Introduction
Malignant mesothelioma is a tumor that is primarily
caused by exposure to asbestos, including crocidolite, amosite, and
chrysotile (1). Mesothelioma is one
of the most lethal tumors, with an expected median survival time of
4–18 months for pleural forms (2).
There are three main histological types of mesothelioma:
Epithelioid, biphasic and sarcomatoid (2). Clinically, patients with the
sarcomatoid subtype have the poorest prognosis (3). The molecular mechanisms of
asbestos-induced mesothelial carcinogenesis have been recently
revealed to include oxidative stress, chronic inflammation,
molecular adsorption, and chromosome tangling (4–8). It is
necessary to understand the molecular mechanisms that regulate
mesothelial carcinogenesis (9–14) and
to develop molecular-targeted drugs (15) to improve the prognosis of
patients.
Mesothelioma often features a profound desmoplastic
reaction since asbestos can develop fibrotic diseases before
mesothelial carcinogenesis (1,2,11),
suggesting the involvement of cancer-associated fibroblasts (CAFs)
in its progression. CAFs occupy the majority of the area in the
tumor stroma and produce extracellular matrix (16–20).
One of the most well-known CAF markers is α-smooth muscle actin
(αSMA). In general, CAFs have been shown to exert protumorigenic
effects by promoting cancer cell proliferation and invasion.
However, recent studies have shown that CAFs are heterogeneous, and
the existence of a type of CAF with antitumor functions has been
proposed (19–23). Studies of CAF heterogeneity have led
to the proposal of multiple CAF markers (16–23).
Connective tissue growth factor (CTGF) is known as a protumorigenic
CAF marker (18–20). CTGF is a 36–38 kDa multifunctional
secretory protein involved in various functions, including cell
proliferation, cell invasion and myofibroblast differentiation. We
previously demonstrated that CTGF expression is correlated with the
malignant behavior of mesothelioma cells (13) and that a CTGF-specific monoclonal
antibody (FG-3019, pamrevlumab), which is currently under clinical
trials for idiopathic pulmonary fibrosis (24,25)
and pancreatic ductal adenocarcinoma (26), was found to inhibit mesothelioma
growth (15). Interestingly, we
found that CTGF is expressed in both mesothelioma cells and CAFs
(15). In contrast, mesenchymal
stromal cell- and fibroblast-expressing Linx paralogue (Meflin;
ISLR) is a glycosylphosphatidylinositol (GPI)-anchored
membrane protein, which has been identified as a marker of
mesenchymal stem cells and tissue-resident fibroblasts (27,28).
The results of our recent study suggest that Meflin is a potential
new marker of antitumorigenic CAFs (29).
Although the functions and heterogeneity of CAFs
have been recognized in other tumors, those in the mesothelioma
microenvironment have not yet been addressed. We aimed to
understand the significance of stromal remodeling during
mesothelioma progression. In the present study, we examined the
correlations between patient prognosis and the extent of fibrosis,
the expression of CAF markers (αSMA, CTGF and Meflin), and the
expression of a cell proliferation marker (Ki-67).
Materials and methods
Patients
A total of 37 patients underwent surgery for
malignant pleural mesothelioma at the Nagoya University Hospital
between January 2007 and December 2016. All patients were reviewed
for age, sex, histological subtype, pathological invasion (pT),
lymph node metastasis (pN), and neoadjuvant therapy. Tumor
classification was performed based on the TNM Classification of
Malignant Tumors (UICC) 7th edition (30). Patients who had another cancer, who
had undergone several surgeries, or who had undergone only
cytoreductive surgery were excluded. Based on histological and
immunohistochemical analyses, patients with the biphasic or
sarcomatoid subtype were also excluded because of the difficulty in
distinguishing the mesothelioma cells from CAFs. In total, 22
samples were ultimately analyzed. Human mesothelioma tissues were
obtained with informed patient consent at the time of surgery at
Nagoya University Hospital (Nagoya, Japan). This study was carried
out in accordance with the principles of the Helsinki Declaration
for human research and approved by the Ethics Committee of Nagoya
University Graduate School of Medicine (protocol no.
2017-0127).
Histologic and immunohistochemical
analysis
Four-micron- thick serial sections were cut from
formalin-fixed and paraffin-embedded tissue and were stained with
hematoxylin and eosin (H&E) or Elastica-Masson or for
immunohistochemistry (IHC). The following antibodies were used for
IHC: Anti-CTGF (goat polyclonal, dilution 1:50; Santa Cruz
Biotechnology, Inc.; cat. no. 14939), anti-AE1/AE3 (mouse
monoclonal, dilution 1:100; Biocare Medical; cat. no. ACR011A, B,
C), anti-Ki-67, clone SP6 (rabbit monoclonal, dilution 1:100;
Abcam; cat. no. 16667), and anti-αSMA (mouse monoclonal, dilution
1:50; Dako; cat. no. M0851). High-temperature antigen retrieval for
CTGF and Ki-67 was performed using Immunosaver (Nisshin EM, Tokyo,
Japan) and that for αSMA and AE1/AE3 was performed using 10 mM
Tris (hydroxymethyl) aminomethane/1 mM
ethylenediaminetetraacetic acid (TE) buffer, pH 9.0. Following
antigen retrieval, the sections were dipped for 30 min in methanol
containing H2O2 (0.3% vol/vol) to quench
endogenous peroxidase activity and subsequently blocked with
Protein Block Serum-Free Ready-to-use (Dako). For CTGF staining,
the avidin-biotin complex method using peroxidase was employed, as
previously described (31). For
AE1/AE3, Ki-67, and αSMA staining, Histofine Simple Stain MAX-PO
(Multi; Nichirei, Tokyo, Japan) was used as the secondary antibody.
Color development was performed with 3,3′-diaminobenzidine (DAB,
Dako) or HistoGreen (EUROBIO/ABCYS, Courtaboeuf, France). All
images were obtained using an Olympus BX53 microscope (Olympus,
Japan; objective lens PlanApo N 2X and U PlanApo 4X and 10X) and a
DP22/U-TV0.5XC camera.
Double staining IHC with primary
antibodies raised in the same species
We performed double staining for αSMA and AE1/AE3.
DAB was used to stain αSMA in the first step, and HistoGreen was
used to stain AE1/AE3 in the second step. Because both antibodies
are mouse monoclonal, high-temperature TE buffer was used to
inactivate the anti-αSMA antibody after DAB staining.
Semiquantitative imaging analysis of
the fibrotic and αSMA area indices in tumors
The entire tumor mass of each specimen was digitized
using the microscope and camera described above. Based on previous
studies (15,32), we analyzed the images using ImageJ
1.50i (http://rsb.info.nih.gov/ij/) and the
color deconvolution plugin (http://imagej.net/Colour_Deconvolution) for ImageJ and
Fiji to implement staining separation via the method of Ruifrok and
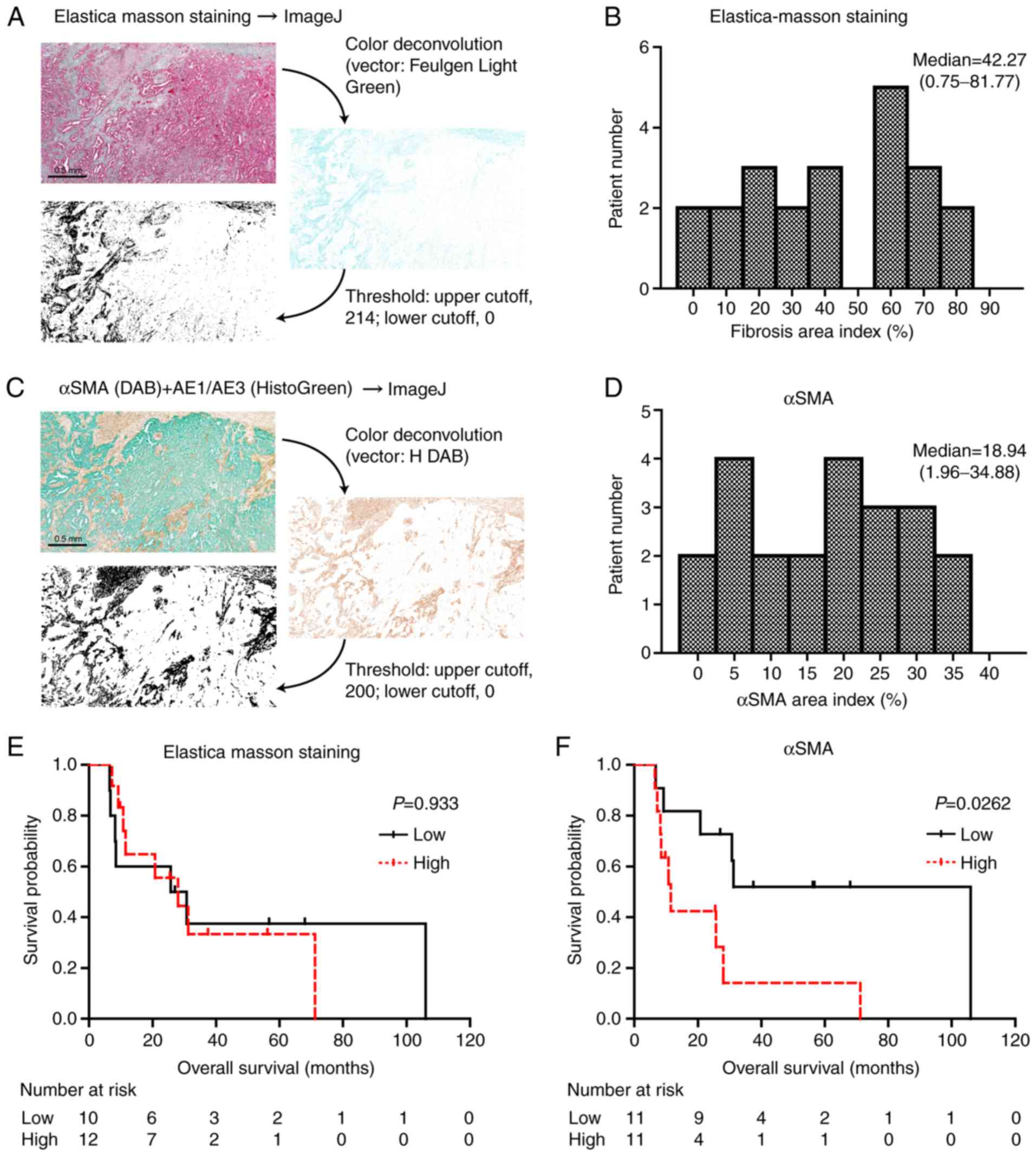
Johnston (33). Fibrosis was
detected as a light green color in Elastica-Masson staining. The
light-green positive area was extracted with the color
deconvolution plugin (vector: Feulgen Light Green), and the area
was converted to black (threshold: Upper cutoff, 214; lower cutoff,
0). After this processing, most of the remaining pixels in the
image were those originally stained in light green, and we
calculated the total area occupied by these pixels. This area was
divided by the entire tumor area, and the extent of fibrosis
(fibrotic area index) was determined as previously described
(15). To obtain the αSMA-positive
area (αSMA area index) and AE1/AE3-positive area in the entire
tumor, we used the same method used to determine the fibrotic area
index (vector: H DAB; threshold: Upper cutoff, 200; lower cutoff,
0). Most of the cases had the reactive pleural fibrosis with
mesothelioma cell invasion. For the fibrotic and αSMA area indices,
we evaluated the entire tumor mass including pleural fibrosis since
invasion to parietal and visceral pleura is a common pattern of
mesothelioma invasion (2) and since
the fibrosis can contribute to mesothelioma progression. To
minimize the influence of tumor heterogeneity, all the fields in
the entire tumor were evaluated. The average of each entire tumor
mass area was 141.7 mm2. We used a 2× objective lens and
the average fields of view for each tumor mass was 7.6.
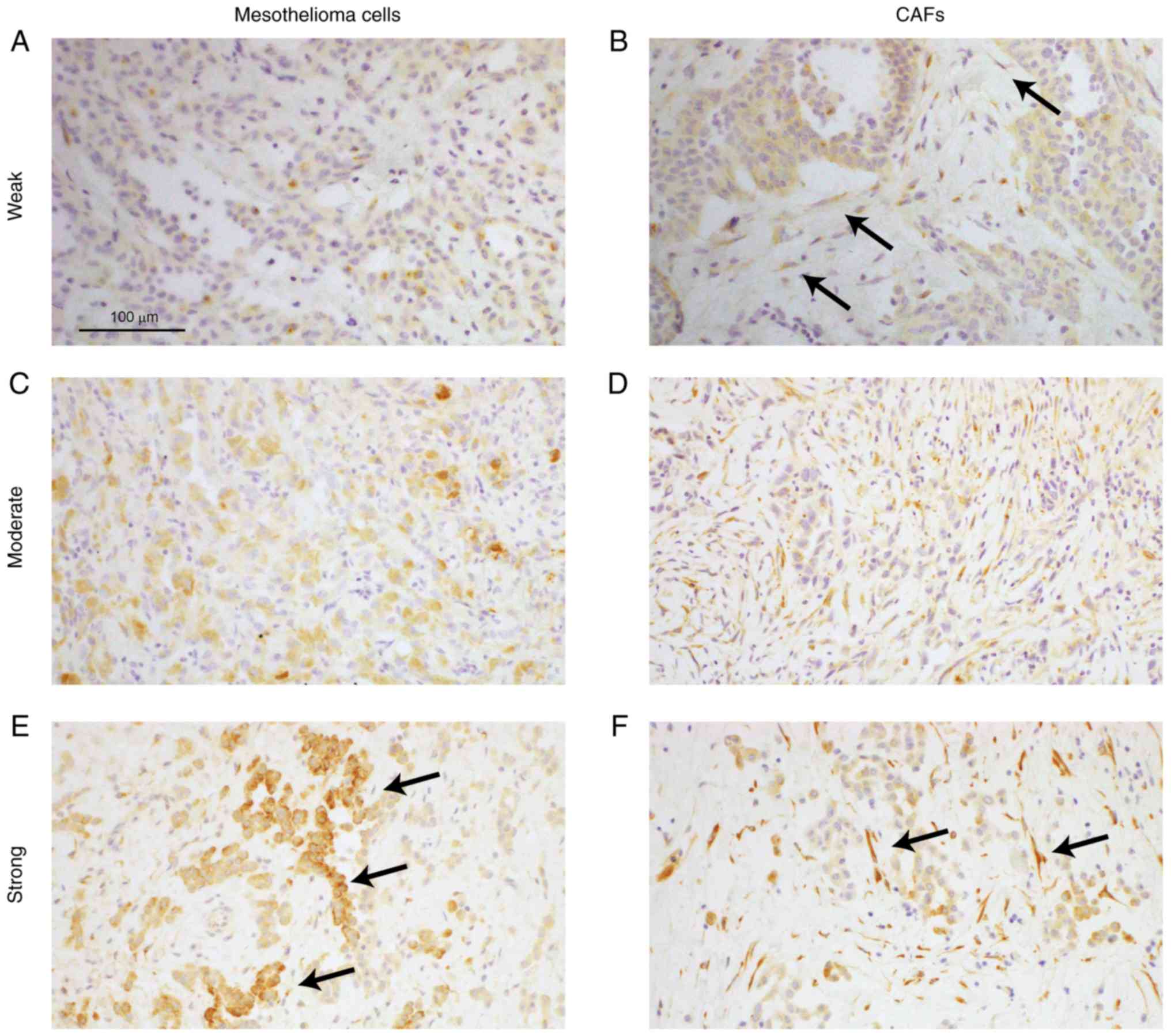
Semiquantitative analysis of CTGF
expression in tumors
We used the entire tumor mass of each specimen. The
CTGF immunostaining intensity in mesothelioma cells and CAFs was
assessed as follows: 0, negative; 1, weak; 2, moderate; and 3,
strong. In addition, the H-score for CTGF (CTGF score) was
calculated using the following formula: [1× (% of cells with an
intensity of 1)+2× (% of cells with an intensity of 2)+3× (% of
cells with an intensity of 3)] (34,35).
All the fields were evaluated by a registered pathologist (YO). The
average of each entire tumor mass area was 141.7 mm2. We
used a 4× objective lens and the average fields of view for each
tumor mass was 24.4. For the Kaplan-Meier survival curve, the CTGF
score for mesothelioma cells and CAFs was modified by the tumor
area (AE1/AE3-positive area) and stromal area (αSMA-positive area)
as follows: (CTGF score × AE1/AE3 or αSMA area index). Using these
modified CTGF scores, the patients were divided into two groups
(low or high).
In situ hybridization of Meflin
In situ hybridization (ISH) analysis was
performed using four-micron-thick formalin-fixed and
paraffin-embedded human tissue sections with the RNAscope
technology (RNAscope 2.5 HD Detection Kit; Advanced Cell
Diagnostics) and a custom-designed probe of human Meflin according
to the manufacturer's instructions, as previously described
(28,29). Briefly, tissue sections were baked
in a dry oven (HybEZ II Hybridization System; Advanced Cell
Diagnostics) at 60°C for 1 h, deparaffinized, and incubated with
H2O2 solution (Pretreat 1 buffer) for 10 min
at room temperature. The slides were boiled in target retrieval
solution (Pretreat 2 buffer) for 30 min, incubated with protease
solution (Pretreat 3 buffer) for 30 min at 40°C, incubated with the
probe for 2 h at 40°C, and then successively incubated with Amp1 to
6 reagents. Staining was visualized with DAB, followed by
counterstaining with hematoxylin. The RNAscope probe was as
follows: Human Meflin (ISLR) (NM_005545.3, region 275–1322;
cat. no. 455481). The slides were evaluated, as previously
described (29).
ImageJ software was used for obtaining the merged
image of αSMA + AE1/AE3 and Meflin. To detect the Meflin-positive
area, we used the same method used to determine the αSMA area index
(vector: H DAB; threshold: Upper cutoff, 190; lower cutoff, 0). The
Meflin-positive area was indicated by red color and merged with
αSMA + AE1/AE3 using Image Calculator.
Statistical analysis
The data were analyzed using GraphPad Prism 5
(GraphPad Software). The correlation between the expression of CAF
markers and various clinicopathological features was analyzed by
the Fisher's exact test. Correlation analysis was performed using
non-parametric method (Spearman's rank correlation coefficient).
The overall survival rate was calculated according to the
Kaplan-Meier method and compared using the Log-rank test if not
indicated otherwise. Gehan-Breslow-Wilcoxon test was used if
crossover between the groups was observed at late timepoints. A
P-value of <0.05 was considered as indicative of statistical
significance.
Results
αSMA-positive (αSMA+) CAFs
correlate with patient prognosis
Through H&E, IHC staining of αSMA + AE1/AE3, and
Elastica-Masson staining, a high extent of fibrosis was observed in
the reactive pleura present adjacent to mesothelioma (Fig. S1). To confirm the correlation
between fibrosis or CAFs and mesothelioma patient features, we
first evaluated the density of fibrosis and the presence of CAFs
expressing αSMA using paraffin-embedded sections of mesothelioma
samples. Although epithelioid mesothelioma is positive for AE1/AE3
(2,36), approximately 20% of sarcomatoid
mesothelioma is negative for AE1/AE3 (37,38).
In addition, it has been reported that reactive spindle cells can
be positive for AE1/AE3 in sarcomatoid mesothelioma (39). Although the H&E and IHC staining
distinguished mesothelioma cells from CAFs in epithelioid
mesothelioma (Fig. S2), our cases
of biphasic or sarcomatoid mesothelioma contained cells for which
it was difficult to clarify whether they were mesothelioma cells or
CAFs. Thus, we excluded cases of biphasic and sarcomatoid
mesothelioma. The area indices of fibrosis and αSMA were quantified
based on color deconvolution (Fig.
1A-D), and the clinicopathological findings are summarized
(Tables I and II). The indices of fibrosis and αSMA did
not correlate with the clinicopathological features. In addition,
no significant differences in overall survival were found based on
the fibrotic area index (Fig. 1E).
However, a significant difference (P=0.0262) was found based on the
αSMA area index (Fig. 1F).
 | Table I.Fibrotic area index and
clinicopathological features of the mesothelioma cases. |
Table I.
Fibrotic area index and
clinicopathological features of the mesothelioma cases.
|
Characteristics | Low | High | P-value |
|---|
| Age (years) |
|
| 0.670 |
|
<65 | 6 | 5 |
|
|
≥65 | 4 | 7 |
|
| Sex |
|
| 0.571 |
|
Male | 8 | 11 |
|
|
Female | 2 | 1 |
|
| Pathological
invasion |
|
| 0.074 |
| pT1 or
pT2 | 6 | 2 |
|
| pT3 or
pT4 | 4 | 10 |
|
| Lymph node
metastasis |
|
| 0.391 |
|
pN0 | 4 | 8 |
|
| pN1 or
pN2 | 6 | 4 |
|
| Stage |
|
| 0.624 |
| I or
II | 3 | 2 |
|
| III or
IV | 7 | 10 |
|
| Neoadjuvant
chemotherapy |
|
| 0.348 |
|
Absent | 4 | 2 |
|
|
Present | 6 | 10 |
|
|
Chemosensitivity |
|
| >0.999 |
| Grade 0
or 1a | 4 | 7 |
|
| Grade
1b or 2 | 2 | 3 |
|
| Table II.αSMA area index and
clinicopathological features of the mesothelioma cases. |
Table II.
αSMA area index and
clinicopathological features of the mesothelioma cases.
|
Characteristics | Low | High | P-value |
|---|
| Age (years) |
|
| >0.999 |
|
<65 | 6 | 5 |
|
|
≥65 | 5 | 6 |
|
| Sex |
|
| >0.999 |
|
Male | 10 | 9 |
|
|
Female | 1 | 2 |
|
| Pathological
invasion |
|
| 0.183 |
| pT1 or
pT2 | 6 | 2 |
|
| pT3 or
pT4 | 5 | 9 |
|
| Lymph node
metastasis |
|
| 0.670 |
|
pN0 | 7 | 5 |
|
| pN1 or
pN2 | 4 | 6 |
|
| Stage |
|
| 0.311 |
| I or
II | 4 | 1 |
|
| III or
IV | 7 | 10 |
|
| Neoadjuvant
chemotherapy |
|
| 0.635 |
|
Absent | 4 | 2 |
|
|
Present | 7 | 9 |
|
|
Chemosensitivity |
|
| 0.596 |
| Grade 0
or 1a | 4 | 7 |
|
| Grade
1b or 2 | 3 | 2 |
|
CTGF-positive (CTGF+) CAFs
correlate with mesothelioma cell proliferation and patient
prognosis
To confirm CTGF as a prognostic factor and potential
targets, we next evaluated the expression of CTGF and Ki-67 using
paraffin-embedded sections. Mesothelial cells, which are
nontumorous, did not express CTGF (Fig. S3), whereas obvious CTGF expression
was observed in both mesothelioma cells and CAFs (Figs. 2A-F and S2). Biphasic and sarcomatoid
mesotheliomas were excluded after the IHC staining results were
examined, as described above. Heterogeneity in CTGF expression was
observed in both mesothelioma cells and CAFs. We therefore adopted
a semiquantitative scoring system (CTGF score; see Materials and
methods) to quantify the expression of CTGF in each tumor sample
(Fig. 3A and B) and compared these
scores with the numbers of Ki-67-positive cells (Ki-67 index). The
CTGF score for CAFs but not that of mesothelioma cells was
correlated with the Ki-67 index for mesothelioma cells (Fig. 3C and D). The CTGF score for CAFs was
also correlated with the αSMA area index, while that for
mesothelioma cells was not (Fig. 3E and
F). No significant correlations were found between CTGF
expression in mesothelioma cells and patient prognosis (Fig. 3G). However, CTGF expression in CAFs
correlated with poor prognosis (Fig.
3H). Notably, the clinicopathological features (pathological
invasion, lymph node metastasis, and stage) and sensitivities to
neoadjuvant chemotherapy of the examined mesothelioma cases did not
correlate with CTGF expression in either mesothelioma cells or CAFs
(Tables III and IV), suggesting that CTGF in CAFs could be
used as a marker that specifically predicts patient prognosis.
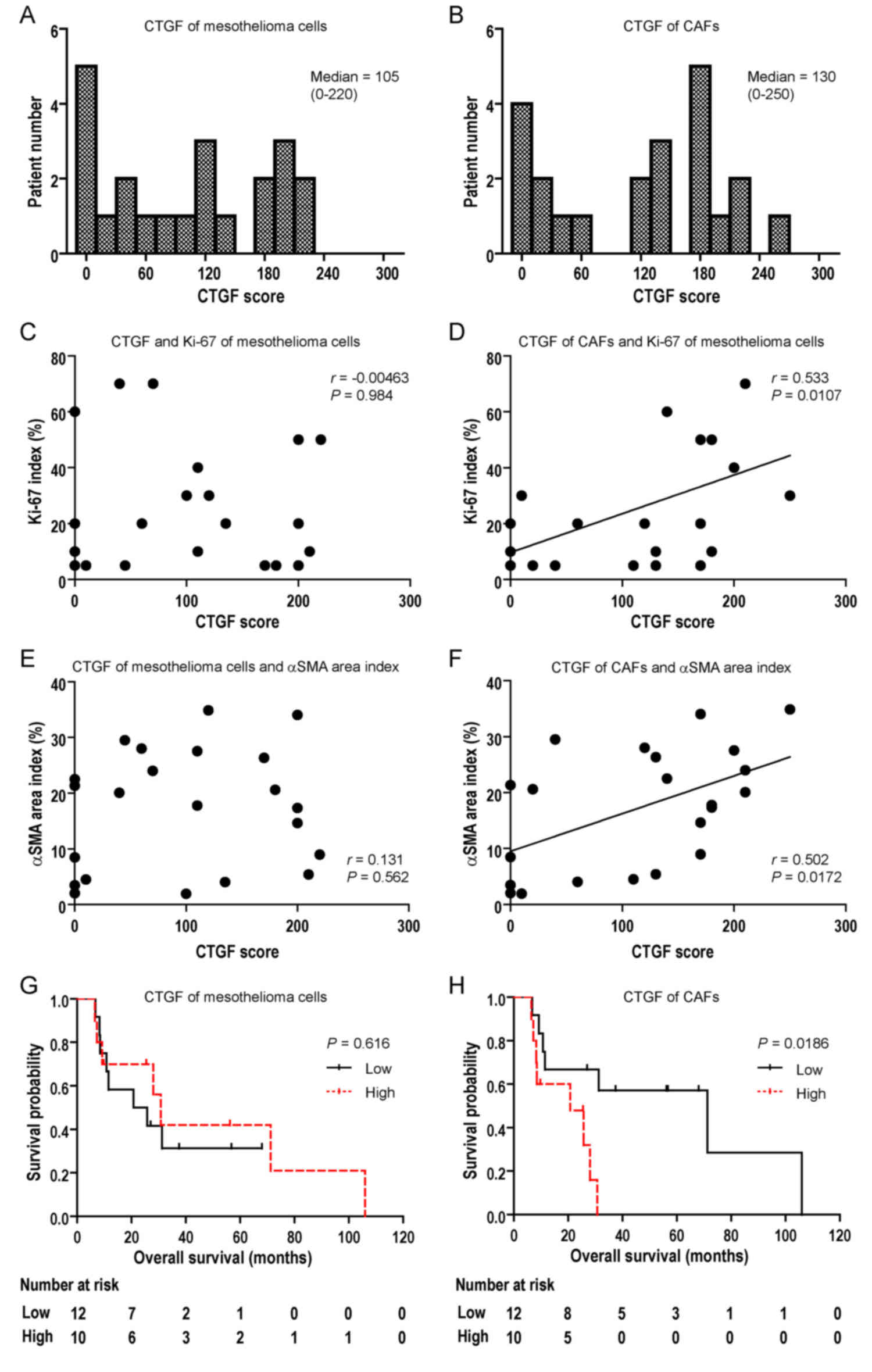 | Figure 3.CTGF expression in CAFs correlates
with mesothelioma patient prognosis. (A and B) Analysis of
immunohistochemical staining of CTGF. The H-score of CTGF (CTGF
score) for all cases is plotted as a histogram. (C) CTGF expression
in mesothelioma cells and the Ki-67 index, indicating no
significant differences. (D) CTGF expression in CAFs and the Ki-67
index, indicating a positive correlation (r=0.533, P=0.0107;
Spearman's correlation test). (E) CTGF expression in mesothelioma
cells and the αSMA area index, indicating no significant
differences. (F) CTGF expression in CAFs and the αSMA area index,
indicating a positive correlation (r=0.502, P=0.0172; Spearman's
correlation test). (G) CTGF expression in mesothelioma cells and
patient prognosis based on Kaplan-Meier survival curves. CTGF
scores were modified by the AE1/AE3 area index values. There were
no significant differences in prognosis based on modified CTGF
scores (low, <10; high, ≥10). (H) CTGF expression in CAFs and
patient prognosis based on Kaplan-Meier survival curves. CTGF
scores were modified by the αSMA area index values. There was a
significant difference (P=0.0186) in prognosis based on modified
CTGF score (low, <30; high, ≥30). αSMA, α-smooth muscle actin;
CAFs, cancer-associated fibroblasts; CTGF, connective tissue growth
factor. |
| Table III.CTGF in mesothelioma cells and
clinicopathological features of the mesothelioma cases. |
Table III.
CTGF in mesothelioma cells and
clinicopathological features of the mesothelioma cases.
|
Characteristics | Low | High | P-value |
|---|
| Age (years) |
|
| 0.670 |
|
<65 | 7 | 4 |
|
|
≥65 | 5 | 6 |
|
| Sex |
|
| 0.571 |
|
Male | 11 | 8 |
|
|
Female | 1 | 2 |
|
| Pathological
invasion |
|
| 0.675 |
| pT1 or
pT2 | 5 | 3 |
|
| pT3 or
pT4 | 7 | 7 |
|
| Lymph node
metastasis |
|
| 0.691 |
|
pN0 | 6 | 6 |
|
| pN1 or
pN2 | 6 | 4 |
|
| Stage |
|
| >0.999 |
| I or
II | 3 | 2 |
|
| III or
IV | 9 | 8 |
|
| Neoadjuvant
chemotherapy |
|
| >0.999 |
|
Absent | 3 | 3 |
|
|
Present | 9 | 7 |
|
|
Chemosensitivity |
|
| 0.308 |
| Grade 0
or 1a | 5 | 6 |
|
| Grade
1b or 2 | 4 | 1 |
|
| Table IV.CTGF in CAFs and clinicopathological
features of the mesothelioma cases. |
Table IV.
CTGF in CAFs and clinicopathological
features of the mesothelioma cases.
|
Characteristics | Low | High | P-value |
|---|
| Age (years) |
|
| 0.198 |
|
<65 | 8 | 3 |
|
|
≥65 | 4 | 7 |
|
| Sex |
|
| >0.999 |
|
Male | 10 | 9 |
|
|
Female | 2 | 1 |
|
| Pathological
invasion |
|
| 0.675 |
| pT1 or
pT2 | 5 | 3 |
|
| pT3 or
pT4 | 7 | 7 |
|
| Lymph node
metastasis |
|
| 0.691 |
|
pN0 | 6 | 6 |
|
| pN1 or
pN2 | 6 | 4 |
|
| Stage |
|
| >0.999 |
| I or
II | 3 | 2 |
|
| III or
IV | 9 | 8 |
|
| Neoadjuvant
chemotherapy |
|
| 0.646 |
|
Absent | 4 | 2 |
|
|
Present | 8 | 8 |
|
|
Chemosensitivity |
|
| >0.999 |
| Grade 0
or 1a | 6 | 5 |
|
| Grade
1b or 2 | 2 | 3 |
|
Meflin as a potential marker for
mesothelioma patient prognosis
We next investigated Meflin expression by RNA ISH
using paraffin-embedded sections. Mesothelial cells, which are
nontumorous, did not express Meflin (Fig. S2), while CAFs expressed Meflin
(Fig. 4A and B). More
Meflin+ CAFs were observed in the αSMA-negative area
than in the αSMA-positive area. Meflin expression did not correlate
with the clinicopathological features (Table V). Additionally, no significant
differences were found in patient prognosis according to Meflin
expression (Fig. 4C).
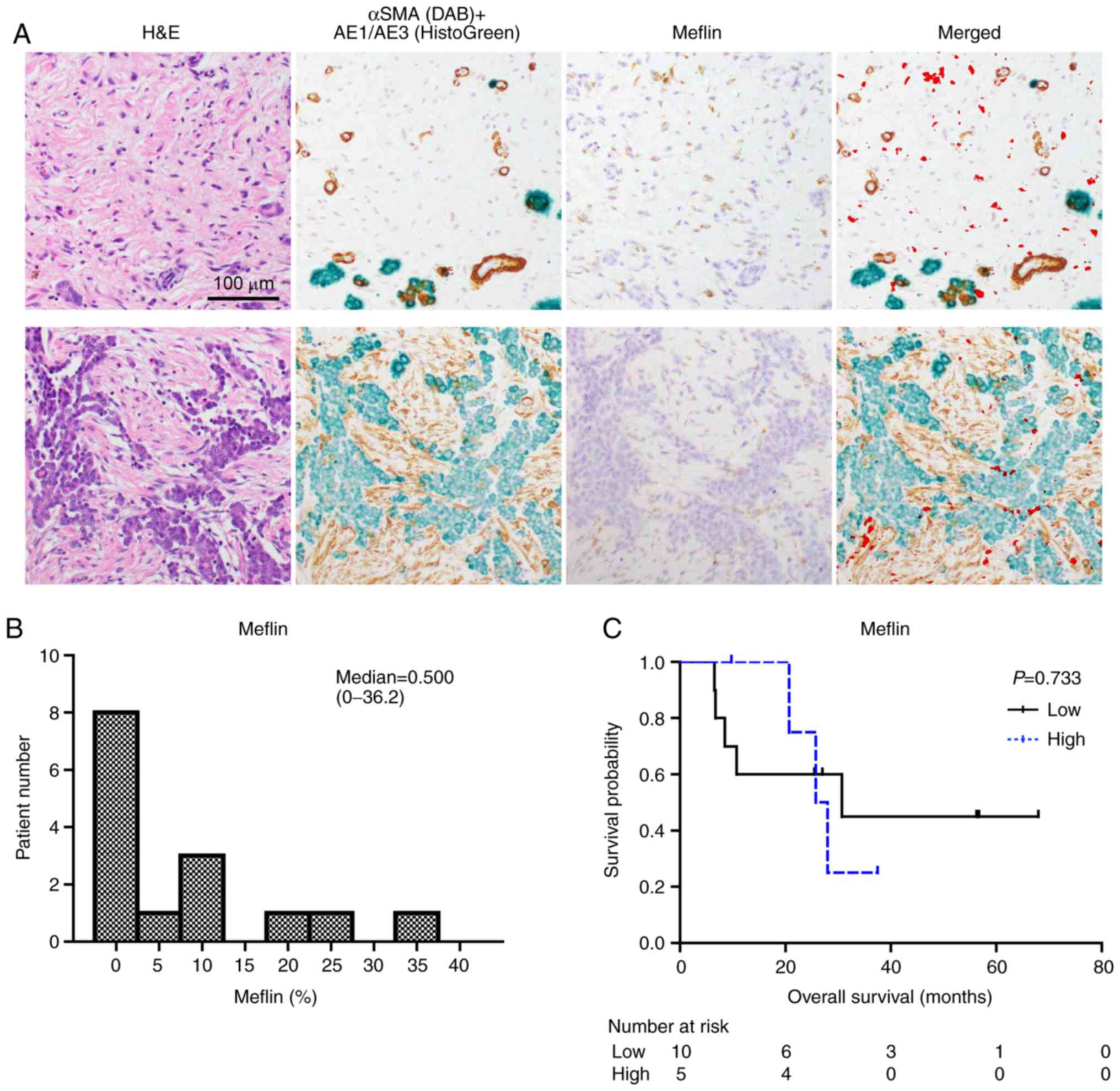 | Figure 4.Meflin expression in mesothelioma.
(A) RNA ISH of Meflin. DAB solution was used to stain αSMA, and
HistoGreen was used to stain AE1/AE3. Mesothelioma cells were
positive for AE1/AE3. CAFs and vessels were positive for αSMA. More
Meflin-positive (Meflin+) CAFs were observed in the
αSMA-negative area (top), which is the invasive front of
mesothelioma. Less Meflin+ CAFs were observed in the
αSMA-high area (bottom), which is the proximal side of
mesothelioma. The merged images of αSMA + AE1/AE3 and Meflin were
obtained using ImageJ software. Meflin-positive area is indicated
by red color in the merged images. All images are shown at the same
magnification. (B) Analysis of RNA ISH data for Meflin. The
proportions of the Meflin+ CAFs for all cases are
plotted as a histogram. (C) Meflin expression in CAFs and patient
prognosis based on Kaplan-Meier survival curves. There was no
significant difference in prognosis based on the proportions of the
Meflin+ CAFs (low, <10%; high, ≥10%).
Gehan-Breslow-Wilcoxon test was used for analysis. αSMA, α-smooth
muscle actin; CAFs, cancer-associated fibroblasts; H&E,
hematoxylin and eosin; ISH, in situ hybridization; Meflin,
mesenchymal stromal cell- and fibroblast-expressing Linx
paralogue. |
| Table V.Meflin and clinicopathological
features of the mesothelioma cases. |
Table V.
Meflin and clinicopathological
features of the mesothelioma cases.
|
Characteristics | Low | High | P-value |
|---|
| Age (years) |
|
| >0.999 |
|
<65 | 4 | 2 |
|
|
≥65 | 6 | 3 |
|
| Sex |
|
| 0.333 |
|
Male | 10 | 4 |
|
|
Female | 0 | 1 |
|
| Pathological
invasion |
|
| >0.999 |
| pT1 or
pT2 | 4 | 2 |
|
| pT3 or
pT4 | 6 | 3 |
|
| Lymph node
metastasis |
|
| 0.580 |
|
pN0 | 5 | 4 |
|
| pN1 or
pN2 | 5 | 1 |
|
| Stage |
|
| >0.999 |
| I or
II | 3 | 1 |
|
| III or
IV | 7 | 4 |
|
| Neoadjuvant
chemotherapy |
|
| 0.600 |
|
Absent | 4 | 1 |
|
|
Present | 6 | 4 |
|
|
Chemosensitivity |
|
| >0.999 |
| Grade 0
or 1a | 4 | 3 |
|
| Grade
1b or 2 | 2 | 1 |
|
Discussion
In the present study, we demonstrated that not only
mesothelioma cells but also cancer-associated fibroblasts (CAFs) in
mesothelioma express connective tissue growth factor (CTGF). CTGF
expression in CAFs was found to be correlated with patient
prognosis although CTGF expression in mesothelioma cells did not.
The CTGF score for mesothelioma cells did not correlate with the
Ki-67 index, but that for CAFs did. In addition, CTGF expression
did not correlate with tumor stage. If a marker correlates with
poor prognosis and tumor stage, it is possible that the correlation
is driven by tumor stage. In other words, the marker is highly
expressed in advanced stage tumors, which results in a correlation
of marker expression with poor prognosis. In the present study,
CTGF expression was found to be correlated with poor prognosis
after surgery irrespective of the tumor stage diagnosed at surgery.
Therefore, CTGF-positive (CTGF+) CAFs are directly
correlated with tumor malignancy/progression and CTGF may be a
molecular target for this disease.
Using tissue or serum samples, previous studies have
revealed that sarcomatoid mesothelioma expresses higher levels of
CTGF than the epithelioid subtype (13,40).
In another study, however, all human mesothelioma cell lines
expressed CTGF irrespective of histological subtype (15). This apparent inconsistency can be
explained by the results of the present study, that is, based on
CTGF expression by CAFs in vivo. Cells of sarcomatoid
mesothelioma are commonly spindle-shaped and accompanied by
proliferating nonneoplastic CAFs, making it difficult to
distinguish between these two cell types. Moreover, CTGF-specific
monoclonal antibody (FG-3019, pamrevlumab) was reported to exhibit
little effect on cancer cell proliferation in conventional
2-dimensional cell culture in vitro, whereas it strongly
inhibited cancer growth in vivo (15,41–43).
These results can also be due to the existence of CTGF+
CAFs.
In the present study, the αSMA area index was found
to be correlated with prognosis, as shown previously (16–20,44–47).
Although fibrosis in mesothelioma is distinctive from that in other
tumors, it is suggested that αSMA+ fibroblasts correlate
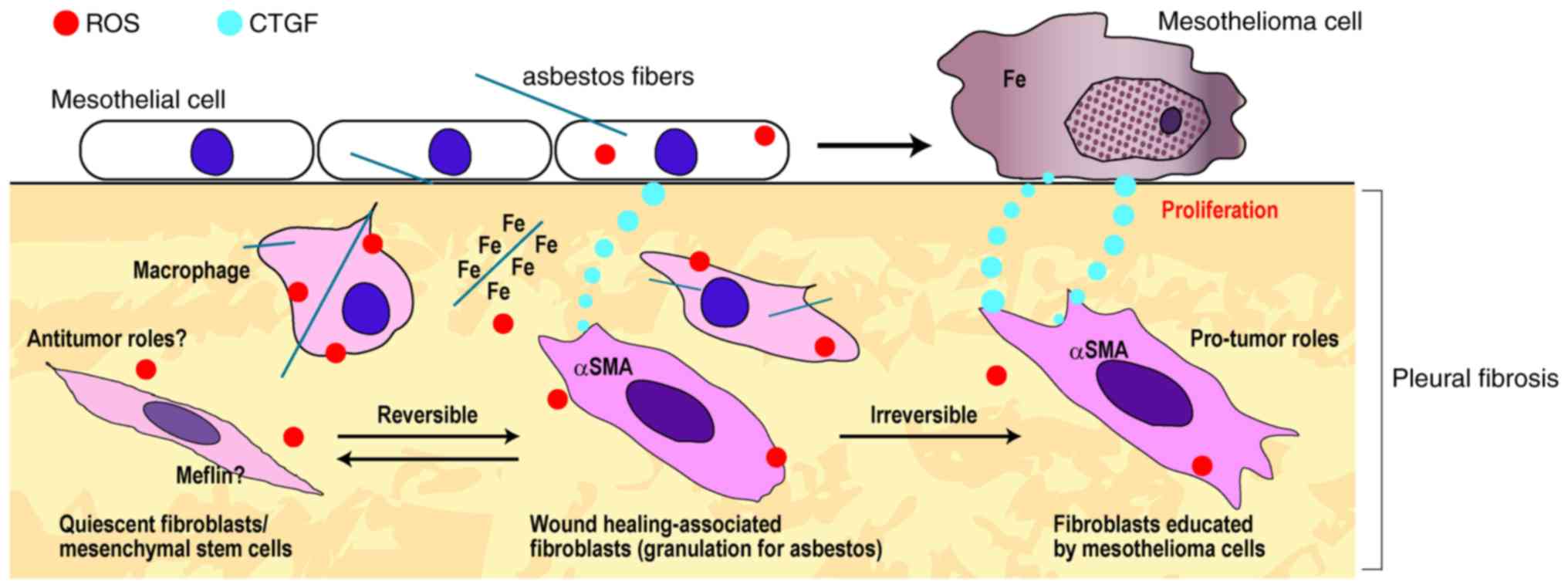
with mesothelioma growth. Inhaled asbestos can first result in
benign pleural fibrosis and then in mesothelioma (1,2,11).
Thus, mesothelioma tissues may exhibit substantial fibrosis from
the precancerous lesion/early mesothelioma stage in situ,
although tumor cells in other tumors involve fibroblasts and form
stroma only when they invade. In addition, reactive oxygen species
(ROS), playing a key molecular mechanism in mesothelial
carcinogenesis (4–8), can activate quiescent fibroblasts to
form myofibroblasts (18).
Therefore, not all αSMA+ fibroblasts in mesotheliomas
may be CAFs that are under the command of mesothelioma cells, as
some of these cells may be wound healing-associated (related to
granulation for asbestos) fibroblasts (Fig. 5). These myofibroblasts may also
express CTGF, because we previously confirmed that normal
fibroblasts can also express CTGF in vitro (15). These cells can contribute to
carcinogenesis by secreting CTGF and cytokines.
For this study, we used immunohistochemistry (IHC)
to demonstrate the roles of CAFs in mesothelioma progression as IHC
rarely decreases the signal compared to immunofluorescence (IF).
IHC made it possible to evaluate all of the specimens. In contrast,
IF of αSMA/CTGF may be useful for studying the differentiation of
CAFs from mesenchymal stem cells and for classifying CAFs
(αSMA/CTGF−, αSMA+/CTGF−,
αSMA−/CTGF+, and
αSMA+/CTGF+). We will perform such studies
and develop the IF of αSMA/CTGF in the future.
A limitation in this study is that the eventual
number of cases was not large. In our hospital, surgical cases of
mesothelioma are rare because of the rareness of the disease and
because the majority of cases were at the advanced stage at
diagnosis. In the stroma, Meflin expression appeared positive where
αSMA expression was negative in some lesions of the mesothelioma
tissue samples. The present study did not elucidate whether Meflin
correlates with patient survival. We were able to collect samples
from only 15 patients as RNA ISH needs to be performed on tissue
samples within five years of sample collection. CTGF expression did
not correlated with sensitivities to neoadjuvant chemotherapy. This
may be also because the number of cases is small for analysis. We
will gather more samples to examine the expression of CAF markers
(αSMA, CTGF, and Meflin) and the correlations of CAFs and
chemotherapy in the future.
In conclusion, CTGF+ CAFs are important
for mesothelioma growth and correlate with patient prognosis. Thus,
these cells may be a potential target for drugs. Our previous study
demonstrated that FG-3019 was effective for mesothelioma in a
murine orthotopic implantation model, and the results of the
present study suggest that FG-3019 targets CTGF+ CAFs.
Thus, whether FG-3019 has therapeutic effects in human mesothelioma
patients warrants further investigation.
Supplementary Material
Supporting Data
Acknowledgements
We thank Ms Tomomi Aoyama, Ms Naomi Tagami, and Dr
Hideki Tsubouchi (Nagoya University) for technical assistance. YO
was a recipient of the Takeda Science Foundation Fellowship (April
2014-March 2018).
Funding
The present study was supported in part by in part,
from JST CREST (grant no. JPMJCR19H4) and JSPS Kakenhi (grant nos.
JP17H04064, JP19H05462 and JP20H05502) to ST and by a Meidai
Ishikai Funding 2016 to YO.
Availability of data and materials
Data and materials are available upon request to the
corresponding author.
Authors' contributions
YO and ST designed the experiments. YO performed the
experiments and data analysis, wrote the main manuscript text, and
prepared the figures. AE, YT, KS, TI, HK, YMiz, YMiy, AH, SM, JS,
KY, FI, YMo, NM, TF, KK and KY provided administrative, technical,
and material support. All authors read and approved the manuscript
and agree to be accountable for all aspects of the research in
ensuring that the accuracy or integrity of any part of the work are
appropriately investigated and resolved.
Ethics approval and consent to
participate
Human mesothelioma tissues were obtained with
informed patient consent at the time of surgery at Nagoya
University Hospital (Nagoya, Japan). This study was carried out in
accordance with the Helsinki Declaration for Human Research and
approved by the Ethics Committee of Nagoya University Graduate
School of Medicine (protocol no. 2017-0127).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
αSMA
|
α-smooth muscle actin
|
|
CAFs
|
cancer-associated fibroblasts
|
|
CTGF
|
connective tissue growth factor
|
|
DAB
|
3,3′-diaminobenzidine
|
|
H&E
|
hematoxylin and eosin
|
|
IHC
|
immunohistochemistry
|
|
ISH
|
in situ hybridization
|
|
Meflin
|
mesenchymal stromal cell- and
fibroblast-expressing Linx paralogue
|
|
ROS
|
reactive oxygen species
|
References
|
1
|
International Agency for Research on
Cancer, . WHO. Asbestos (chrysotile, amosite, crocidolite,
tremolite, actinolite, and anthophyllite). IARC Monographs on the
Evaluation of Carcinogenic Risks to Humans Volume 100C. A Review of
Human Carcinogens; Part C: Arsenic. Metals. (Fibres, and Dusts,
Lyon, France). 219–309. 2012.
|
|
2
|
Pavlisko EN and Sporn TA: Mesothelioma.
Pathology of asbestos-associated diseases. 3rd. Springer; Berlin:
pp. 81–140. 2014, View Article : Google Scholar
|
|
3
|
Rusch VW, Giroux D, Kennedy C, Ruffini E,
Cangir AK, Rice D, Pass H, Asamura H, Waller D, Edwards J, et al:
Initial analysis of the international association for the study of
lung cancer mesothelioma database. J Thorac Oncol. 7:1631–1639.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Donaldson K, Murphy FA, Duffin R and
Poland CA: Asbestos, carbon nanotubes and the pleural mesothelium:
A review of the hypothesis regarding the role of long fibre
retention in the parietal pleura, inflammation and mesothelioma.
Part Fibre Toxicol. 7:52010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nagai H and Toyokuni S: Biopersistent
fiber-induced inflammation and carcinogenesis: Lessons learned from
asbestos toward safety of fibrous nanomaterials. Arch Biochem
Biophys. 502:1–7. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chew SH and Toyokuni S: Malignant
mesothelioma as an oxidative stress-induced cancer: An update. Free
Radic Biol Med. 86:166–178. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nagai H and Toyokuni S: Differences and
similarities between carbon nanotubes and asbestos fibers during
mesothelial carcinogenesis: Shedding light on fiber entry
mechanism. Cancer Sci. 103:1378–1390. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Toyokuni S: Iron addiction with
ferroptosis-resistance in asbestos-induced mesothelial
carcinogenesis: Toward the era of mesothelioma prevention. Free
Radic Biol Med. 133:206–215. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Toyokuni S: Role of iron in
carcinogenesis: Cancer as a ferrotoxic disease. Cancer Sci.
100:9–16. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ohara Y, Chew SH, Shibata T, Okazaki Y,
Yamashita K and Toyokuni S: Phlebotomy as a preventive measure for
crocidolite-induced mesothelioma in male rats. Cancer Sci.
109:330–339. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jiang L, Chew SH, Nakamura K, Ohara Y,
Akatsuka S and Toyokuni S: Dual preventive benefits of iron
elimination by desferal in asbestos-induced mesothelial
carcinogenesis. Cancer Sci. 107:908–915. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chew SH, Okazaki Y, Akatsuka S, Wang S,
Jiang L, Ohara Y, Ito F, Saya H, Sekido Y and Toyokuni S:
Rheostatic CD44 isoform expression and its association with
oxidative stress in human malignant mesothelioma. Free Radic Biol
Med. 106:91–99. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jiang L, Yamashita Y, Chew SH, Akatsuka S,
Ukai S, Wang S, Nagai H, Okazaki Y, Takahashi T and Toyokuni S:
Connective tissue growth factor and β-catenin constitute an
autocrine loop for activation in rat sarcomatoid mesothelioma. J
Pathol. 233:402–414. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang S, Jiang L, Han Y, Chew SH, Ohara Y,
Akatsuka S, Weng L, Kawaguchi K, Fukui T, Sekido Y, et al:
Urokinase-type plasminogen activator receptor promotes
proliferation and invasion with reduced cisplatin sensitivity in
malignant mesothelioma. Oncotarget. 7:69565–69578. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ohara Y, Chew SH, Misawa N, Wang S, Somiya
D, Nakamura K, Kajiyama H, Kikkawa F, Tsuyuki Y, Jiang L, et al:
Connective tissue growth factor-specific monoclonal antibody
inhibits growth of malignant mesothelioma in an orthotopic mouse
model. Oncotarget. 9:18494–18509. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Orimo A and Weinberg RA: Stromal
fibroblasts in cancer: A novel tumor-promoting cell type. Cell
Cycle. 5:1597–1601. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kalluri R: The biology and function of
fibroblasts in cancer. Nat Rev Cancer. 16:582–598. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
LeBleu VS and Kalluri R: A peek into
cancer-associated fibroblasts: Origins, functions and translational
impact. Dis Model Mech. 11:dmm0294472018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Öhlund D, Elyada E and Tuveson D:
Fibroblast heterogeneity in the cancer wound. J Exp Med.
211:1503–1523. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rhim AD, Oberstein PE, Thomas DH, Mirek
ET, Palermo CF, Sastra SA, Dekleva EN, Saunders T, Becerra CP,
Tattersall IW, et al: Stromal elements act to restrain, rather than
support, pancreatic ductal adenocarcinoma. Cancer Cell. 25:735–747.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sherman MH, Yu RT, Engle DD, Ding N,
Atkins AR, Tiriac H, Collisson EA, Connor F, Van Dyke T, Kozlov S,
et al: Vitamin D receptor-mediated stromal reprogramming suppresses
pancreatitis and enhances pancreatic cancer therapy. Cell.
159:80–93. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Öhlund D, Handly-Santana A, Biffi G,
Elyada E, Almeida AS, Ponz-Sarvise M, Corbo V, Oni TE, Hearn SA,
Lee EJ, et al: Distinct populations of inflammatory fibroblasts and
myofibroblasts in pancreatic cancer. J Exp Med. 214:579–596. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Raghu G, Scholand MB, de Andrade J,
Lancaster L, Mageto Y, Goldin J, Brown KK, Flaherty KR, Wencel M,
Wanger J, et al: FG-3019 anti-connective tissue growth factor
monoclonal antibody: Results of an open-label clinical trial in
idiopathic pulmonary fibrosis. Eur Respir J. 47:1481–1491. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Richeldi L, Fernández Pérez ER, Costabel
U, Albera C, Lederer DJ, Flaherty KR, Ettinger N, Perez R, Scholand
MB, Goldin J, et al: Pamrevlumab, an anti-connective tissue growth
factor therapy, for idiopathic pulmonary fibrosis (PRAISE): A phase
2, randomised, double-blind, placebo-controlled trial. Lancet
Respir Med. 8:25–33. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Picozzi VJ, Pipas JM, Koong AC, Giaccia
AJ, Bahary N, Krishnamurthi SS, Lopez CD, O'Dwyer P, Modelska K,
Carney M, et al: FG-3019, a human monoclonal antibody to connective
tissue growth factor, combined with chemotherapy in patients with
locally advanced or metastatic pancreatic ductal adenocarcinoma. J
Cancer Clin Trials. 2:12017.
|
|
27
|
Maeda K, Enomoto A, Hara A, Asai N,
Kobayashi T, Horinouchi A, Maruyama S, Ishikawa Y, Nishiyama T,
Kiyoi H, et al: Identification of Meflin as a potential marker for
mesenchymal stromal cells. Sci Rep. 6:222882016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hara A, Kobayashi H, Asai N, Saito S,
Higuchi T, Kato K, Okumura T, Bando YK, Takefuji M, Mizutani Y, et
al: Roles of the mesenchymal stromal/stem cell marker Meflin in
cardiac tissue repair and the development of diastolic dysfunction.
Circ Res. 125:414–430. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mizutani Y, Kobayashi H, Iida T, Asai N,
Masamune A, Hara A, Esaki N, Ushida K, Mii S, Shiraki Y, et al:
Meflin-positive cancer-associated fibroblasts inhibit pancreatic
carcinogenesis. Cancer Res. 79:5367–5381. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM Classification of Malignant Tumors (UICC), 7th edn. New
York, NY. Wiley–Liss. 2009.
|
|
31
|
Chew SH, Okazaki Y, Nagai H, Misawa N,
Akatsuka S, Yamashita K, Jiang L, Yamashita Y, Noguchi M, Hosoda K,
et al: Cancer-promoting role of adipocytes in asbestos-induced
mesothelial carcinogenesis through dysregulated adipocytokine
production. Carcinogenesis. 35:164–172. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kato T, Noma K, Ohara T, Kashima H,
Katsura Y, Sato H, Komoto S, Katsube R, Ninomiya T, Tazawa H, et
al: Cancer-associated fibroblasts affect intratumoral
CD8+ and FoxP3+ T cells via IL6 in the tumor
microenvironment. Clin Cancer Res. 24:4820–4833. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ruifrok AC and Johnston DA: Quantification
of histochemical staining by color deconvolution. Anal Quant Cytol
Histol. 23:291–299. 2001.PubMed/NCBI
|
|
34
|
Boyle TA, Masago K, Ellison KE, Yatabe Y
and Hirsch FR: ROS1 immunohistochemistry among major genotypes of
non-small-cell lung cancer. Clin Lung Cancer. 16:106–111. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Detre S, Saclani Jotti G and Dowsett M: A
‘quickscore’ method for immunohistochemical semiquantitation:
Validation for oestrogen receptor in breast carcinomas. J Clin
Pathol. 48:876–878. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Husain AN, Colby TV, Ordóñez NG, Allen TC,
Attanoos RL, Beasley MB, Butnor KJ, Chirieac LR, Churg AM, Dacic S,
et al: Guidelines for pathologic diagnosis of malignant
mesothelioma 2017 update of the consensus statement from the
international mesothelioma interest group. Arch Pathol Lab Med.
142:89–108. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Attanoos RL, Dojcinov SD, Webb R and Gibbs
AR: Anti-mesothelial markers in sarcomatoid mesothelioma and other
spindle cell neoplasms. Histopathology. 37:224–231. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Chirieac LR, Pinkus GS, Pinkus JL,
Godleski J, Sugarbaker DJ and Corson JM: The immunohistochemical
characterization of sarcomatoid malignant mesothelioma of the
pleura. Am J Cancer Res. 1:14–24. 2011.PubMed/NCBI
|
|
39
|
Churg A, Cagle P, Colby TV, Corson JM,
Gibbs AR, Hammar S, Ordonez N, Roggli VL, Tazelaar HD, Travis WD,
et al: The fake fat phenomenon in organizing pleuritis: A source of
confusion with desmoplastic malignant mesotheliomas. Am J Surg
Pathol. 35:1823–1829. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Fujii M, Toyoda T, Nakanishi H, Yatabe Y,
Sato A, Matsudaira Y, Ito H, Murakami H, Kondo Y, Kondo E, et al:
TGF-β synergizes with defects in the Hippo pathway to stimulate
human malignant mesothelioma growth. J Exp Med. 209:479–494. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Dornhöfer N, Spong S, Bennewith K, Salim
A, Klaus S, Kambham N, Wong C, Kaper F, Sutphin P, Nacamuli R, et
al: Connective tissue growth factor-specific monoclonal antibody
therapy inhibits pancreatic tumor growth and metastasis. Cancer
Res. 66:5816–5827. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Neesse A, Frese KK, Bapiro TE, Nakagawa T,
Sternlicht MD, Seeley TW, Pilarsky C, Jodrell DI, Spong SM and
Tuveson DA: CTGF antagonism with mAb FG-3019 enhances chemotherapy
response without increasing drug delivery in murine ductal pancreas
cancer. Proc Natl Acad Sci USA. 110:12325–12330. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Finger EC, Cheng CF, Williams TR, Rankin
EB, Bedogni B, Tachiki L, Spong S, Giaccia AJ and Powell MB: CTGF
is a therapeutic target for metastatic melanoma. Oncogene.
33:1093–1100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Sinn M, Denkert C, Striefler JK, Pelzer U,
Stieler JM, Bahra M, Lohneis P, Dörken B, Oettle H, Riess H and
Sinn BV: α-Smooth muscle actin expression and desmoplastic stromal
reaction in pancreatic cancer: Results from the CONKO-001 study. Br
J Cancer. 111:1917–1923. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Underwood TJ, Hayden AL, Derouet M, Garcia
E, Noble F, White MJ, Thirdborough S, Mead A, Clemons N, Mellone M,
et al: Cancer-associated fibroblasts predict poor outcome and
promote periostin-dependent invasion in oesophageal adenocarcinoma.
J Pathol. 235:466–477. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Valach J, Fík Z, Strnad H, Chovanec M,
Plzák J, Cada Z, Szabo P, Sáchová J, Hroudová M, Urbanová M, et al:
Smooth muscle actin-expressing stromal fibroblasts in head and neck
squamous cell carcinoma: Increased expression of galectin-1 and
induction of poor prognosis factors. Int J Cancer. 131:2499–2508.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Fujita H, Ohuchida K, Mizumoto K, Nakata
K, Yu J, Kayashima T, Cui L, Manabe T, Ohtsuka T and Tanaka M:
Alpha-smooth muscle actin expressing stroma promotes an aggressive
tumor biology in pancreatic ductal adenocarcinoma. Pancreas.
39:1254–1262. 2010. View Article : Google Scholar : PubMed/NCBI
|