Introduction
Acute myocardial infarction is one of main causes of
cardiac insufficiency. When complicated by decompensated heart
failure, it is one of the primary causes of mortality from coronary
heart disease. Certain patients present with acute decompensated
heart failure despite receiving standardized anticoagulation and
anti-ischemia treatment (including thrombolysis and emergency
percutaneous coronary intervention), which necessitates the use of
an appropriate cardiotonic to improve the clinical symptoms and
prognosis. Recombinant human brain natriuretic peptide (rhBNP) is
used to treat acute decompensated heart failure (1–3).
Bone mesenchymal stem cells (BMSCs) are of
particular interest to researchers due to their potential to
differentiate into myocardial cells, which are convenient and have
low tendency to cause immunological reactions and rejection
(4–6). In recent years, animal experiments
involving BMSC transplantation have been successfully conducted and
transplanted BMSCs have been confirmed to improve cardiac function
(7–10). However, the results of previous
clinical studies using BMSCs are unsatisfactory. BMSCs for use in
transplantation are not produced through pure cultures; thus, the
transplanted stem cells may be reduced and variable in number, with
even fewer transplanted cells surviving to undergo differentiation
(11,12). Therefore, numerous studies
concerning the treatment of cardiac diseases have focused on
identifying non-toxic methods to enhance the survival rate of
transplanted cells and to promote their differentiation into
myocardial cells. In the current study, a heart failure (HF) model
was established in rats. The recombinant hormone rhBNP was
administered to the rats in conjunction with BMSC transplantation
to investigate the effects of the combination treatment on heart
function. The survival rate of the BMSCs in the myocardial tissue
and the expression levels of myocardium-specific proteins were also
determined to gain new insights into the treatment of heart failure
with BMSCs.
Materials and methods
Animals
A total of 40 healthy male Wistar outbred rats, 6–7
weeks old with body weights of 200–220 g were selected for the
study. According to the method proposed by Siveski-Iliskovic et
al(13), a HF model was
established in the rats. Adriamycin was administered at a dose of
2.5 mg/kg by intraperitoneal injection three times per week for one
week. After a two-week interval, Adriamycin was administered for
another week. These steps were conducted six times until the total
dose reached 15 mg/kg. Following the last injection, the rats were
continually observed for 4 weeks. This study was carried out in
strict accordance with the recommendations in the Guide for the
Care and Use of Laboratory Animals of the National Institutes of
Health. The animal use protocol has been reviewed and approved by
the Institutional Animal Care and Use Committee (IACUC) of The
First Affiliated Hospital of Xinxiang Medical University.
Isolation and culture of BMSCs
The rats were sacrificed and soaked in 75% ethanol
for 10 min. Under sterile conditions, the femurs and tibias were
bilaterally dissected to expose the epiphyseal plates. An injector
containing phosphate-buffered saline (PBS) was inserted to rinse
out the bone marrow completely until the bone cavity became white.
Subsequently, the rinsed bone marrow was blown and beaten into a
cell suspension. The suspension was centrifuged for 10 min at 1,500
rpm to remove the supernatant liquid. An appropriate amount of
Dulbecco’s modified Eagle’s medium was added to the precipitate and
the mixture was blown into a cell suspension and placed into
culture flasks for cell culturing. The culture medium was replaced
after 72 h, and then again every 2–3 days thereafter. When the
cells reached >80% confluence, they were digested with 0.25%
pancreatin and passaged to a ratio of 1:2 or 1:3. Cell morphology
was observed under a phase contrast microscope daily during
passage. The fourth generation of purified cells was selected for
cell labeling prior to transplantation. Two days before
transplantation, the cells were inoculated into 25-mm culture
dishes. Upon reaching 60% confluence, bromodeoxyuridine was added
to the cells at a final concentration of 10 mol/l. After incubation
for 48 h, the culture medium was removed and the remaining
suspension was digested and centrifuged to collect the cells. The
collected cells were stored on ice for transplantation.
Grouping
The rats were divided into five experimental groups:
i) the normal group (untreated normal healthy rats); ii) the HF
group (HF model rats injected with an equivalent amount of normal
saline via the tail vein); iii) the BMSC group (HF model rats
injected with ~107 cultured BMSCs in 100 μl via the tail
vein); iv) the rhBNP group (HF model rats treated with 15 g/kg
rhBNP via the jugular vein once daily for 4 weeks); and v) the BMSC
plus rhBNP group (HF model rats injected once with an equivalent
amount of BMSCs and an equivalent amount of rhBNP via the tail
vein). After the corresponding treatments, the groups were observed
for 4 weeks and the related indicators were measured.
Echocardiography
Following the 4-week treatment, high-frequency
echocardiographic examination of the chest was conducted using a GE
Vivid 7 Color Doppler Ultrasound Imaging Instrument (GE Company,
Fairfield, USA). High-frequency ultrasonography was conducted with
a l0S probe along the chest wall at 11.4 MHz, with an image depth
of 2.0 cm. A dose of 800 mg/kg urethane (20%) was administered by
intraperitoneal injection. Using two-dimensional ultrasound, the
left ventricular end-systolic diameter (LVSD), the left ventricular
end-diastolic diameter (LVDD), the left ventricular end-systolic
volume (LVSV) and the left ventricular end-diastolic volume (LVDV)
were detected with an M-mode ultrasound. For each parameter, three
measurements were taken under a consecutive complete heartbeat
cycle and the mean was obtained. The left ventricular ejection
fraction (LVEF) and the left ventricular shortening fraction (LVFS)
were converted according to Simpson’s method.
Polygraph detection of heart
function
Following the 4-week treatment, the rats were
anesthetized. The right common carotid artery was isolated and a
catheter was inserted into the left ventricle. A polygraph was used
to record the left ventricular systolic pressure (LVSP), the left
ventricular diastolic pressure (LVDP), the heart rate and the
maximum variations in left ventricular pressure rise and decline
(±dp/dtmax). The data were continuously measured 5 times
at 3-min intervals. The results were expressed as the mean of at
least 3 stable measurements.
Serum BNP detection
For the various treatment groups, blood was drawn
via the tail vein in the morning from the fasted rats. This was
performed prior to and following the 4-week treatment. The blood
samples were centrifuged to collect the serum. An enzyme-linked
immunosorbent assay was used to detect the serum BNP levels
according to the manufacturer’s instructions (Boster Company,
Wuhan, China).
Western blot
Following the 4-week treatment, the rats were
sacrificed and thoracotomy was immediately conducted to remove the
heart. The hearts were washed with PBS and samples of the left
ventricular myocardial tissue were weighed and homogenized in 10 ml
cell lysis solution per 1 mg tissue. The homogenate was centrifuged
at 10,000 rpm for 10 min at 4°C and the tissue supernatant liquid
was collected for further use. Western blot analysis was used to
detect the expression levels of myocardium-specific proteins in the
tissue sample. Antibodies specific for cardiac troponin I (cTnI;
1:300 dilution), connexin 43 (Cx43; 1:300 dilution) and GAT-binding
protein 4 (GATA-4; 1:200 dilution) were used as primary antibodies
(Boster Company, Wuhan, China).
Statistical analysis
The SPSS 16.0 statistical package was used for all
statistical analyses. Measured data were analyzed by the
paired-samples Student’s t-test. The correlation between data was
analyzed by the Spearman’s rank test. P<0.05 was considered to
indicate a statistically significant result.
Results
Animal models
In this experiment, 40 rats were used for modeling,
but only 34 rats survived for further experimentation. Four of the
rats suddenly died of unknown causes, whereas two other rats died
of massive ascites. Echocardiography was conducted on the rats
before and after modeling. The detection results show significant
differences in the LVDD and LVSD of the rats before and after
modeling (6.52±0.76 vs. 4.18±0.21 mm and 3.81±0.76 vs. 1.10±0.15
mm, respectively; P<0.05). Significant differences were also
observed in their LVEF and LVFS before and after modelling
(75.34±8.45 vs. 94.51±2.61% and 41.28±1.93 vs. 73.68±1.87%,
respectively; P<0.05). Using the HF model establishment
criteria, the LVEF and LVFS dropped by 20–30% of the normal
reference values. Five rats presented no evident expansion of their
ventricular chamber and had no clear decrease in LVEF. Therefore,
these animals were excluded. A total of 29 model rats that
fulfilled the HF criteria survived.
Comparison of heart function
The echocardiographic findings in the HF group
revealed the typical manifestations of cardiomyopathy and heart
failure: the LVSD and LVDD were clearly enlarged and the LVFS and
LVEF evidently reduced, which suggest a decline in left heart
function. The LVSD, LVDD, LVEF and LVFS in the BMSC, the rhBNP and
the BMSC plus rhBNP groups were all significantly different from
those in the HF group (P<0.05), which suggests that the left
heart functions of these three groups had improved. Among these
three groups, the systolic function in the BMSC plus rhBNP group
exhibited the most improvement. The improvement was significantly
higher than those in the BMSC and rhBNP groups (P<0.05).
However, the differences between the BMSC and rhBNP groups were not
statistically significant (P>0.05; Table I).
 | Table ICardiac functions of rats with heart
failure analyzed by echocardiography 4 weeks after injection (mean
± s). |
Table I
Cardiac functions of rats with heart
failure analyzed by echocardiography 4 weeks after injection (mean
± s).
| Group | n | LVDD (mm) | LVSD (mm) | LVEF (%) | LVFS (%) |
|---|
| Normal | 6 | 4.21±0.09 | 1.03±0.21 | 74.21±1.49 | 44.21±1.78 |
| HF | 6 | 6.75±0.42a | 4.25±0.12a | 47.75±2.42a | 20.15±1.04a |
| BMSC | 8 | 5.56±0.71b | 2.26±0.91b,c | 55.56±2.73b,c | 25.26±1.91b,c |
| BMSC + rhBNP | 8 | 5.32±0.65b,c | 2.32±0.06b,c | 65.32±4.35b–d | 29.12±1.05b–d |
| rhBNP | 7 | 6.23±0.61 | 3.33±0.41 | 56.65±3.61b | 24.23±1.61 |
Hemodynamic indicators
Following the 4-week treatment, the
hemodynamic-related indicators among the various groups were
significantly different (P<0.05). The LVSP and the
±dp/dtmax of the BMSC, the rhBNP and the BMSC plus rhBNP
groups were significantly increased and their LVDP values were
significantly decreased compared with those of the HF group
(P<0.01). These results suggest that the cardiac function had
improved, but was not significantly improved over that in the
normal group (P<0.05). Compared with the other groups, the
±dp/dtmax in the BMSC plus rhBNP group was significantly
improved (P<0.05). No significant differences were observed
between the BMSC and rhBNP groups (P>0.05; Table II).
| Table IIHemodynamic data of rats with heart
failure 4 weeks after injection (mean ± s). |
Table II
Hemodynamic data of rats with heart
failure 4 weeks after injection (mean ± s).
| Group | n | LVSP (kPa) | LVDP (kPa) | +dp/dtmax
(kPa/sec) | −dp/dtmax
(kPa/sec) |
|---|
| Normal | 6 | 21.24±1.09 | −0.32±0.24 | 974.21±71.39 | 724.21±91.78 |
| HF | 6 | 14.35±2.62 | 0.85±0.36 | 331.45±55.82 | 372.05±46.84 |
| BMSC | 8 | 16.56±2.73a | 0.31±0.21a | 575.56±27.73a | 475.12±47.71a |
| BMSC + rhBNP | 8 | 18.02±3.85a | 0.22±0.46a | 635.52±34.85ab | 649.52±44.55a,b |
| rhBNP | 7 | 16.03±3.31a | 0.33±0.26a | 556.65±13.64a | 524.83±24.61a |
Change of serum BNP levels
Compared with the normal group, the BNP levels of
the various treatment groups were significantly increased following
treatment. No significant differences in BNP levels were observed
among the BMSC, the rhBNP and the BMSC plus rhBNP groups, either
before or after treatment (P<0.05). However, following the
intervention, the BNP levels of these groups were significantly
reduced compared with those of the control group (P<0.05).
Following the treatment, the BNP levels in the BMSC plus rhBNP
group were significantly reduced compared with those in the BMSC
and rhBNP groups (P<0.05). No significant difference in BNP
levels was observed between the BMSC and rhBNP groups following the
treatment (P>0.05; Table
III).
| Table IIISerum BNP levels 4 weeks after
injection (ng/l, mean ± s). |
Table III
Serum BNP levels 4 weeks after
injection (ng/l, mean ± s).
| Group | n | Pre-injection | Post-injection |
|---|
| Normal | 6 | 75.04±7.28 | 72.32±6.54 |
| HF | 6 | 554.15±32.60 | 597.85±35.36 |
| BMSC | 8 | 566.86±19.53 | 376.31±27.21a,b |
| BMSC + rhBNP | 8 | 571.62±13.67 | 343.36±17.26a–c |
| rhBNP | 7 | 563.83±22.49 | 402.71±15.76a,b |
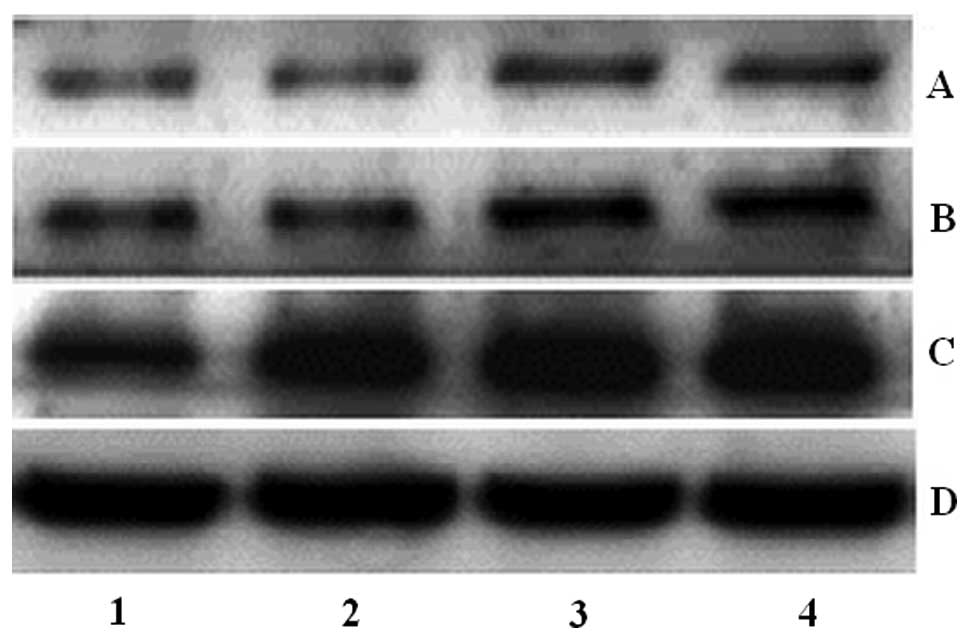
Expression of specific proteins in
myocardial tissue
Following the 4-week treatment, the expression
levels of specific proteins in the myocardial tissue were detected.
The expression levels of GATA-4, cTnI and Cx43 proteins in the BMSC
and the BMSC plus rhBNP groups were increased compared with those
in the HF group (P<0.05). The GATA-4, cTnI, and Cx43 protein
expression levels of the BMSC plus rhBNP group were significantly
higher than those of the BMSC group (P<0.05). In addition, the
GATA-4 expression level in the BMSC group was higher than that in
the rhBNP group (P<0.05; Fig.1).
Discussion
Cardiomyocytes are the most basic structural and
functional units of the heart. The change in cardiac function
caused by heart disease is essentially caused by the
denaturation-induced necrosis of myocardial cells. The traditional
drug treatments that target heart failure only relieve the symptoms
of the disease and do not fundamentally stop the progression of the
disease. For patients with advanced heart failure, heart
transplantation is not always a viable option due to the
limitations in the number of donors and the risk of transplant
rejection. Unlike heart transplantation, the transplantation of
functional myocardial tissues to replace injured myocardial tissues
of the host to recover cardiac function has broader applications.
Therefore, stem cell research to remedy, repair and replace
myocardial cells has become a popular research area in the
cardiovascular field (14–16).
The rhBNP protein itself has no cardiotonic effect,
but it increases the intracellular cyclic GMP (cGMP) concentration,
which promotes the relaxation of smooth muscle cells by interacting
with the guanylate cyclase in vascular smooth muscle cells and
endothelial cells. As a secondary messenger, cGMP dilates arteries
and veins, which reduces the systemic arterial pressure, the right
atrial pressure and the pulmonary capillary wedge pressure,
ultimately reducing the cardiac preload and afterload and improving
heart function. In addition, rhBNP inhibits sodium reabsorption in
the proximal tubules, which generates a natriuretic effect and
further reduces the cardiac preload by enhancing the glomerular
filtration rate (17–19). rhBNP is also an antagonist of the
renin-angiotensin-aldosterone system (RAAS) and it reduces the
excessive activation of renin, aldosterone, endothelin and
vasopressin to relieve their adverse effects (20,21).
rhBNP is involved in the regulation of blood pressure, blood volume
and the water and electrolyte balance. It reduces pulmonary
resistance and the plasma volume, thereby reducing the cardiac
preload and afterload and improving heart function. Considering
that rhBNP has no positive inotropic action, it does not increase
myocardial oxygen consumption.
By contrast, dobutamine increases cardiac
contractility, quickens atrioventricular conduction and reduces
peripheral vascular resistance, mainly through its agonist effect
on β1 receptors, thereby increasing the heart stroke volume and
improving heart function. However, under increased cardiac
contractility, with larger doses of dobutamine or in highly
sensitive patients, the ventricular rate will increase and blood
pressure increases abnormally. These factors increase the
myocardial oxygen consumption, which is detrimental to patients
with acute myocardial infarction.
We selected rats with an LVEF reduced by 20–30% as
the experimental model and we selected echocardiography,
hemodynamics and the serum BNP concentration as indicators of heart
function. The results suggest that BMSC transplantation improves
heart function, but the extent of this improvement is relatively
low. Between the rhBNP and the BMSC treatments for heart failure,
no significant differences were observed in terms of their effect
on heart function. Compared with simple cell transplantation, the
combination of BMSC transplantation and rhBNP therapy clearly
improved heart function.
A question of debate in the field of cell
transplantation research is whether it is possible for transplanted
cells to be induced to differentiate into myocardial cells.
Previous studies have suggested that bone marrow cell
transplantation improves the heart function of the patients with
myocardial infarction and heart failure. However, these conditions
were not improved at the end of the treatment, and its long-term
efficacy is controversial. At present, although a few studies have
indicated that bone marrow cells have the potential to
differentiate into myocardial cells, the consensus on the benefits
of cell transplantation on heart function lies in the promotion of
angiogenesis and resistance to myocardial apoptosis via paracrine
secretion, rather than by their differentiation into myocardial
cells. Based on the present study, following BMSC transplantation,
the myocardial tissues expressed the transcription factor GATA-4,
which is closely related to myocardial cell differentiation. In
addition, the HF model rats that were treated with rhBNP expressed
low levels of GATA-4, which was possibly associated with the
activation and initial division of the cardiac stem cells after
myocardial injury. Following the combined BMSC transplantation and
rhBNP treatment, the GATA-4 expression was significantly higher
than that after BMSC transplantation or rhBNP treatment alone. The
Cx43 and cTnI expression levels were also significantly higher than
those in the other groups. Further studies are required to
determine whether the aforementioned results are associated with
enhanced BMSC differentiation into myocardial cells or the enhanced
survival of BMSCs in the myocardial tissue to function in paracrine
secretion. In addition, whether the combined effect of BMSCs and
rhBNP is simply the sum of two effects or is synergistic should be
determined.
References
|
1
|
Xu XW, Zeng GY, Yang Y and Liu HX:
Recombinant human brain natriuretic peptide on the cardiac
hemodynamics and renal function in dogs with heart failure. Yao Xue
Xue Bao. 37:758–762. 2002.(In Chinese).
|
|
2
|
Iglesias J, Hom D, Antoniotti M, Ayoub S
and Levine JS: Predictors of worsening renal function in adult
patients with congestive heart failure receiving recombinant human
B-type brain natriuretic peptide (nesiritide). Nephrol Dial
Transplant. 21:3458–3465. 2006. View Article : Google Scholar
|
|
3
|
Recombinant Human Brain Natriuretic
Peptide Multicenter Clinical Study Group. Hu DY: Efficacy and
safety of intravenous recombinant human brain natriuretic peptide
in patients with decompensated acute heart failure: a multicenter,
randomized, open label, controlled study. Zhonghua Xin Xue Guan
Bing Za Zhi. 39:305–308. 2011.(In Chinese).
|
|
4
|
Hatzistergos KE, Quevedo H, Oskouei BN, et
al: Bone marrow mesenchymal stem cells stimulate cardiac stem cell
proliferation and differentiation. Circ Res. 107:913–922. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wei H, Tan G, Manasi, et al: One-step
derivation of cardiomyocytes and mesenchymal stem cells from human
pluripotent stem cells. Stem Cell Res. 9:87–100. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gnecchi M, Danieli P and Cervio E:
Mesenchymal stem cell therapy for heart disease. Vascul Pharmacol.
57:48–55. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li XH, Fu YH, Lin QX, et al: Induced bone
marrow mesenchymal stem cells improve cardiac performance of
infarcted rat hearts. Mol Biol Rep. 39:1333–1342. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Vassalli G and Moccetti T: Cardiac repair
with allogeneic mesenchymal stem cells after myocardial infarction.
Swiss Med Wkly. 141:w132092011.PubMed/NCBI
|
|
9
|
Wen Z, Zheng S, Zhou C, Wang J and Wang T:
Repair mechanisms of bone marrow mesenchymal stem cells in
myocardial infarction. J Cell Mol Med. 15:1032–1043. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tokunaga M, Liu ML, Nagai T, et al:
Implantation of cardiac progenitor cells using self-assembling
peptide improves cardiac function after myocardial infarction. J
Mol Cell Cardiol. 49:972–983. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hilfiker A, Kasper C, Hass R and Haverich
A: Mesenchymal stem cells and progenitor cells in connective tissue
engineering and regenerative medicine: is there a future for
transplantation? Langenbecks Arch Surg. 396:489–497. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Menasche P: Cardiac cell therapy: lessons
from clinical trials. J Mol Cell Cardiol. 50:258–265. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Siveski-Iliskovic N, Hill M, Chow DA and
Singal PK: Probucol protects against adriamycin cardiomyopathy
without interfering with its antitumor effect. Circulation.
91:10–15. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Oh Y, Wei H, Ma D, Sun X and Liew R:
Clinical applications of patient-specific induced pluripotent stem
cells in cardiovascular medicine. Heart. 98:443–449. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hoover-Plow J and Gong Y: Challenges for
heart disease stem cell therapy. Vasc Health Risk Manag. 8:99–113.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Arnous S, Mozid A, Martin J and Mathur A:
Bone marrow mononuclear cells and acute myocardial infarction. Stem
Cell Res Ther. 3:22012. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mills RM, LeJemtel TH, Horton DP, et al:
Sustained hemodynamic effects of an infusion of nesiritide (human
b-type natriuretic peptide) in heart failure: a randomized,
double-blind, placebo-controlled clinical trial. Natrecor Study
Group. J Am Coll Cardiol. 34:155–162. 1999. View Article : Google Scholar
|
|
18
|
Bocchi EA, Moura LZ, Issa VS, Cruz F,
Carvalho VO and Guimarães GV: Effects of the recombinant form of
the natural human B-type natriuretic peptide and levosimendan on
pulmonary hyperventilation and chemosensivity in heart failure.
Cardiovasc Ther. Aug 3–2011.(Epub ahead of print). View Article : Google Scholar
|
|
19
|
Iglesias J, Hom D, Antoniotti M, Ayoub S
and Levine JS: Predictors of worsening renal function in adult
patients with congestive heart failure receiving recombinant human
B-type brain natriuretic peptide (nesiritide). Nephrol Dial
Transplant. 21:3458–3465. 2006. View Article : Google Scholar
|
|
20
|
Calderone A, Thaik CM, Takahashi N, Chang
DL and Colucci WS: Nitric oxide, atrial natriuretic peptide, and
cyclic GMP inhibit the growth-promoting effects of norepinephrine
in cardiac myocytes and fibroblasts. J Clin Invest. 101:812–818.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kawakami R, Saito Y, Kishimoto I, et al:
Overexpression of brain natriuretic peptide facilitates neutrophil
infiltration and cardiac matrix metalloproteinase-9 expression
after acute myocardial infarction. Circulation. 110:3306–3312.
2004. View Article : Google Scholar
|