Introduction
Ovarian cancer (OC) is the most common malignancy of
the female reproductive system and the fifth leading cause of
cancer-associated death in women in the USA (1). In 2020, ~313,956 new cases of OC were
diagnosed and ~207,252 OC-associated deaths occurred worldwide
(2). Despite therapeutic advances,
the responses of patients with advanced OC remain unsatisfactory,
with 70% of patients experiencing relapse after treatment.
Consequently, the survival rate is extremely low, making OC one of
the primary causes of cancer-associated mortality in women
(3). In 2020, the number of
OC-associated deaths in the USA reached 13,438, accounting for 4.2%
of all cancer-related deaths (1).
Histopathologically, 90% of all OC develops from
epithelial cells, and the main subtypes are serous and mucinous
(4). The World Health Organization
(WHO) previously published a classification standard for tumors of
the female genital organs, which categorizes epithelial OC (EOC)
into two types based on the genetic lineage (5). Type I EOC includes low-grade serous
carcinoma, low-grade endometrioid carcinoma, clear cell carcinoma
and mucinous carcinoma. Type I EOCs develop from benign or
borderline ovarian lesions and are characterized by slow growth,
being typically confined to the ovaries and exhibiting large
unilateral cystic tumors (6,7). The
genetic mutations in type I EOCs are more stable, such as KRAS,
BRAF, CTNNB1, PTEN, PIK3CA, ARID1A, and PPP2R1A and ERBB2
mutations, while the TP53 mutation is rare (8). Surgery is an effective treatment for
early stage type I EOCs, but advanced cases are often unresponsive
to cytotoxic chemotherapy, with targeted drugs, such as BRAF
inhibitors, showing some efficacy. Type II EOC includes high-grade
serous carcinoma, high-grade endometrioid carcinoma, carcinosarcoma
and undifferentiated carcinoma (9).
Most patients are diagnosed in the first instance with
advanced-stage cancer, exhibiting invasion of extra-ovarian
tissues, although type II EOCs usually present as small lesions
involving both ovaries. Furthermore, the tumor volume at the site
of metastasis is large, accompanied by ascites and other malignant
tumor signs. TP53 mutations and CCNE1 amplification are present in
>80% of patients with type II EOC, while other mutations are
rare (10). Although traditional
platinum-based chemotherapy is effective for the majority of type
II EOCs, the overall survival (OS) rate of patients remains poor
due to a high propensity for relapse (11). In summary, the prognosis of patients
with type I EOCs is generally more favorable than those with type
II EOCs (12).
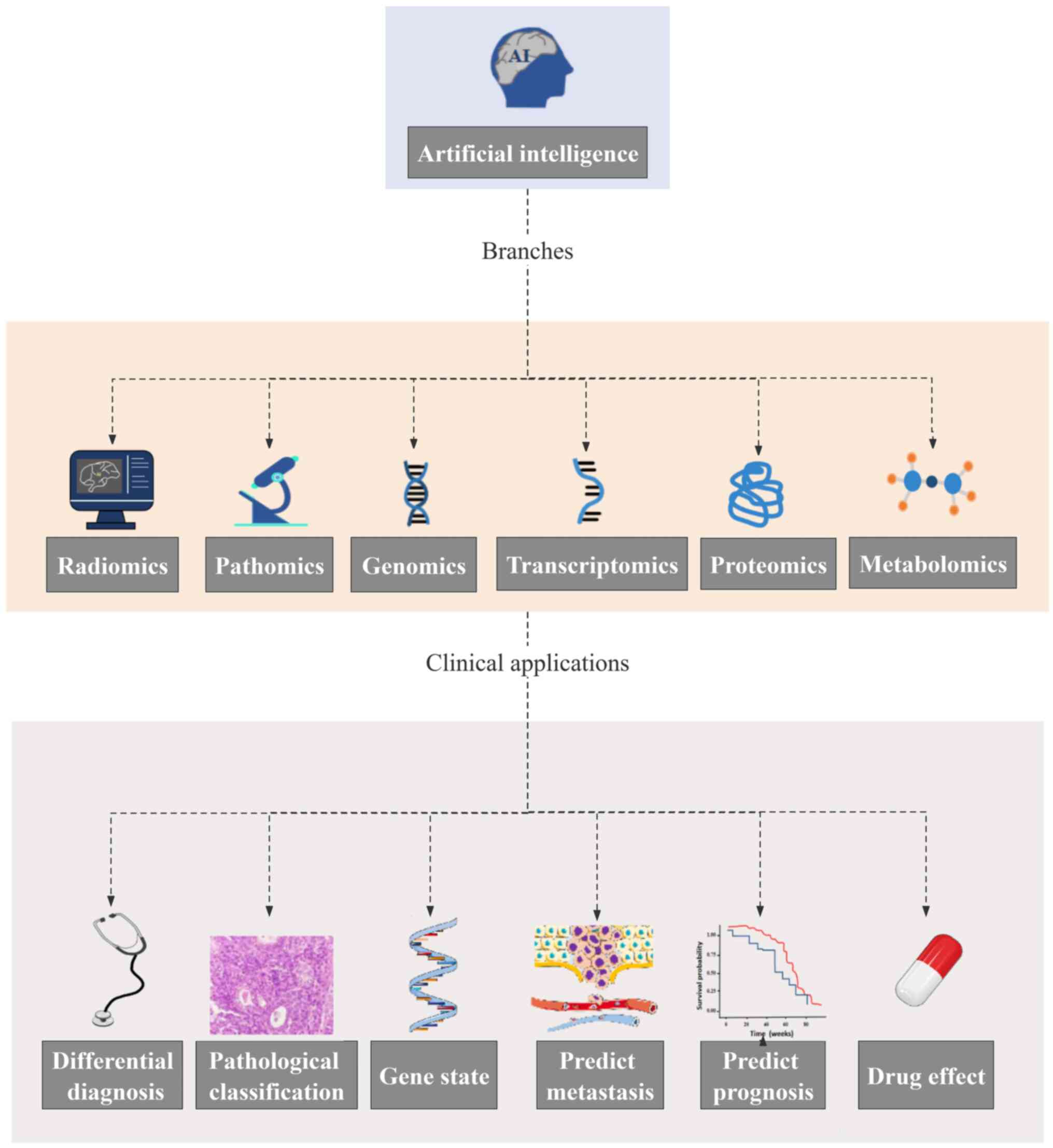
Artificial intelligence (AI), a branch of computer
science, refers to the ability of computer systems to learn from
input data. AI is playing an important role in areas of medical
research, including imaging, pathomics, genomics, transcriptomics,
proteomics and metabolomics. In recent years, AI-based multi-omics
research has been widely conducted with a focus on OC diagnosis,
benign and malignant differentiation, and the prediction of
pathological classification, drug efficacy and prognosis.
Researchers have studied and reviewed the clinical application of
AI in OC. Shrestha et al (13) reviewed AI methods, imaging methods
and clinical parameters in gynecological tumors, such as
endometrial cancer, cervical cancer and OC. However, this previous
study is limited to only discussing the content based on medical
images, and there is no elaboration on other omics-based
technologies, such as pathomics, genomics, transcriptomics and
several other omics. Similarly, Mikdadi et al (14) reviewed the use of AI in the
diagnosis and prognosis of OC and pancreatic cancer; however, the
study did not provide detailed research progress of AI in various
other omics-based approaches (14).
In addition, Shrestha et al (13) reviewed the application of AI for the
processing of medical images, clinical information and biological
information of common gynecological tumors. Breen et al
(15) reviewed studies on the use
of AI for the analysis of histopathological images in OC, and
evaluated the role of various AI models in the diagnosis and
prognosis of the disease. Notably, most of the aforementioned
studies are limited to evaluating the application value of uniomics
in AI. In the present study, a comprehensive review of the workflow
of AI and its applications in imaging, pathomics, genomics,
transcriptomics, proteomics and metabolomics is provided.
Radiomics
Radiomics is a non-invasive approach to extract
high-throughput imaging features from the medical images of
techniques such as computed tomography (CT), magnetic resonance
imaging (MRI) and ultrasound, and was first proposed by Lambin
et al in 2012 (16). Medical
images contain high-throughput digital information related to tumor
pathophysiology (17). Moreover,
radiomics can be used to extract relevant features from images, and
combine and supplement the findings with clinical information,
pathophysiology and molecular biological information, so as to
improve clinical diagnosis, predict the tumor stage and genotype,
and assess the prognosis (18,19).
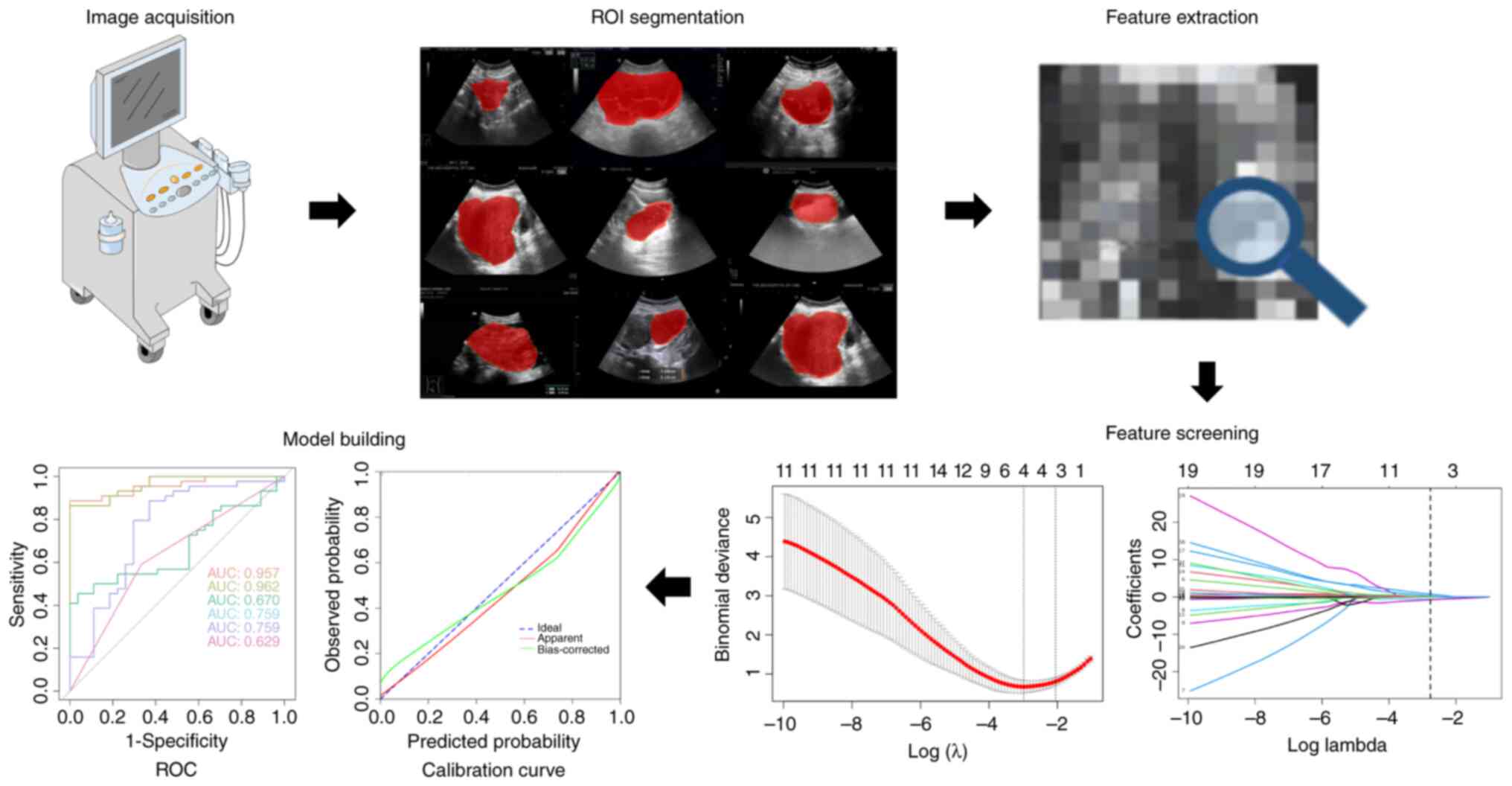
The major steps of radiomics include medical image acquisition,
image segmentation, feature extraction, feature screening and model
building (Fig. 1). Radiomics has
been widely used in the research of various tumors, including
thyroid (20), breast (21), liver (22) and prostate (23) cancer, and OC (24).
Image acquisition
CT, MRI, positron emission tomography (PET) and
ultrasound are the most common image acquisition methods (25). Images obtained by the same machine
equipment, scanning method and scanning layer thickness need not
undergo post-processing during feature extraction. However, images
obtained using different equipment and acquisition conditions
require pre-processing before feature extraction. The
pre-processing process includes resampling, standardization and
high-pass filtering, to obtain a uniform layer thickness and matrix
size for feature extraction. Due to the limitations of imaging
conditions imposed by radiomics, there are few prospective studies
(26). Most research has been
conducted as retrospective studies (20–24),
thus the medical images acquired come from hospital image storage
systems or online databases (27).
Image segmentation
After obtaining medical images, a region of interest
(ROI) is typically delineated, which involves automatic
segmentation, manual segmentation and semi-automatic segmentation.
Automatic segmentation is fast in delineating lesions, but poor in
identifying them. In addition, the edge of tumors on most medical
images is vague, and the influence of surrounding metastases and
accompanying symptoms, such as inflammation, on the image easily
interferes with the contours created by semi-automatic and
automatic segmentation. Manual segmentation, on the other hand, is
subjective and slow, as it depends on the identification of the
lesions and drawing of contours by clinicians. Semi-automatic
segmentation, based on automatic segmentation, allows clinicians to
‘proofread’ the delineated edges manually, which can improve the
efficiency and accuracy of the delineation (28). Currently, ordinary ROI mapping
software includes MIM (www.mimsoftware.com), ITK-SNAP (www.itksnap.com), 3DSlicer (www.slicer.org) and ImageJ (National Institutes of
Health) software.
Feature extraction
Radiomics features include the morphological,
first-order, second-order and higher-order features of the tumor
itself (29). Morphological
features include the tumor shape, size, vascular distribution and
its relationship with surrounding tissue, amongst other features.
However, each feature alone provides general characteristics of the
tumor instead of tumor heterogeneity. First-order features are also
recognized as intensity features, which are related to the
distribution of gray-level intensities in the ROI. The histogram
represents the number of pixels with a certain gray level in the
image, reflecting the frequency of each gray level in the image.
Information such as maximum, minimum, mean, mean absolute
deviation, median, skewness, standard deviation, consistency,
variance, energy and entropy can be obtained from the intensity
histogram. The second-order features include the gray co-occurrence
matrix and the gray run length matrix, which can estimate the
spatial distribution relationship of the image gray value. The
higher-order features include the neighborhood gray difference
matrix and gray region size matrix. The gray difference matrix of
the neighborhood can evaluate the pixel heterogeneity between the
ROI and adjacent regions, while the gray region size matrix can
evaluate the characteristics of homogeneous regions (30).
Feature screening
In the process of feature extraction, several
features will be identified, which may lead to overfitting when the
data set is smaller than the feature set (31). To avoid this overfitting of the
model, several features must be selected. Feature screening is
usually achieved using AI or statistical methods, and commonly used
methods include maximum correlation minimum redundancy, principal
component analysis and least absolute shrinkage and selection
operator (LASSO) regression, amongst other approaches (32).
Model building
The final step in radiomics is the establishment of
the model, which can combine patient clinical data, susceptibility
factors and biomarkers with radiomics to create a more precise
model. For example, a nomogram is often used in the modeling of
imaging omics (33). The
establishment of these models has improved the ability of
clinicians to diagnose and differentiate diseases. Some models can
also predict pathological types and patient outcomes, which
contributes to the implementation of personalized medicine and
modern medicine. Several studies have combined imaging with
genomics, transcriptomics, proteomics and metabolomics to build
diagnostic models, gene expression models and prognostic models of
diseases (34–36).
AI in the radiomics of OC
Traditional imaging diagnosis relies on a
clinician's subjective judgment of the visual information (37). However, AI can standardize and
simplify the process by extracting the available information from
the images by mimicking the cognitive behaviors associated with the
human brain (38). Therefore, AI
can be applied to the process of feature screening and model
building in radiomics. The significant differences in AI
diagnostics using imaging depend on who created the AI model
(39). AI includes machine learning
(ML), significant data management and information mining, image
processing and pattern recognition. ML is the approach and core of
medical AI, including supervised learning, unsupervised learning
and reinforcement learning (40,41).
Supervised learning refers to the application of known cohorts as
known information of learning, so as to build a classification and
prediction model for unknown cohorts (42). However, the data results are not
necessary for the construction of the unsupervised learning model,
and the data can be summarized and classified (43). Reinforcement learning is a
computational method to understand and automatically process
goal-oriented learning and decision-making problems, and there are
several advantages, such as direct interaction with the environment
and autonomous learning without the need for emulated supervisory
signals for modeling (44).
Notably, ML is an essential branch of AI, and the major procedures
include data collection and processing, model training and
optimization, and model evaluation, amongst others (45). ML can establish models by converting
medical images into features or labels and subsequently performing
a mapping from features to labels using algorithms. ML primarily
includes logistic regression, artificial neural networks (ANNs),
support vector machines and deep learning convolutional neural
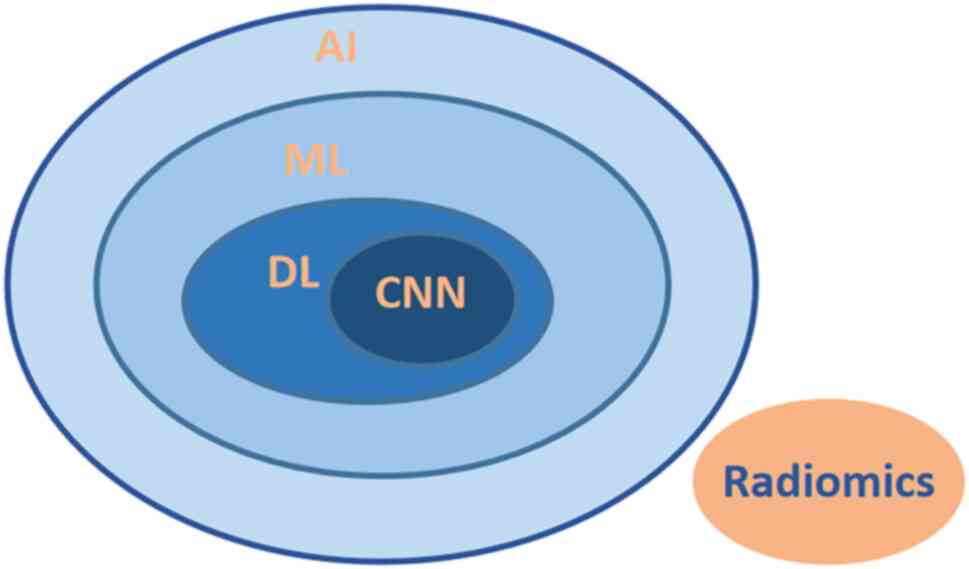
networks (DCNNs) (46). Deep
learning (DL) is a subset of ML, which can use multiple ANNs to
solve complex problems based on the structure of brain neurons.
Neural networks can link dependent and independent variables
together without prior knowledge to detect patterns and nonlinear
interactions in complex data (47).
CNNs, a subset of AI and DL, are a special type of computational
model the principle of which is to imitate neurons and synapses in
the human brain (Fig. 2) (47). A neural network with more hidden
layers is defined as a deep neural network. DL can solve various
classification and prediction problems using deep neural networks;
it can also identify features from data automatically and avoiding
manual feature selection, which is an apparent advantage compared
with traditional ML (48).
Radiomics, ML and DL are not independent
individuals, but are intricately intertwined for the most part. The
modeling process in radiomics usually relies on DL (49). AI has been widely used in the
diagnosis of diseases, the differentiation of benign and malignant
tumors, and the prediction of therapeutic effects (50) (Fig.
3).
Identification of benign and malignant
tumors
The comprehensive evaluation of ovarian tumors, both
benign and malignant, requires a preliminary judgment by clinicians
based on symptoms, and laboratory and imaging examinations. At
present, the gold standard for determining benign and malignant
ovarian tumors is still pathological analysis of a puncture biopsy
or postoperative pathological examination. However, the methods are
invasive, and puncture biopsy carries a certain risk of needle path
metastasis (51). Therefore, a
number of studies have explored the application of radiomics in the
identification of benign and malignant tumors. For example, Wang
et al (52) retrospectively
collected CT images of patients with EOC from multiple centers to
establish a CT radiomics model that could distinguish high-grade
serous OC (HGSOC). The areas under the curve (AUCs) were 0.837 (95%
CI, 0.835-0.838) for the training cohort and 0.836 (95% CI,
0.833-0.840) for the testing cohort. The study confirmed that the
radiomics model is important for the individualized treatment and
prognostic evaluation of patients. Similarly, Li et al
(53) reported the effectiveness of
radiomics. This previous study established a radiomics model to
identify benign and malignant ovarian tumors based on 143 CT
images. The AUCs for both the training set (0.88) and the test set
(0.87) were high, which confirmed the discriminative ability of the
model. A nomogram combining clinical information and serum markers
was also created. Saida et al (54) reported that the established CNN
model of OC diagnosis based on MRI also showed a good diagnostic
effect. Moreover, it was demonstrated that the differential model
based on radiomics had a higher average diagnostic efficiency than
the radiologist (internal data set: 88.8 vs. 85.7%; external
validation data set: 86.9 vs. 81.1%), and the combined use of the
model could improve the efficiency of the radiologist. The accuracy
[87.6% (95% CI, 85.0-90.2) vs. 78.3% (95% CI, 72.1-84.5);
P<0.0001] and sensitivity [82.7% (95% CI, 78.5-86.9) vs. 70.4%
(95% CI, 59.1-81.7); P<0.0001] of DCNN-assisted diagnosis were
higher than the values for the radiologists alone (55). Wang et al (56) also explored the MRI of 201 patients
with borderline ovarian tumors and 99 patients with EOC, and
established a differential diagnosis model based on DL. The results
revealed that the accuracy of the AI model was higher than that of
the radiologists. A recent study showed that the models based on DL
had an AUC of 0.93 (95% CI, 0.85-0.97) for differentiating
malignant from benign ovarian tumors, which was comparable with the
Ovarian-Adnexal Reporting and Data System (O-RADS) (57) (AUC, 0.92; 95% CI, 0.85-0.97; P=0.88)
and expert assessment (AUC, 0.97; 95% CI, 0.91-0.99; P=0.07)
(58). The models based on
DLdecision, DLfeature, O-RADS and expert assessment achieved
sensitivities of 92, 92, 92 and 96%, respectively, and
specificities of 80, 85, 89 and 87%, respectively, for malignancy.
Therefore, the models based on DL may distinguish malignant from
benign ovarian tumors with a diagnostic performance comparable to
expert subjective and Ovarian-Adnexal Reporting and Data System
assessment. In addition, the specificity and sensitivity of the
models established by different AI algorithms for the
identification of ovarian tumors are also different (58). Other researchers have also shown
that AI models based on ultrasonic images have high accuracy and
sensitivity for the identification of OC, and the differentiation
of benign and malignant tumors. Furthermore, the diagnostic
efficacy is similar to that of ultrasound experts (59,60).
Pathological classification
EOC is classified into type I and type II according
to the classification standard of female reproductive organ cancers
from the WHO in 2014 (61). Due to
the difference in treatment and prognosis between type I and type
II EOC, it is necessary to classify the pathological type after a
diagnosis of OC (5). In this
regard, Tang et al (62)
investigated ultrasonic images of patients with EOC (n=154), and
divided them into type I and type II EOC according to the
pathology. The seven features with the greatest differences were
screened out using LASSO regression ten-fold cross-validation. As a
result, an identifiable model was established with satisfactory
predictive efficiency, with AUCs of 0.817 and 0.731 for the
training and test sets, respectively. Furthermore, radiomics can be
utilized to evaluate tumor heterogeneity in addition to predicting
pathological types. Xu et al (63) analyzed the MRI results of patients
with EOC (n=146), and established a model and nomograms for
distinguishing EOC from borderline ovarian tumors and EOC subtypes
using logistic regression. The study mapped not only the solid
components of the tumor tissue, but also the overall region of the
tumor tissue, providing a more complete evaluation of the tumor
heterogeneity. Jian et al (64) conducted a multicenter retrospective
analysis of MRI results in patients with EOC (n=294) and
established a radiomics model that distinguished type I from type
II by extracting relevant radiomics features from axial sequences
of T2-weighted images with fat saturation (T2WIFS),
diffusion-weighted imaging (DWI), apparent diffusion coefficient
and contrast enhanced (CE)-T1WI. The model showed good diagnostic
performance in both internal and external validation cohorts, with
AUCs of 0.806 and 0.847, respectively. Additionally, an occlusion
experiment was conducted to locate the critical areas of the image
for model building and diagnosis. The results showed that the most
important area used to identify type I and type II EOCs was located
at the junction between solid and cystic components, and in the
area with a low density of solid components in T2WIFS. This
conclusion may provide a basis and guidance for puncture diagnosis
of tumors and pathological sampling.
Gene mutation state
Studies have demonstrated that ~50% of EOC cases
carry homologous recombination repair defects, which are primarily
caused by mutations in the breast cancer susceptibility gene
(BRCA). BRCA can participate in the repair of DNA double-strand
breaks during the process of homologous recombination repair, and
is a crucial tumor suppressor gene (65,66).
Patients with advanced OC accompanied by BRCA mutations are more
responsive to platinum-based chemotherapy drugs, exhibiting higher
objective response rates and survival rates (66–69).
The 5-year survival rate and progression-free survival (PFS) rates
of patients with BRCA mutation-positive OC are higher than those
without mutations (70). Moreover,
BRCA1/2 mutation-positive patients have also shown good reactivity
when treated with platinum-based agents in patients with a
recurrent case of OC (71).
Therefore, it is essential to make a definitive diagnosis of any
BRCA mutations before treatment in order to aid the clinical
planning and evaluation of a patient's prognosis. Current
guidelines from different scientific societies also recommend the
genetic testing of BRCA1/2 for newly diagnosed patients with a
non-mucinous EOC (72). Although
puncture sampling is commonly used to detect BRCA gene status in
patients, it is an invasive method that may cause cancer cell
metastasis along the puncture needle tract during the process.
Furthermore, the gene expression within tumors may have certain
heterogeneity (73), and the
puncture sampling method can only perform genetic identification on
some of the tissues, instead of evaluating the overall genetic
diversity of the entire tumor (74). Additionally, genetic testing is
costly and time-consuming (75).
Radiomics has emerged as a promising alternative to genetic testing
in recent years. A number of studies have applied radiomics to
assess the gene state of OC. Meier et al (73) retrospectively collected the CT
images from 88 patients with HGSOC, and extracted the texture
features. The results showed that the radiomics features were
significantly correlated with the prognosis of the patients, but
not with the status of BRCA mutations, which may be due to the
small number of patients assessed. In addition to BRCA, Ki-67 was
also significantly correlated with the recurrence and prognosis of
OC. Wang et al (76)
analyzed the PET/CT images of patients with HGSOC (n=161). The
radiomics features of the whole tumor area were extracted based on
a Habitat method and a model for predicting the Ki-67 status of OC
was established. The results verified that radiomics could predict
the expression of Ki-67 accurately and might be a novel marker to
replace Ki-67. Additionally, the Habitat model could stratify
prognosis more efficiently (P<0.05).
Metastasis
Advanced OC is typically accompanied by
intra-abdominal diffusion and distant metastasis at first
diagnosis. It has been shown that the 5-year survival rate of
patients with OC is only 20–45% (77). Therefore, it is essential to detect
metastases early, as this affects the treatment used and the
management from stage to stage. However, the positive rate for
detection of small metastases by conventional means remains poor
(78). A novel approach, radiomics,
has been shown to predict metastasis more accurately (79). Ai et al (80) explored the CT images of patients
with OC (n=101), and identified nine radiomic features for
screening from a total of 184. The results revealed that the
radiomics model and the comprehensive model combined with age and
cancer antigen 125 levels could be used to predict the metastatic
status. Similarly, MRI-based research has validated the role of
radiomics in predicting OC metastasis. Yu et al (81) established a nomogram for predicting
peritoneal metastasis based on radiomics characteristics and
clinical data from FS-T2WI, DWI and dynamic CE-MRI images of 86
patients with OC. The comprehensive nomogram (AUC, 0.902) combining
radiomics characteristics and clinicopathological risk factors
showed a better diagnostic effect than the clinical model (AUC,
0.858) and the radiomics model (AUC, 0.846). These findings suggest
that the radiomics model is a promising method for predicting OC
metastasis, particularly small metastases, and may thus be used to
improve the detection rate.
Postoperative residue and
prognosis
In total, >70% of patients with OC are diagnosed
at an advanced stage (82), and the
current standard treatment involves initial tumor cell reduction
and platinum-based chemotherapy. However, the effectiveness of
initial tumor cell reduction and patient response to chemotherapy
drugs vary due to individual differences (such as gene mutation
status and physiological status) and tumor heterogeneity.
Therefore, it is important to predict a patient's response before
and after treatment (83).
Radiomics has emerged as a promising tool for predicting the
postoperative tumor residual status of patients and the risk of
recurrence after receiving chemotherapy drugs, which will be
conducive to the selection of chemotherapeutic drugs,
chemotherapeutic methods and the formulation of individualized
follow-up periods (84). Lu et
al (85) applied ML to obtain
the radiomic prognostic vector (RPV) for 364 patients with EOC. It
was reported that RPV could be used to assess patient outcomes in
discovery datasets, which was well validated in validation datasets
and the Cancer Genome Atlas validation dataset. Meier et al
(73) extracted CT features from
pre-treatment images of 88 patients with HGSOC and found that these
features were relevant to patient PFS and OS time. A study by Hong
et al (86) also verified
the ability of a model to predict OS in patients with OC. CT images
of serous OC were selected from the cancer imaging archive as the
model training set, while images collected in the study hospital
were used as the validation set, and three radiomics features were
finally screened out. Furthermore, the nomogram, in combination
with clinical data, was established as a model to evaluate the OS
with serous OC, which will be helpful for the formulation of
treatment strategies and the prognostic evaluation of patients. Wei
et al (87) verified the
relationship between PFS and the radiomics characteristics of
advanced HGSOC through Kaplan-Meier survival analysis and a Cox
proportional risk model, and established a nomogram for predicting
the recurrence risk of HGSOC. Notably, not only did the model have
a good predictive effect, but other DL models based on MRI and CT
images did also (88,89). Compared with CT and MRI, ultrasound
is more convenient and economical. In recent years, ultrasonography
has been used to establish a prognostic model for OC. In one study,
111 patients with EOC were examined by transvaginal
ultrasonography, and the characteristics of ultrasonography were
extracted to establish a comprehensive PFS prediction model
combined with clinical variables (90). Additionally, AI can predict the
length of postoperative hospital stay for patients with HGSOC
(91), which may contribute to the
individualized treatment and management plans in clinical
practice.
Response to chemotherapy
Lei et al (92) included MRI (CE-T1WI and T2WI) of 93
patients with EOC who had received platinum-based chemotherapy (≥4
cycles), and established two different models based on the primary
tumor or the entire abdomen as areas of interest. Furthermore,
1,024 features were extracted using the pre-trained CNN model. The
results showed that the whole abdominal DL model based on MRI was
effective in predicting the sensitivity of patients with EOC to
platinum-based therapy (Table
I).
 | Table I.Overview of the studies on AI in
radiomics. |
Table I.
Overview of the studies on AI in
radiomics.
| A, Identification
of benign and malignant tumors |
|---|
|
|---|
| First author,
year | Disease | Number of
patients | Type of
imaging | AI model | Main result | Main
conclusion | (Refs.) |
|---|
| Wang et al,
2022 | EOC | 665 | CT | LR | The AUCs of the LR
model in differentiating high- grade serous carcinoma and
non-high-grade serous carcinoma were 0.837 (95% CI, 0.835-0.838)
for the training cohort and 0.836 (95% CI, 0.833-0.840) for the
testing cohort. | Radiomic features
extracted from contrast-enhanced CT are useful in the
classification of histological subtypes in EOC. | (52) |
| Li et al,
2021 | OC | 134 | CT | DL | The AUC in the
training set was 0.88 and the AUC in the test set was 0.87. | The model based on
CT images is helpful for the identification and prediction of
benign and malignant ovarian neoplasms. | (53) |
| Saida et al,
2022 | OC, BOT | 146 | MRI | CNN | The sensitivity,
specificity, accuracy and AUC of CNN were 0.77-0.85, 0.77-0.92,
0.81-0.87 and 0.83-0.89, respectively. The CNN showed the highest
diagnostic performance on the ADC map among all sequences
(specificity, 0.85; sensitivity, 0.77; accuracy, 0.81; AUC,
0.89). | CNNs exhibit a
diagnostic performance that is non-inferior to that of
radiologists. | (54) |
| Gao et al,
2022 | OC | 3,755 | US | CNN | Accuracy and
sensitivity of diagnosis increased more after DCNN-assisted
diagnosis than after assessment by radiologists alone [87.6%
(85.0-90.2) vs. 78.3% (72.1-84.5), P<0.0001; 82.7% (78.5-86.9)
vs. 70.4% (59.1-81.7), P<0.0001]. | The performance of
the CNN model exceeds the average diagnostic level of the
radiologist and can enhance the accuracy of the radiologist. | (55) |
| Wang et al,
2023 | EOC, BOT | 102+99 | MRI | DL | The DL model could
differentiate BOT from EOC with a higher AUC of 0.87, an accuracy
of 83.7%, a sensitivity of 75.0% and a specificity of 87.5%. | The DL model based
on MRI can distinguish BOT from EOC accurately, which is superior
to radiologists. | (56) |
| Jung et al,
2022 | OC | 1,154 | US | CNN | The accuracy of the
CNN model was 97.2%, the sensitivity was 97.2% and the AUC was
0.9936 in terms of distinguishing normal and ovarian tumors. The
CNN model showed 90.12% accuracy, 86.67% sensitivity and 0.9406 AUC
in distinguishing malignant ovarian tumors. | The CNN model can
recognize valid texture and morphology features from the US images
and classifies ovarian tumors. | (59) |
| Christiansen et
al, 2021 | OC | 758 | US | CNN | At a sensitivity of
96.0%, model 1 had a specificity similar to that of subjective
assessment (86.7% vs. 88.0%; P>0.999). Model 2 had a
sensitivity of 97.1% and a specificity of 93.7% when designating
12.7% of the lesions as inconclusive. | CNN models can
predict ovarian malignancy accurately, comparable to the human
results, which demonstrates that the models are crucial in the
triage of ovarian tumors. | (60) |
|
| B, Pathological
classification |
|
| First author,
year | Disease | Number of
patients | Type of
imaging | AI
model | Main
result | Main
conclusion | (Refs.) |
|
| Tang et al,
2022 | EOC | 154 | US | ML | The AUCs of the
training set and test set in the radiomics model and comprehensive
model were 0.817 and 0.731, and 0.982 and 0.886, respectively. | The radiomics model
based on ultra- sound has a great predictive effect for
differentiating type I and type II EOC. | (62) |
| Xu et al,
2022 | EOT | 146 | MRI | LR | The radiomics model
showed more favorable discri- mination than the clinical model
(0.915 vs. 0.852, and 0.954 vs. 0.852, respectively) in
distinguishing BOT from EOC in the training cohort. The radiomics
model was superior to the clinical model (AUC 0.905 vs. 0.735) in
classifying early stage type I and type II EOC. | Radiomics based on
DWI is an effective approach to categorize EOTs. | (63) |
| Jian et al,
2021 | EOC | 294 | MRI | LASSO | The combined
radiomics model was superior to the single-parametric radiomics
models in internal and external validation cohorts (AUCs of 0.806
and 0.847, respectively). | The radiomics model
based on MRI can differentiate type I and type II EOC. | (64) |
| Meier et al,
2019 | HGSOC | 88 | CT | GLCM | Higher values of
all three metrics were significantly associated with lower complete
surgical resection is an important tool to predict the
outcome. | The radiomics model
based on CT status in BRCA-negative patients (SE, P=0.039; SCV,
P=0.006; SCP, P=0.02), but not in BRCA-positive patients (SE,
P=0.7; SCV, P=0.91; SCP, P=0.67) | (73) |
| Wang et al,
2022 | HGSOC | 161 | PET/CT | Habitat | The texture
features generated by the Habitat could predict the Ki-67 state,
which is more efficient than the texture features extracted from
the whole tumor (P<0.001). | This model can
guide the stratification of prognosis in patients with HGSOC and is
related to the expression of Ki-67 in tumor tissues. | (76) |
|
| C,
Metastasis |
|
| First author,
year | Disease | Number of
patients | Type of
imaging | AI
model | Main
result | Main
conclusion | (Refs.) |
|
| Ai et al,
2021 | OC | 101 | CT | Ridge
Regression | The AUCs of the
radiomics model, clinical model and combined model were 0.82 (95%
CI, 0.66-0.98; sensitivity, 0.90; specificity, 0.70), 0.83 (95% CI,
0.67-0.95; sensitivity, 0.71; specificity, 0.8) and 0.86 (95% CI,
0.72-0.99; sensitivity, 0.81; specificity, 0.8), respectively. | Radiomics model can
predict the metastatic status for patients with OC. | (80) |
| Yu et al,
2021 | OC | 86 | MRI | LR | The nomogram (AUC,
0.902) constructed by combining radiomics characteristics and
clinico-pathological risk factors showed a better diagnostic effect
than the clinical model (AUC, 0.858) and the radiomics model (AUC,
0.846). | Radiomics nomogram
based on MRI has a good predictive accuracy for patients with
OC. | (81) |
|
| D, Postoperative
residue and prognosis |
|
| First author,
year | Disease | Number of
patients | Type of
imaging | AI
model | Main
result | Main
conclusion | (Refs.) |
|
| Lu et al,
2019 | EOC | 364 | CT | ML | RPV remained
significantly and continuously associated with OS in the discovery
dataset (HR, 3.83; 95% CI, 2.27-6.46; P=5.11×10−7; RPV
range, −0.322 to 3.16), as well as TCGA validation dataset (HR,
4.87; 95% CI, 1.67-14.2; P=0.0038] and the HH validation dataset
(HR, 7.36; 95% CI, 1.29-41.9; P=0.0245). | RPV and the
associated analysis platform could be exploited to guide
personalized therapy of EOC. | (85) |
| Meier et al,
2019 | HGSOC | 88 | CT | GLCM | Higher SCV was
associated with lower PFS (P=0.006) and OS (P=0.003). Higher SCP
was associated with lower PFS (P=0.02) and higher SE was correlated
with lower OS (P=0.01). | The features are
relevant to the patient PFS and OS. | (73) |
| Hong et al,
2022 | HGSOC | 119 | CT | LASSO | The nomogram showed
great discrimination in the training set (C-index, 0.754; 95% CI,
0.678-0.830), which was confirmed in the validation set (C-index,
0.727; 95% CI, 0.569-0.885). | The
radiomic-clinical nomogram can increase the predictive accuracy of
OS in patients with HGSOC after surgery. | (86) |
| Wei et al,
2019 | HGSOC | 142 | CT | LASSO | The accuracy values
of radiomic nomogram for predicting 18-month and 3-year recurrence
risks were 84.1% (95% CI, 80.5-87.7%) and 88.9% (95% CI,
85.8-92.5%), respectively. | Radiomic signature
is a potential prognostic marker, which can be used to evaluate the
patients with advanced HGSOC. | (87) |
| Wang et al,
2019 | HGSOC | 245 | CT | DL | Two patient groups
with high and low recurrence risk (P=0.0038 and P=0.0164) could be
clearly identified by Kaplan-Meier analysis. The 3-year recurrence
prediction was also effective (AUC, 0.772 and 0.825,
respectively). | The DL model based
on CT can predict the prognosis of patients with HGSOC. | (88) |
| Liu et al,
2023 | HGSOC | 185 | MRI | DL | The fusion model
that included clinical and DL features had a higher AUC (0.986 and
0.961) than the DL model (0.706 and 0.676) and the clinical model
(0.506 and 0.506) in validation cohorts 1 or 2. The model could
distinguish two patient groups with high and low recurrence risk
(P=0.0008 and P=0.0035, respectively) using the Kaplan-Meier
analysis. | DL model is a
low-cost, non-invasive method to predict the risk for recurrence of
advanced HGSOC. | (89) |
| Yao et al,
2022 | EOC | 111 | US | LASSO | The combined model
was superior to the clinical and Rad-Score models in estimating
5-year PFS and achieved an AUC of 0.868 (95% CI, 0.766-0.971) in
the training cohort. | The model that
combines clinical parameters with ultrasound radiomics features can
predict prognosis in patients with EOC. | (90) |
|
| E, Chemotherapy
drug response |
|
| First author,
year | Disease | Number of
patients | Type of
imaging | AI
model | Main
result | Main
conclusion | (Refs.) |
|
| Lei et al,
2022 | EOC | 93 | MRI | CNN | The AUCs of the
whole abdomen model were 0.97 and 0.98 for the training and
validation cohorts, respectively, which were higher than those of
the primary tumor model (AUCs of 0.88 and 0.81 in the training and
validation cohorts, respectively) | The whole-abdomen
DL model based on MRI exhibits satisfactory predictive performance
for platinum sensitivity. | (92) |
Identification of whole slide images
based on DL
A pathological biopsy is the gold standard for
diagnosing EOC, and it is also a mandatory examination mode during
postoperative chemotherapy in patients with advanced OC. The
clinician can make a more individualized treatment plan for the
patient based on the pathological findings. The traditional
pathological diagnostic method is to stain the tissue with
hematoxylin and eosin (H&E) and observe samples under a
microscope (93). However, the
method of diagnosis depends on the experience of the pathologists
and is thus subjective. Furthermore, the storage of slices is a
difficult problem after pathological diagnosis, and there are
certain limitations in remote consultation. Whole slide imaging
(WSI) can transform pathological tissue sections into
high-resolution digital images using a computer and full-slice
digital scanning technology. WSI has solved the limitations of
traditional diagnostic methods, and has improved the efficiency and
accuracy of pathological diagnosis (94). DL has been widely used in the field
of medical pathological image recognition, where it can improve the
degree of digitization of pathology and also plays a vital role in
the analysis of pathological images (95).
Prediction of different pathological
subtypes
The therapeutic scheme of OC is dependent on its
pathological subtypes, which require different chemotherapy drugs
and treatment plans. The identification of the subtypes
predominantly relies on the subjective judgment of pathologists;
however, the interobserver consistency of pathologists is often low
(Cohen's κ, 0.54-0.67) (96).
Farahani et al (96)
developed four deep CNN algorithms to identify pathological
subtypes of OC using WSI in 545 patients. The highest scoring CNN
model showed high concordance with pathologists in diagnosing OC
pathological subtypes [81.38% concordance (Cohen's κ, 0.7378) in
the training set and 80.97% concordance (Cohen's κ, 0.7547) in the
external dataset], indicating that CNN may be used as an auxiliary
diagnostic model to improve the efficiency of diagnosing OC
pathological subtypes. In addition, the model established based on
WSI had good efficacy in predicting the effect of OC chemotherapy
drugs. Wang et al (97)
developed a weakly supervised DL to accurately predict the
therapeutic effect of bevacizumab in patients with OC by analyzing
the entire image of histological H&E staining. This method can
guide clinical treatment decisions by screening out patients who
are likely to show a poor response. A Cox proportional risk model
showed that the model could predict patients at a higher risk of
recurrence due to a poor treatment response compared with patients
with a more favorable treatment response. The aforementioned
results indicated that the combination of WSI and DL in pathology
could effectively extract relevant information from high-throughput
pathological data, and provide more instructive information for
improved precision treatment.
Prediction of the mutation status of a
gene
Different pathological types of EOCs exhibit varying
gene mutation sites, with ~50% of EOCs displaying homologous
recombination repair defects. Homologous recombination repair
defects are primarily caused by mutations in the BRCA gene, which
plays a crucial role in the DNA double-strand break repair process
during homologous recombination repair and is considered an
important tumor suppressor gene (66). Patients with advanced OC carrying
BRCA1/2 mutations demonstrate increased sensitivity to
platinum-based chemotherapy drugs, and exhibit higher objective
remission rate and survival rates following treatment with
platinum-based drugs. Furthermore, the use of poly(ADP-ribose)
polymerase inhibitors after platinum-based chemotherapy can
significantly reduce the recurrence rate and the mortality rate of
patients with OC (69). Notably, a
DL model can be employed to identify gene mutations by analyzing
the H&E-stained pathological images of tumors. Ho et al
(98) utilized DL to analyze the
WSI of patients with OC and developed a model that could predict
the mutation status of the BRCA gene mutation in HGSOC. These
studies demonstrate the potential of DL based on WSI in quantifying
tumor histopathological features and related gene behavior. Nero
et al (99) applied weakly
supervised learning based on DL to analyze the WSI images of 66
patients with HGSOC. While the model exhibited zero errors in the
training set, its performance in the verification set was mediocre,
with an AUC of 0.59. In addition, this model was also used to
predict PFS, with an AUC of 0.71, indicating a good prognostic
performance.
Predict the efficacy and prognosis of
drug therapy
Currently, the standard treatment for EOC is
cytoreductive surgery combined with platinum-based chemotherapy,
but patients with different pathological types of OC have different
sensitivity levels to platinum-based chemotherapy. Laury et
al (100) utilized the WSI of
patients with HGSOC who underwent platinum-based chemotherapy with
different resultant effects in order to establish a CNN model for
predicting the effect of platinum-based chemotherapy. The CNN-based
model was effective in distinguishing patients with different
responses to platinum-based drugs, exhibiting both high sensitivity
(73%) and specificity (91%). With the occurrence of chemotherapy
resistance and refractory diseases, the sensitivity of
platinum-based chemotherapy has declined (101). Bevacizumab, an antibody against
vascular endothelial growth factor, has been used in the first- and
second-line treatments of OC. Wang et al (102) collected the WSI results of
patients with EOC and peritoneal serous papillary carcinoma, and
established a DL model to predict the therapeutic effect of
bevacizumab. The results showed that the new model could predict
the effects of treatment without guidance or prior knowledge of the
pathology. The proposed DL model could effectively distinguish
patients who would respond well from the patients whose recurrence
rate would be low after treatment and those whose disease was
likely to deteriorate after treatment. Wu et al (103) appraised the WSI results of
patients with OC through DL, and developed risk scores for these
patients. The AUC of the time-dependent ROC curve verified the good
predictive performance of risk scores. Additionally, the
researchers analyzed the differential survival rate of patients
with different homologous repair deficiency states using the
aforementioned model. The DL model not only facilitated overall
risk stratification of patients with OC, but also distinguished
between different subtypes in terms of the prognosis, which could
be used to provide a basis for targeted therapy for patients with
OC (Table II).
| Table II.Overview of the studies on AI in
WSI. |
Table II.
Overview of the studies on AI in
WSI.
| A, Prediction of
different pathological subtypes |
|---|
|
|---|
| First author,
year | Disease | Number of
patients | AI model | Main result | Main
conclusion | (Refs.) |
|---|
| Farahani et
al, 2022 | OC | 545 | ML | The best-performing
model achieved a diagnostic concordance of 81.38% (Cohen's κ,
0.7378) in the training set and 80.97% concordance (Cohen's κ,
0.7547) in the external dataset. | The CNN model may
improve the diagnostic efficiency for determining OC pathological
subtypes. | (96) |
| Wang et al,
2022 | OC | 288 | DL | For an independent
testing set, the three proposed methods obtained promising results
with high recall (sensitivity) values of 0.946, 0.893 and 0.964,
respectively. | The DL method can
help identify patients with different treatment responses. | (97) |
|
| B, Predict the
mutation status of a gene |
|
| First author,
year | Disease | Number of
patients | AI
model | Main
result | Main
conclusion | (Refs.) |
|
| Ho et al,
2023 | OC | 609 | DL | The model achieved
an intersection-over-union value of 0.74, a recall value of 0.86
and a precision value of 0.84. | The DL model can be
used to diagnose OC and find novel morphological patterns to
predict molecular subtypes. | (98) |
| Nero et al,
2022 | HGSOC | 644 | DL | The model achieved
an AUC of 0.71, with a negative predictive value of 0.69 and a
positive predictive value of 0.75 when applied to predict PFS. | The DL model based
on WSI can predict BRCA1/2 gene status. | (99) |
|
| C, Predict the
efficacy and prognosis of drug therapy |
|
| First author,
year | Disease | Number of
patients | AI
model | Main
result | Main
conclusion | (Refs.) |
|
| Laury et al,
2021 | HGSOC | 30 | CNN | The CNN model based
on WSI discriminated the response to primary platinum-based
chemotherapy with high sensitivity (73%) and specificity
(91%). | DL based image
analysis is able to. predict outcome | (100) |
| Wang et al,
2022 | EOC | 720 | DL | The model in
combination with AIM2 achieves high accuracy (0.92), recall (0.97),
F-measure (0.93) and AUC (0.97) values for the first experiment
(66% training and 34% testing) and high accuracy (0.86±0.07),
precision (0.9±0.07), recall (0.85±0.06), F-measure (0.87±0.06) and
AUC (0.91±0.05) for the second experiment using five-fold cross
validation, respectively. | AIM2-DL model can
distinguish patients gaining positive therapeutic effects with low
cancer recurrence from patients with disease progression after
treatment. | (102) |
| Wu et al,
2022 | OC | 90 | DL | The mean value of
the resulting C-index was 0.5789 (range, 0.5096-0.6053), and the
resulting P-value was 0.00845. | The DL framework is
a promising method for searching WSIs and providing a valuable
clinical means for prognosis. | (103) |
Other AI-based omics in OC
Genomics
DL models based on various other omics-based
approaches have also emerged in addition to radiography and
pathological images, and these may also play a role in exploring
the occurrence and development of diseases. Guo et al
(104) applied DL to analyze
multi-omics OC data using three datasets from the Gene Expression
Omnibus database. Furthermore, a DL framework that could integrate
multi-omics data and denoising autoencoder to identify OC subtypes
was established. The results showed that this method could be used
to identify OC subtypes at the molecular level with satisfactory
efficiency. In addition, differential expression analysis and
weighted gene co-expression network analysis were used to screen
out target genes associated with specific molecular subtypes.
Finally, 34 biomarkers and 19 Kyoto Encyclopedia of Genes and
Genomes (KEGG) pathways associated with OC were identified.
Similarly, Ye et al (105)
identified the pathogenic genes of OC based on omics data and DL.
CNN was used to predict OC-related genes, and the AUC and the area
under precision-recall curve of the model were 0.761 and 0.788
respectively, which proved the accuracy and effectiveness of the
model. Moreover, gene set enrichment analysis revealed 245 novel OC
pathogenic genes and 10 associated KEGG pathways. Cell-free tumor
DNA (cfTDNA) is also associated with the occurrence and development
of OC. cfTDNA can be released along with the occurrence of cell
necrosis and apoptosis, and the release of cancer cells. The levels
of circulating cell-free DNA (cfDNA) in patients are high, and
mostly originate from tumor cells (106). Therefore, Bahado-Singh et
al (106) performed
genome-wide DNA methylation analysis of cytosine markers and used
AI to identify the most predictive epigenetic markers in the
genome. The results revealed that the AI model based on cyclic
cfDNA cytosine methylation changes is effective in diagnosing OC
(AUC, 1.00; sensitivity, 100%; specificity, 88%).
Transcriptomics
Aghayousefi et al (107) applied a DL model to screen
microRNAs (miRNAs/miRs) related to OC occurrence, and found that
miR-1914, miR-203, miR-135a-2, miR-149 and miR-9-1 were the risk
factors associated with OC with the highest frequency. Moreover,
the study suggested that the miRNAs may participate in the
epithelial-mesenchymal transformation of cancer cells, as well as
the heterogeneous and adaptive processes of tumors. Hamidi et
al (108) compared the
differences in miRNA expression between patients with OC and
healthy individuals using the public data platform GSE106817
dataset (109). The study screened
out 10 miRNAs regulated in OC samples and developed a clinical
prediction model using ML (logistic regression, random forest,
artificial neural network, XGBoost and decision tree). ROC analysis
showed that the miRNA model exhibited a good diagnostic
performance, and the AUC of the first four prediction models was
100%, which indicated that the OC diagnostic model based on the
serum miRNA spectrum may have important clinical value.
Metabolomics
Irajizad et al (110) performed metabolomic analysis on
the serum samples from 101 patients with serous and non-serous OC,
and 134 patients with benign pelvic masses. A total of seven
cancer-related metabolites were screened using DL. The performance
of DL for OC diagnosis in the early stage was significantly
improved when combined with the risk of ovarian malignancy
algorithm.
Conclusions and future perspectives
Thus far, AI-based radiomics has shown satisfactory
efficiency in the diagnosis, differentiation and prognostic
prediction of OC. At the same time, the combination of AI models
and traditional diagnoses from clinicians can improve the accuracy
and efficiency of diagnosis, and may improve diagnostic systems in
the future. In addition, the prediction of pathological typing and
gene status may serve as a type of ‘virtual biopsy’, which could
reduce the need for invasive tests on patients in the future.
However, there remain several challenges in the clinical
application of AI in OC. Firstly, while there are an increasing
number of multi-omics studies based on genomics, transcriptomics
and proteomics, there are fewer multi-omics studies combining
radiomics and pathomics, which to some extent limits the clinical
application of AI. The integration of multi-omics data has the
potential to improve patient survival and facilitate future
precision medicine approaches. Secondly, there are several AI
algorithms, and current research only builds models around one or a
few algorithms. It is necessary to conduct a multi-center
comparison of these models to select the best AI models for general
clinical application, so this scientific research can be truly
implemented in a clinical setting. The number of clinical samples
collected by general research institutes is small and often
imbalanced in terms of representativeness of the subsequent feature
extraction, which is a challenge for AI data processing. In future
studies, considerably larger cohorts from multiple centers and
indeed cohorts from multiple countries are needed to increase the
validity of any models. Additionally, it is necessary to
continuously innovate and improve the algorithms to optimize
existing models. Finally, the clinical applications based on AI
models are mostly concentrated in thyroid diseases, breast diseases
and liver diseases, and the research of other systems remains
predominantly in the theoretical stage. In future work, these
clinical models should be used in clinical prospective studies to
assist clinicians in diagnostic and prognostic analyses. The
problems and effects encountered by clinicians when applying
artificial intelligence models should then be summarized, and the
models constantly optimized. Advances in AI-based approaches will
improve diagnostic accuracy, accelerate the diagnostic process, and
play a key role in assisting doctors in decision-making and
intelligent monitoring in the future.
In conclusion, AI has emerged as a powerful tool for
the processing of large datasets, and is being extensively utilized
in the development of diverse omics models for OC. Multi-omics
analysis, including imaging, pathomics, genomics, metabolomics and
proteomics, has demonstrated potential in enhancing the accuracy of
OC diagnoses, the differentiation between benign and malignant
cases, and the prediction of pathological types and prognosis. The
integration of multi-omics data has the potential to improve
patient survival and facilitate precision medicine in the
future.
Acknowledgements
Not applicable.
Funding
This study was funded by the Special Fund for Doctoral
Supervisors of The Second Affiliated Hospital of Fujian Medical
University (grant no. 2022BD1005).
Availability of data and materials
Not applicable.
Authors' contributions
YW, WL, GL and LL conceived and designed the
article. YW contributed to collecting data and editing the
manuscript. WL and XW contributed to researching the literature,
and revising the content with regard to obstetrics and gynecology.
XZ and YH contributed to revising the content with regard to
pathology. GL gave final approval of the manuscript. All authors
have read and approved the final version of the manuscript. The
authors guarantee that no AI tools were used to produce any content
in the article. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD, Wagle NS and Jemal
A: Cancer statistics, 2023. CA Cancer J Clin. 73:17–48. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Allemani C, Weir HK, Carreira H, Harewood
R, Spika D, Wang XS, Bannon F, Ahn JV, Johnson CJ, Bonaventure A,
et al: Global surveillance of cancer survival 1995–2009: Analysis
of individual data for 25,676,887 patients from 279
population-based registries in 67 countries (CONCORD-2). Lancet.
385:977–1010. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Millstein J, Budden T, Goode EL, Anglesio
MS, Talhouk A, Intermaggio MP, Leong HS, Chen S, Elatre W, Gilks B,
et al: Prognostic gene expression signature for high-grade serous
ovarian cancer. Ann Oncol. 31:1240–1250. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kurman RJ and Shih IM: The origin and
pathogenesis of epithelial ovarian cancer: A proposed unifying
theory. Am J Surg Pathol. 34:433–443. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schmeler KM, Tao X, Frumovitz M, Deavers
MT, Sun CC, Sood AK, Brown J, Gershenson DM and Ramirez PT:
Prevalence of lymph node metastasis in primary mucinous carcinoma
of the ovary. Obstet Gynecol. 116:269–273. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang KH and Ding DC: The role and
applications of exosomes in gynecological cancer: A review. Cell
Transplant. 32:96368972311952402023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khella CA, Mehta GA, Mehta RN and Gatza
ML: Recent advances in integrative multi-omics research in breast
and ovarian cancer. J Pers Med. 11:1492021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yu H, Wang J, Wu B, Li J and Chen R:
Prognostic significance and risk factors for pelvic and para-aortic
lymph node metastasis in type I and type II ovarian cancer: A large
population-based database analysis. J Ovarian Res. 16:282023.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chang YH, Wu KC, Harnod T and Ding DC: The
organoid: A research model for ovarian cancer. Tzu Chi Med J.
34:255–260. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kurman RJ and Shih IM: The dualistic model
of ovarian carcinogenesis: Revisited, revised, and expanded. Am J
Pathol. 186:733–747. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang T, Liu Q, Zhu Y, Huang Y, Qin J, Wu
X and Zhang S: Lymphocyte and macrophage infiltration in omental
metastases indicates poor prognosis in advance stage epithelial
ovarian cancer. J Int Med Res. 49:30006052110662452021. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shrestha P, Poudyal B, Yadollahi S, Wrigh
DE, Gregor AV, Warne JD, Korfiati P, Gree IC, Rassie SL, Mariani A,
et al: A systematic review on the use of artificial intelligence in
gynecologic imaging-Background, state of the art, and future
directions. Gynecol Oncol. 166:596–605. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mikdadi D, O'Connell KA, Meacham PJ, Dugan
MA, Ojiere MO, Carlson TB and Klenk JA: Applications of artificial
intelligence (AI) in ovarian cancer, pancreatic cancer, and image
biomarker discovery. Cancer Biomark. 33:173–184. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Breen J, Allen K, Zucker K, Adusumilli P,
Scarsbrook A, Hall G, Orsi NM and Ravikumar N: Artificial
intelligence in ovarian cancer histopathology: A systematic review.
NPJ Precis Oncol. 7:832023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lambin P, Rios-Velazquez E, Leijenaar R,
Carvalho S, van Stiphout RG, Granton P, Zegers CM, Gillies R,
Boellard R, Dekker A and Aerts HJ: Radiomics: Extracting more
information from medical images using advanced feature analysis.
Eur J Cancer. 48:441–446. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tagliafico AS, Piana M, Schenone D, Lai R,
Massone AM and Houssami N: Overview of radiomics in breast cancer
diagnosis and prognostication. Breast. 49:74–80. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Aerts HJ, Velazquez ER, Leijenaar RT,
Parmar C, Grossmann P, Carvalho S, Bussink J, Monshouwer R,
Haibe-Kains B, Rietveld D, et al: Decoding tumour phenotype by
noninvasive imaging using a quantitative radiomics approach. Nat
Commun. 5:40062014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sun R, Orlhac F, Robert C, Reuzé S,
Schernberg A, Buvat I, Deutsch E and Ferté C: In regard to mattonen
et al. Int J Radiat Oncol Biol Phys. 95:1544–1545. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tong Y, Zhang J, Wei Y, Yu J, Zhan W, Xia
H, Zhou S, Wang Y and Chang C: Ultrasound-based radiomics analysis
for preoperative prediction of central and lateral cervical lymph
node metastasis in papillary thyroid carcinoma: A
multi-institutional study. BMC Med Imaging. 22:822022. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Du Y, Zha HL, Wang H, Liu XP, Pan JZ, Du
LW, Cai MJ, Zong M and Li CY: Ultrasound-based radiomics nomogram
for differentiation of triple-negative breast cancer from
fibroadenoma. Br J Radiol. 95:202105982022. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Peng Y, Lin P, Wu L, Wan D, Zhao Y, Liang
L, Ma X, Qin H, Liu Y, Li X, et al: Ultrasound-Based radiomics
analysis for preoperatively predicting different histopathological
subtypes of primary liver cancer. Front Oncol. 10:16462020.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ou W, Lei J, Li M, Zhang X, Liang R, Long
L, Wang C, Chen L, Chen J, Zhang J and Wang Z: Ultrasound-based
radiomics score for pre-biopsy prediction of prostate cancer to
reduce unnecessary biopsies. Prostate. 83:109–118. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Avesani G, Tran HE, Cammarata G, Botta F,
Raimondi S, Russo L, Persiani S, Bonatti M, Tagliaferri T, Dolciami
M, et al: CT-based radiomics and deep learning for BRCA mutation
and progression-free survival prediction in ovarian cancer using a
multicentric dataset. Cancers (Basel). 14:23792022. View Article : Google Scholar
|
|
25
|
Levy MA, Freymann JB, Kirby JS, Fedorov A,
Fennessy FM, Eschrich SA, Berglund AE, Fenstermacher DA, Tan Y, Guo
X, et al: Informatics methods to enable sharing of quantitative
imaging research data. Magn Reson Imaging. 30:1249–1256. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Beer L, Martin-Gonzalez P, Delgado-Ortet
M, Reinius M, Rundo L, Woitek R, Ursprung S, Escudero L, Sahin H,
Funingana IG, et al: Ultrasound-guided targeted biopsies of
CT-based radiomic tumour habitats: Technical development and
initial experience in metastatic ovarian cancer. Eur Radiol.
31:3765–3772. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Karimi D, Dou H, Warfield SK and Gholipour
A: Deep learning with noisy labels: Exploring techniques and
remedies in medical image analysis. Med Image Anal. 65:1017592020.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kumar V, Gu Y, Basu S, Berglund A,
Eschrich SA, Schabath MB, Forster K, Aerts HJ, Dekker A,
Fenstermacher D, et al: Radiomics: The process and the challenges.
Magn Reson Imaging. 30:1234–1248. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Peeken JC, Bernhofer M, Wiestler B,
Goldberg T, Cremers D, Rost B, Wilkens JJ, Combs SE and Nüsslin F:
Radiomics in radiooncology-challenging the medical physicist. Phys
Med. 48:27–36. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Koh YW, Lee D and Lee SJ: Intratumoral
heterogeneity as measured using the tumor-stroma ratio and PET
texture analyses in females with lung adenocarcinomas differs from
that of males with lung adenocarcinomas or squamous cell
carcinomas. Medicine (Baltimore). 98:e148762019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Busnatu Ș, Niculescu AG, Bolocan A,
Petrescu GED, Păduraru DN, Năstasă I, Lupușoru M, Geantă M,
Andronic O, Grumezescu AM and Martins H: Clinical applications of
artificial intelligence-an updated overview. J Clin Med.
11:22652022. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Oakden-Rayner L, Carneiro G, Bessen T,
Nascimento JC, Bradley AP and Palmer LJ: Precision radiology:
Predicting longevity using feature engineering and deep learning
methods in a radiomics framework. Sci Rep. 7:16482017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Li W, Dong S, Wang H, Wu R, Wu H, Tang ZR,
Zhang J, Hu Z and Yin C: Risk analysis of pulmonary metastasis of
chondrosarcoma by establishing and validating a new clinical
prediction model: A clinical study based on SEER database. BMC
Musculoskelet Disord. 22:5292021. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chen L, Zeng H, Xiang Y, Huang Y, Luo Y
and Ma X: Histopathological images and multi-omics integration
predict molecular characteristics and survival in lung
adenocarcinoma. Front Cell Dev Biol. 9:7201102021. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Guo S, Tian M, Fan Y and Zhang X: Recent
advances in mass spectrometry-based proteomics and metabolomics in
chronic rhinosinusitis with nasal polyps. Front Immunol.
14:12671942023. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zeng H, Chen L, Zhang M, Luo Y and Ma X:
Integration of histopathological images and multi-dimensional omics
analyses predicts molecular features and prognosis in high-grade
serous ovarian cancer. Gynecol Oncol. 163:171–180. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Gupta R, Srivastava D, Sahu M, Tiwari S,
Ambasta RK and Kumar P: Artificial intelligence to deep learning:
Machine intelligence approach for drug discovery. Mol Divers.
25:1315–1360. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
European Society of Radiology (ESR), .
What the radiologist should know about artificial intelligence-an
ESR white paper. Insights Imaging. 10:442019. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Joda T, Bornstein MM, Jung RE, Ferrari M,
Waltimo T and Zitzmann NU: Recent trends and future direction of
dental research in the digital era. Int J Environ Res Public
Health. 17:19872020. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Covas P, De Guzman E, Barrows I, Bradley
AJ, Choi BG, Krepp JM, Lewis JF, Katz R, Tracy CM, Zeman RK, et al:
Artificial intelligence advancements in the cardiovascular imaging
of coronary atherosclerosis. Front Cardiovasc Med. 9:8394002022.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Li W, Dong Y, Liu W, Tang Z, Sun C, Lowe
S, Chen S, Bentley R, Zhou Q, Xu C, et al: A deep belief
network-based clinical decision system for patients with
osteosarcoma. Front Immunol. 13:10033472022. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Chen L, Han Z, Wang J and Yang C: The
emerging roles of machine learning in cardiovascular diseases: A
narrative review. Ann Transl Med. 10:6112022. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhao J, Luo Y, Xiao R, Wu R and Fan T:
Tri-training algorithm for adaptive nearest neighbor density
editing and cross entropy evaluation. Entropy (Basel). 25:4802023.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Awassa L, Jdey I, Dhahri H, Hcini G,
Mahmood A, Othman E and Haneef M: Study of different deep learning
methods for coronavirus (COVID-19) pandemic: Taxonomy, survey and
insights. Sensors (Basel). 22:18902022. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhang Z, Zhu Y, Liu M, Zhang Z, Zhao Y,
Yang X, Xie M and Zhang L: Artificial intelligence-enhanced
echocardiography for systolic function assessment. J Clin Med.
11:28932022. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Chen S, Zhao S and Lan Q: Residual block
based nested U-type architecture for multi-modal brain tumor image
segmentation. Front Neurosci. 16:8328242022. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Park CW, Oh SJ, Kim KS, Jang MC, Kim IS,
Lee YK, Chung MJ, Cho BH and Seo SW: Artificial intelligence-based
classification of bone tumors in the proximal femur on plain
radiographs: System development and validation. PLoS One.
17:e02641402022. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wu W, Huang Y and Wu X: A new deep
learning method with self-supervised learning for delineation of
the electrocardiogram. Entropy (Basel). 24:18282022. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Kaka H, Zhang E and Khan N: Artificial
intelligence and deep learning in neuroradiology: Exploring the new
frontier. Can Assoc Radiol J. 72:35–44. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Liu P, Liang X, Liao S and Lu Z: Pattern
classification for ovarian tumors by integration of radiomics and
deep learning features. Curr Med Imaging. 18:1486–1502. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Qin X, Hu X, Xiao W, Zhu C, Ma Q and Zhang
C: Preoperative evaluation of hepatocellular carcinoma
differentiation using contrast-enhanced ultrasound-based
deep-learning radiomics model. J Hepatocell Carcinoma. 10:157–168.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wang M, Perucho JAU, Hu Y, Choi MH, Han L,
Wong EMF, Ho G, Zhang X, Ip P and Lee EYP: Computed tomographic
radiomics in differentiating histologic subtypes of epithelial
ovarian carcinoma. JAMA Netw Open. 5:e22451412022. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Li S, Liu J, Xiong Y, Pang P, Lei P, Zou
H, Zhang M, Fan B and Luo P: A radiomics approach for automated
diagnosis of ovarian neoplasm malignancy in computed tomography.
Sci Rep. 11:87302021. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Saida T, Mori K, Hoshiai S, Sakai M,
Urushibara A, Ishiguro T, Minami M, Satoh T and Nakajima T:
Diagnosing ovarian cancer on MRI: A preliminary study comparing
deep learning and radiologist assessments. Cancers (Basel).
14:9872022. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Gao Y, Zeng S, Xu X, Li H, Yao S, Song K,
Li X, Chen L, Tang J, Xing H, et al: Deep learning-enabled pelvic
ultrasound images for accurate diagnosis of ovarian cancer in
China: A retrospective, multicentre, diagnostic study. Lancet Digit
Health. 4:e179–e187. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Wang Y, Zhang H, Wang T, Yao L, Zhang G,
Liu X, Yang G and Yuan L: Deep learning for the ovarian lesion
localization and discrimination between borderline and malignant
ovarian tumors based on routine MR imaging. Sci Rep. 13:27702023.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Andreotti RF, Timmerman D, Strachowski LM,
Froyman W, Benacerraf BR, Bennett GL, Bourne T, Brown DL, Coleman
BG, Frates MC, et al: O-RADS US risk stratification and management
system: A consensus guideline from the ACR ovarian-adnexal
reporting and data system committee. Radiology. 294:168–185. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Chen H, Yang BW, Qian L, Meng YS, Bai XH,
Hong XW, He X, Jiang MJ, Yuan F, Du QW and Feng WW: Deep learning
prediction of ovarian malignancy at US compared with O-RADS and
expert assessment. Radiology. 304:106–113. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Jung Y, Kim T, Han MR, Kim S, Kim G, Lee S
and Choi YJ: Ovarian tumor diagnosis using deep convolutional
neural networks and a denoising convolutional autoencoder. Sci Rep.
12:170242022. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Christiansen F, Epstein EL, Smedberg E,
Åkerlund M, Smith K and Epstein E: Ultrasound image analysis using
deep neural networks for discriminating between benign and
malignant ovarian tumors: Comparison with expert subjective
assessment. Ultrasound Obstet Gynecol. 57:155–163. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Harris HR, Guertin KA, Camacho TF, Johnson
CE, Wu AH, Moorman PG, Myers E, Bethea TN, Bandera EV, Joslin CE,
et al: Racial disparities in epithelial ovarian cancer survival: An
examination of contributing factors in the ovarian cancer in women
of African Ancestry consortium. Int J Cancer. 151:1228–1239. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Tang ZP, Ma Z, He Y, Liu RC, Jin BB, Wen
DY, Wen R, Yin HH, Qiu CC, Gao RZ, et al: Ultrasound-based
radiomics for predicting different pathological subtypes of
epithelial ovarian cancer before surgery. BMC Med Imaging.
22:1472022. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Xu Y, Luo HJ, Ren J, Guo LM, Niu J and
Song X: Diffusion-weighted imaging-based radiomics in epithelial
ovarian tumors: Assessment of histologic subtype. Front Oncol.
12:9781232022. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Jian J, Li Y, Pickhardt PJ, Xia W, He Z,
Zhang R, Zhao S, Zhao X, Cai S, Zhang J, et al: MR image-based
radiomics to differentiate type I and type II epithelial ovarian
cancers. Eur Radiol. 31:403–410. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Konstantinopoulos PA, Ceccaldi R, Shapiro
GI and D'Andrea AD: Homologous recombination deficiency: Exploiting
the fundamental vulnerability of ovarian cancer. Cancer Discov.
5:1137–1154. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Tutt A, Tovey H, Cheang MCU, Kernaghan S,
Kilburn L, Gazinska P, Owen J, Abraham J, Barrett S, Barrett-Lee P,
et al: Carboplatin in BRCA1/2-mutated and triple-negative breast
cancer BRCAness subgroups: The TNT trial. Nat Med. 24:628–637.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Golan T, Sella T, O'Reilly EM, Katz MH,
Epelbaum R, Kelsen DP, Borgida A, Maynard H, Kindler H, Friedmen E,
et al: Overall survival and clinical characteristics of BRCA
mutation carriers with stage I/II pancreatic cancer. Br J Cancer.
116:697–702. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Li MR, Liu MZ, Ge YQ, Zhou Y and Wei W:
Assistance by routine CT features combined with 3D texture analysis
in the diagnosis of BRCA gene mutation status in advanced
epithelial ovarian cancer. Front Oncol. 11:6967802021. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Moore K, Colombo N, Scambia G, Kim BG,
Oaknin A, Friedlander M, Lisyanskaya A, Floquet A, Leary A, Sonke
GS, et al: Maintenance olaparib in patients with newly diagnosed
advanced ovarian cancer. N Engl J Med. 379:2495–2505. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Soslow RA, Han G, Park KJ, Garg K, Olvera
N, Spriggs DR, Kauff ND and Levine DA: Morphologic patterns
associated with BRCA1 and BRCA2 genotype in ovarian carcinoma. Mod
Pathol. 25:625–636. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Alsop K, Fereday S, Meldrum C, deFazio A,
Emmanuel C, George J, Dobrovic A, Birrer MJ, Webb PM, Stewart C, et
al: BRCA mutation frequency and patterns of treatment response in
BRCA mutation-positive women with ovarian cancer: A report from the
Australian ovarian cancer study group. J Clin Oncol. 30:2654–2663.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Sánchez-Lorenzo L, Salas-Benito D,
Villamayor J, Patiño-García A and González-Martín A: The BRCA gene
in epithelial ovarian cancer. Cancers (Basel). 14:12352022.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Meier A, Veeraraghavan H, Nougaret S,
Lakhman Y, Sosa R, Soslow RA, Sutton EJ, Hricak H, Sala E and
Vargas HA: Association between CT-texture-derived tumor
heterogeneity, outcomes, and BRCA mutation status in patients with
high-grade serous ovarian cancer. Abdom Radiol (NY). 44:2040–2047.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Verhaak RG, Tamayo P, Yang JY, Hubbard D,
Zhang H, Creighton CJ, Fereday S, Lawrence M, Carter SL, Mermel CH,
et al: Prognostically relevant gene signatures of high-grade serous
ovarian carcinoma. J Clin Invest. 123:517–525. 2013.PubMed/NCBI
|
|
75
|
Vargas HA, Huang EP, Lakhman Y, Ippolito
JE, Bhosale P, Mellnick V, Shinagare AB, Anello M, Kirby J,
Fevrier-Sullivan B, et al: Radiogenomics of high-grade serous
ovarian cancer: Multireader multi-institutional study from the
cancer genome atlas ovarian cancer imaging research group.
Radiology. 285:482–492. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Wang X, Xu C, Grzegorzek M and Sun H:
Habitat radiomics analysis of pet/ct imaging in high-grade serous
ovarian cancer: Application to Ki-67 status and progression-free
survival. Front Physiol. 13:9487672022. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Heintz AP, Odicino F, Maisonneuve P, Quinn
MA, Benedet JL, Creasman WT, Ngan HY, Pecorelli S and Beller U:
Carcinoma of the ovary. FIGO 26th annual report on the results of
treatment in gynecological cancer. Int J Gynaecol Obstet. 95 (Suppl
1):S161–S192. 2006.
|
|
78
|
Suidan RS, Ramirez PT, Sarasohn DM,
Teitcher JB, Mironov S, Iyer RB, Zhou Q, Iasonos A, Paul H, Hosaka
M, et al: A multicenter prospective trial evaluating the ability of
preoperative computed tomography scan and serum CA-125 to predict
suboptimal cytoreduction at primary debulking surgery for advanced
ovarian, fallopian tube, and peritoneal cancer. Gynecol Oncol.
134:455–461. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Peng Z, Lin Z, He A, Yi L, Jin M, Chen Z,
Tao Y, Yang Y, Cui C, Liu Y and Zuo M: Development and validation
of a comprehensive model for predicting distant metastasis of solid
lung adenocarcinoma: 3D radiomics, 2D radiomics and clinical
features. Cancer Manag Res. 14:3437–3448. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Ai Y, Zhang J, Jin J, Zhang J, Zhu H and
Jin X: Preoperative prediction of metastasis for ovarian cancer
based on computed tomography radiomics features and clinical
factors. Front Oncol. 11:6107422021. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Yu XY, Ren J, Jia Y, Wu H, Niu G, Liu A,
Gao Y, Hao F and Xie L: Multiparameter MRI radiomics model predicts
preoperative peritoneal carcinomatosis in ovarian cancer. Front
Oncol. 11:7656522021. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Chien J and Poole EM: Ovarian cancer
prevention, screening, and early detection: Report from the 11th
biennial ovarian cancer research symposium. Int J Gynecol Cancer.
27:S20–S22. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Yang R, Niepel M, Mitchison TK and Sorger
PK: Dissecting variability in responses to cancer chemotherapy
through systems pharmacology. Clin Pharmacol Ther. 88:34–38. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Luvero D, Milani A and Ledermann JA:
Treatment options in recurrent ovarian cancer: Latest evidence and
clinical potential. Ther Adv Med Oncol. 6:229–239. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Lu H, Arshad M, Thornton A, Avesani G,
Cunnea P, Curry E, Kanavati F, Liang J, Nixon K, Williams ST, et
al: A mathematical-descriptor of tumor-mesoscopic-structure from
computed-tomography images annotates prognostic- and
molecular-phenotypes of epithelial ovarian cancer. Nat Commun.
10:7642019. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Hong Y, Liu Z, Lin D, Peng J, Yuan Q, Zeng
Y, Wang X and Luo C: Development of a radiomic-clinical nomogram
for prediction of survival in patients with serous ovarian cancer.
Clin Radiol. 77:352–359. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Wei W, Liu Z, Rong Y, Zhou B, Bai Y, Wei
W, Wang S, Wang M, Guo Y and Tian J: A computed tomography-based
radiomic prognostic marker of advanced high-grade serous ovarian
cancer recurrence: A multicenter study. Front Oncol. 9:2552019.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Wang S, Liu Z, Rong Y, Zhou B, Bai Y, Wei
W, Wei W, Wang M, Guo Y and Tian J: Deep learning provides a new
computed tomography-based prognostic biomarker for recurrence
prediction in high-grade serous ovarian cancer. Radiother Oncol.
132:171–177. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Liu L, Wan H, Liu L, Wang J, Tang Y, Cui S
and Li Y: Deep learning provides a new magnetic resonance
imaging-based prognostic biomarker for recurrence prediction in
high-grade serous ovarian cancer. Diagnostics (Basel). 13:7482023.
View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Yao F, Ding J, Hu Z, Cai M, Liu J, Huang
X, Zheng R, Lin F and Lan L: Ultrasound-based radiomics score: A
potential biomarker for the prediction of progression-free survival
in ovarian epithelial cancer. Abdom Radiol (NY). 46:4936–4945.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Laios A, De Freitas DLD, Saalmink G, Tan
YS, Johnson R, Zubayraeva A, Munot S, Hutson R, Thangavelu A,
Broadhead T, et al: Stratification of length of stay prediction
following surgical cytoreduction in advanced high-grade serous
ovarian cancer patients using artificial intelligence; the leeds
L-AI-OS score. Curr Oncol. 29:9088–9104. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Lei R, Yu Y, Li Q, Ya Q, Wan J, Ga M, Zhuo
W, Ren W, Ta Y, Zhan B, et al: Deep learning magnetic resonance
imaging predicts platinum sensitivity in patients with epithelial
ovarian cancer. Front Oncol. 12:8951772022. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Fereidouni F and Levenson R: Beyond
brightfield: A possible future of slide scanners. Biotechniques.
70:5–6. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Boehm KM, Aherne EA, Ellenson L,
Nikolovski I, Alghamdi M, Vázquez-García I, Zamarin D, Roche KL,
Liu Y, Patel D, et al: Multimodal data integration using machine
learning improves risk stratification of high-grade serous ovarian
cancer. Nat Cancer. 3:723–733. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Jiang Z, Song L, Lu H and Yin J: The
potential use of DCE-MRI texture analysis to predict HER2 2+
status. Front Oncol. 9:2422019. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Farahani H, Boschman J, Farnell D,
Darbandsari A, Zhang A, Ahmadvand P, Jones SJM, Huntsman D, Köbel
M, Gilks CB, et al: Deep learning-based histotype diagnosis of
ovarian carcinoma whole-slide pathology images. Mod Pathol.
35:1983–1990. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Wang CW, Chang CC, Lee YC, Lin YJ, Lo SC,
Hsu PC, Liou YA, Wang CH and Chao TK: Weakly supervised deep
learning for prediction of treatment effectiveness on ovarian
cancer from histopathology images. Comput Med Imaging Graph.
99:1020932022. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Ho DJ, Chui MH, Vanderbilt CM, Jung J,
Robson ME, Park CS, Roh J and Fuchs TJ: Deep interactive
learning-based ovarian cancer segmentation of H&E-stained whole
slide images to study morphological patterns of BRCA mutation. J
Pathol Inform. 14:1001602023. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Nero C, Boldrini L, Lenkowicz J, Giudice
MT, Piermattei A, Inzani F, Pasciuto T, Minucci A, Fagotti A,
Zannoni G, et al: Deep-learning to predict BRCA mutation and
survival from digital H&E slides of epithelial ovarian cancer.
Int J Mol Sci. 23:113262022. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Laury AR, Blom S, Ropponen T, Virtanen A
and Carpén OM: Artificial intelligence-based image analysis can
predict outcome in high-grade serous carcinoma via histology alone.
Sci Rep. 11:191652021. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Lim HJ and Ledger W: Targeted therapy in
ovarian cancer. Womens Health (Lond). 12:363–378. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Wang CW, Lee YC, Chang CC, Lin YJ, Liou
YA, Hsu PC, Chang CC, Sai AK, Wang CH and Chao TK: A weakly
supervised deep learning method for guiding ovarian cancer
treatment and identifying an effective biomarker. Cancers (Basel).
14:16512022. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Wu M, Zhu C, Yang J, Cheng S, Yang X, Gu
S, Xu S, Wu Y, Shen W, Huang S and Wang Y: Exploring prognostic
indicators in the pathological images of ovarian cancer based on a
deep survival network. Front Genet. 13:10696732022. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Guo LY, Wu AH, Wang YX, Zhang LP, Chai H
and Liang XF: Deep learning-based ovarian cancer subtypes
identification using multi-omics data. BioData Min. 13:102020.
View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Ye L, Zhang Y, Yang X, Shen F and Xu B: An
ovarian cancer susceptible gene prediction method based on deep
learning methods. Front Cell Dev Biol. 9:7304752021. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Bahado-Singh RO, Ibrahim A, Al-Wahab Z,
Aydas B, Radhakrishna U, Yilmaz A and Vishweswaraiah S: Precision
gynecologic oncology: Circulating cell free DNA epigenomic
analysis, artificial intelligence and the accurate detection of
ovarian cancer. Sci Rep. 12:186252022. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Aghayousefi R, Khatibi SM, Vahed SZ,
Bastami M, Pirmoradi S and Teshnehlab M: A diagnostic miRNA panel
to detect recurrence of ovarian cancer through artificial
intelligence approaches. J Cancer Res Clin Oncol. 149:325–341.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Hamidi F, Gilani N, Belaghi RA, Sarbakhsh
P, Edgünlü T and Santaguida P: Exploration of potential miRNA
biomarkers and prediction for ovarian cancer using artificial
intelligence. Front Genet. 12:7247852021. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Yokoi A, Matsuzaki J, Yamamoto Y, Yoneoka
Y, Takahashi K, Shimizu H, Uehara T, Ishikawa M, Ikeda SI, Sonoda
T, et al: Integrated extracellular microRNA profiling for ovarian
cancer screening. Nat Commun. 9:43192018. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Irajizad E, Han CY, Celestino J, Wu R,
Murage E, Spencer R, Dennison JB, Vykoukal J, Long JP, Do KA, et
al: A blood-based metabolite panel for distinguishing ovarian
cancer from benign pelvic masses. Clin Cancer Res. 28:4669–4676.
2022. View Article : Google Scholar : PubMed/NCBI
|