutsui S,
Yamamoto K, Isohashi F, Yamasaki M, Miyata H, Kato M, Yamada T, et
al: Lymph node enlargement after definitive chemoradiotherapy for
clinical stage I esophageal squamous cell carcinoma. BMC Cancer.
14:7062014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cheng YF, Chen HS, Wu SC, Chen HC, Hung
WH, Lin CH and Wang BY: Esophageal squamous cell carcinoma and
prognosis in Taiwan. Cancer Med. 7:4193–4201. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mine S, Watanabe M, Kumagai K, Okamura A,
Yuda M, Hayami M, Yamashita K, Imamura Y and Ishizuka N: Comparison
of mediastinal lymph node metastases from adenocarcinoma of the
esophagogastric junction versus lower esophageal squamous cell
carcinoma with involvement of the esophagogastric junction. Dis
Esophagus. Feb 22–2019.(Epub ahead of print). View Article : Google Scholar :
|
|
28
|
Huang GW, Xue YJ, Wu ZY, Xu XE, Wu JY, Cao
HH, Zhu Y, He JZ, Li CQ, Li EM and Xu LY: A three-lncRNA signature
predicts overall survival and disease-free survival in patients
with esophageal squamous cell carcinoma. BMC Cancer. 18:1472018.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang J, Sun D, Wu K, Liu J, Zhao M, Li X,
Xu Y and Li B: Genome-wide analysis of long non-coding RNAs in
esophageal squamous cell carcinoma reveals their potential role in
invasion and metastasis. Thorac Cancer. 10:78–89. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Alaei S, Sadeghi B, Najafi A and
Masoudi-Nejad A: LncRNA and mRNA integration network reconstruction
reveals novel key regulators in esophageal squamous-cell carcinoma.
Genomics. 111:76–89. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Campbell JD, Liu G, Luo L, Xiao J, Gerrein
J, Juan-Guardela B, Tedrow J, Alekseyev YO, Yang IV, Correll M, et
al: Assessment of microRNA differential expression and detection in
multiplexed small RNA sequencing data. RNA. 21:164–171. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Collins JE, Wali N, Sealy IM, Morris JA,
White RJ, Leonard SR, Jackson DK, Jones MC, Smerdon NC, Zamora J,
et al: High-throughput and quantitative genome-wide messenger RNA
sequencing for molecular phenotyping. BMC Genomics. 16:5782015.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ozsolak F: Attomole-level genomics with
single-molecule direct DNA, cDNA and RNA sequencing technologies.
Curr Issues Mol Biol. 18:43–48. 2016.PubMed/NCBI
|
|
34
|
Lacaze É, Gendron AD, Miller JL, Colson
TL, Sherry JP, Giraudo M, Marcogliese DJ and Houde M: Cumulative
effects of municipal effluent and parasite infection in yellow
perch: A field study using high-throughput RNA-sequencing. Sci
Total Environ. 665:797–809. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ge L, Liu S, Xie L, Sang L, Ma C and Li H:
Differential mRNA expression profiling of oral squamous cell
carcinoma by high-throughput RNA sequencing. J Biomed Res.
29:2015.(Epub ahead of print). PubMed/NCBI
|
|
36
|
Gao M, Zhong A, Patel N, Alur C and Vyas
D: High throughput RNA sequencing utility for diagnosis and
prognosis in colon diseases. World J Gastroenterol. 23:2819–2825.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ma T, Liang F, Oesterreich S and Tseng GC:
A joint bayesian model for integrating microarray and RNA
sequencing transcriptomic data. J Comput Biol. 24:647–662. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yan Y, Li S, Wang S, Rubegni P, Tognetti
L, Zhang J and Yan L: Long noncoding RNA HAND2-AS1 inhibits cancer
cell proliferation, migration, and invasion in esophagus squamous
cell carcinoma by regulating microRNA-21. J Cell Biochem.
120:9564–9571. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Dong Z, Zhang A, Liu S, Lu F, Guo Y, Zhang
G, Xu F, Shi Y, Shen S, Liang J and Guo W: Aberrant
methylation-mediated silencing of lncRNA MEG3 functions as a ceRNA
in esophageal cancer. Mol Cancer Res. 15:800–810. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Huang ZL, Chen RP, Zhou XT, Zhan HL, Hu
MM, Liu B, Wu GD and Wu LF: Long non-coding RNA MEG3 induces cell
apoptosis in esophageal cancer through endoplasmic reticulum
stress. Oncol Rep. 37:3093–3099. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yang S, Ning Q, Zhang G, Sun H, Wang Z and
Li Y: Construction of differential mRNA-lncRNA crosstalk networks
based on ceRNA hypothesis uncover key roles of lncRNAs implicated
in esophageal squamous cell carcinoma. Oncotarget. 7:85728–85740.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Zang W, Wang T, Wang Y, Chen X, Du Y, Sun
Q, Li M, Dong Z and Zhao G: Knockdown of long non-coding RNA
TP73-AS1 inhibits cell proliferation and induces apoptosis in
esophageal squamous cell carcinoma. Oncotarget. 7:19960–19974.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhou XL, Wang WW, Zhu WG, Yu CH, Tao GZ,
Wu QQ, Song YQ, Pan P and Tong YS: High expression of long
non-coding RNA AFAP1-AS1 predicts chemoradioresistance and poor
prognosis in patients with esophageal squamous cell carcinoma
treated with definitive chemoradiotherapy. Mol Carcinog.
55:2095–2105. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Shi H, Liu Z, Pei D, Jiang Y, Zhu H and
Chen B: Development and validation of nomogram based on lncRNA
ZFAS1 for predicting survival in lymph node-negative esophageal
squamous cell carcinoma patients. Oncotarget. 8:59048–59057.
2017.PubMed/NCBI
|
|
45
|
Wang P, Guo Q, Gao Y, Zhi H, Zhang Y, Liu
Y, Zhang J, Yue M, Guo M, Ning S, et al: Improved method for
prioritization of disease associated lncRNAs based on ceRNA theory
and functional genomics data. Oncotarget. 8:4642–4655.
2017.PubMed/NCBI
|
|
46
|
Hu Q, Tai S and Wang J: Oncogenicity of
lncRNA FOXD2-AS1 and its molecular mechanisms in human cancers.
Pathol Res Pract. 215:843–848. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Stelzer Y, Sagi I, Yanuka O, Eiges R and
Benvenisty N: The noncoding RNA IPW regulates the imprinted
DLK1-DIO3 locus in an induced pluripotent stem cell model of
Prader-Willi syndrome. Nat Genet. 46:551–557. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Zang Y, Zhou X, Wang Q, Li X and Huang H:
LncRNA FIRRE/NF-kB feedback loop contributes to OGD/R injury of
cerebral microglial cells. Biochem Biophys Res Commun. 501:131–138.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Su C, Shi K, Cheng X, Han Y, Li Y, Yu D
and Liu Z: Long noncoding RNA LINC00472 inhibits proliferation and
promotes apoptosis of lung adenocarcinoma cells via regulating
miR-24-3p/DEDD. Technol Cancer Res Treat. 17:15330338187904902018.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Lu T, Chen D, Wang Y, Sun X, Li S, Miao S,
Wo Y, Dong Y, Leng X, Du W and Jiao W: Identification of DNA
methylation-driven genes in esophageal squamous cell carcinoma: A
study based on the cancer genome atlas. Cancer Cell Int. 19:522019.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Yang W, Qu Y, Tan B, Jia Y, Wang N, Hu P
and Wang J: Prognostic significance of preoperative IKBKE
expression in esophageal squamous cell carcinoma. Onco Targets
Ther. 11:1305–1314. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Maehara O, Suda G, Natsuizaka M, Ohnishi
S, Komatsu Y, Sato F, Nakai M, Sho T, Morikawa K, Ogawa K, et al:
Fibroblast growth factor-2-mediated FGFR/Erk signaling supports
maintenance of cancer stem-like cells in esophageal squamous cell
carcinoma. Carcinogenesis. 38:1073–1083. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Unger JM, Vaidya R, Hershman DL, Minasian
LM and Fleury ME: Systematic review and meta-analysis of the
magnitude of structural, clinical, and physician and patient
barriers to cancer clinical trial participation. J Natl Cancer
Inst. 111:245–255. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Li PD, Hu JL, Ma C, Ma H, Yao J, Chen LL,
Chen J, Cheng TT, Yang KY, Wu G, et al: Upregulation of the long
non-coding RNA PVT1 promotes esophageal squamous cell carcinoma
progression by acting as a molecular sponge of miR-203 and LASP1.
Oncotarget. 8:34164–34176. 2017.PubMed/NCBI
|
|
55
|
Bao J, Zhou C, Zhang J, Mo J, Ye Q, He J
and Diao J: Upregulation of the long noncoding RNA FOXD2-AS1
predicts poor prognosis in esophageal squamous cell carcinoma.
Cancer Biomark. 21:527–533. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Kang M, Ren M, Li Y, Fu Y, Deng M and Li
C: Exosome-mediated transfer of lncRNA PART1 induces gefitinib
resistance in esophageal squamous cell carcinoma via functioning as
a competing endogenous RNA. J Exp Clin Cancer Res. 37:1712018.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Chen LP, Wang H, Zhang Y, Chen QX, Lin TS,
Liu ZQ and Zhou YY: Robust analysis of novel mRNA-lncRNA cross talk
based on ceRNA hypothesis uncovers carcinogenic mechanism and
promotes diagnostic accuracy in esophageal cancer. Cancer Manag
Res. 11:347–358. 2018. View Article : Google Scholar : PubMed/NCBI
|