Introduction
Gastric cancer (GC) is the sixth most common cancer
and the fourth leading cause of cancer-related deaths worldwide
(1–3). The incidence of GC, especially in the
Asian region (China, Japan, and Korea), has markedly increased over
the past three decades (4).
Moreover, statistics of cancer research from the International
Agency for Research on Cancer have revealed that the morbidity and
mortality rates associated with GC in China accounted for 42.6 and
45.0% of the global rates in 2015, respectively (5). Consequently, the high incidence of GC
can result in great health and economic burdens (6). The recent development of diagnostic
and surgical techniques has greatly improved the prognosis of GC
patients (7,8). Five-year survival rates for patients
with early GC can reach 90%. Unfortunately, most patients, however,
have already developed advanced GC at the time of diagnosis
(9,10). For patients with advanced GC,
several studies have revealed that the median survival time of
patients with GC was only 6–9 months, with surgical treatment
unable to prolong the patient survival (11,12).
Even with expanded resection, lymph node clearance, and neoadjuvant
chemotherapy, the incidence rates of postoperative local recurrence
and distant metastasis are still high (13). Therefore, considering the high ratio
of early GC patients who are cured, the key to reducing mortality
rates and improving the prognosis for GC patients is early and
accurate diagnosis.
To create a non-invasive, convenient, and low-priced
diagnostic method, circulating biomarker detection methods have
been widely used in clinics. GC serum tumor markers are currently
used in clinical settings for the detection of GC. However, methods
for the detection of carcinoembryonic antigen (CEA), carbohydrate
antigen 199 (CA199), and carbohydrate antigen 724 (CA724) lack
adequate sensitivity and specificity, which has precluded their
widespread application in early diagnosis of GC (14). Therefore, it is necessary to
investigate other potential biomarkers useful in identifying GC
with high sensitivity and specificity. Recently, many researchers
have been attracted to microRNAs (miRNAs) which have been stably
detected in cell-free body fluids, such as plasma or serum. These
miRNAs are called circulating miRNAs and are protected from
degradation by ribonucleases in the blood. Additionally, the
expression profile of miRNAs in GC patients usually exhibits
exceptionally high expression of miRNAs in contrast to that in
normal specimens (15).
miRNAs are a small, single-stranded non-coding RNAs
that can regulate the expression of thousands of genes by
inhibiting and degrading mRNAs during the translation process
(16,17). miRNAs regulate various
pathophysiological processes that involve cell proliferation,
apoptosis, and differentiation. They also play an important role in
tumorigenesis, especially neoplasm development, metastasis,
angiogenesis, and immune responses (18).
Circulating miRNAs are considered to be novel
potential biomarkers in the detection of many diseases, which were
first demonstrated by Mitchell et al (19) for the detection of cancer.
Subsequently, their roles have been demonstrated in numerous
studies. Nevertheless, it is difficult to specify a suitable miRNA,
and the results of miRNA expression analysis are inconsistent.
Despite a large number of studies on circulating miRNAs, few
relevant measures have been applied in the clinical setting. In the
present study, in this meta-analysis, we systematically and
comprehensively analyzed the diagnostic accuracy of circulating
miRNAs in distinguishing gastric cancer patients from the
significant heterogeneity of other factors.
Materials and methods
Literature search
Two authors independently searched online databases,
PubMed, Embase, the Cochrane Library, Web of Science, and Springer
to identify potentially eligible studies published before November
10, 2017. The keywords used for literature retrieval were
(‘microRNA’ or ‘miRNA’ or ‘miR’) and (‘gastric cancer’ or ‘gastric
carcinoma’ or ‘gastric tumor’ or ‘gastric neoplasm’) and
(‘diagnostic’ or ‘diagnosis’ or ‘sensitivity and specificity’ or
‘ROC curve’) and (‘circulating’ or ‘plasma’ or ‘serum’ or ‘blood’).
The citations in identified articles and in review articles were
also examined. All publications identified by our search strategy
were independently assessed by four reviewers. Any disagreement on
a controversial study was resolved by discussion to consensus.
Literature selection
Eligible studies included in the present
meta-analysis met the following criteria: i) the diagnosis of GC
was made based on histopathological confirmation; ii) miRNA
concentration in plasma, serum, or blood was detected before the
patient received any treatment; iii) the study explored the
correlation between miRNA expression levels and gastric cancer
diagnosis; iv) the study included standard references for the GC
diagnosis, including patients with benign diseases or healthy
individuals as the control groups; and v) the study provided
adequate or sufficient data for the calculation of 2×2 tables
consisting of true positive (TP), false positive (FP), true
negative (TN), and false negative (FN). In addition, exclusion
criteria were: i) publications irrelevant to the detection values
of circulating miRNAs for GCs; ii) review studies, editorials, case
reports, and letters; iii) duplicate publications; and iv)
unqualified data. All literature that satisfied the above criteria
constituted qualified studies.
Data extraction and quality
assessment
The following data characteristics were extracted
for each eligible study by two reviewers (HW and KP),
independently: i) basic characteristics of the included studies,
including the first author, year of publication, country of
publication, origin of the study population, sample type, study
design, sample size, number of participants, and variables adjusted
for the analysis, and ii) for diagnostic studies, the sensitivity,
specificity, TP, FP, FN, and TN values of the diagnostic test
results were considered.
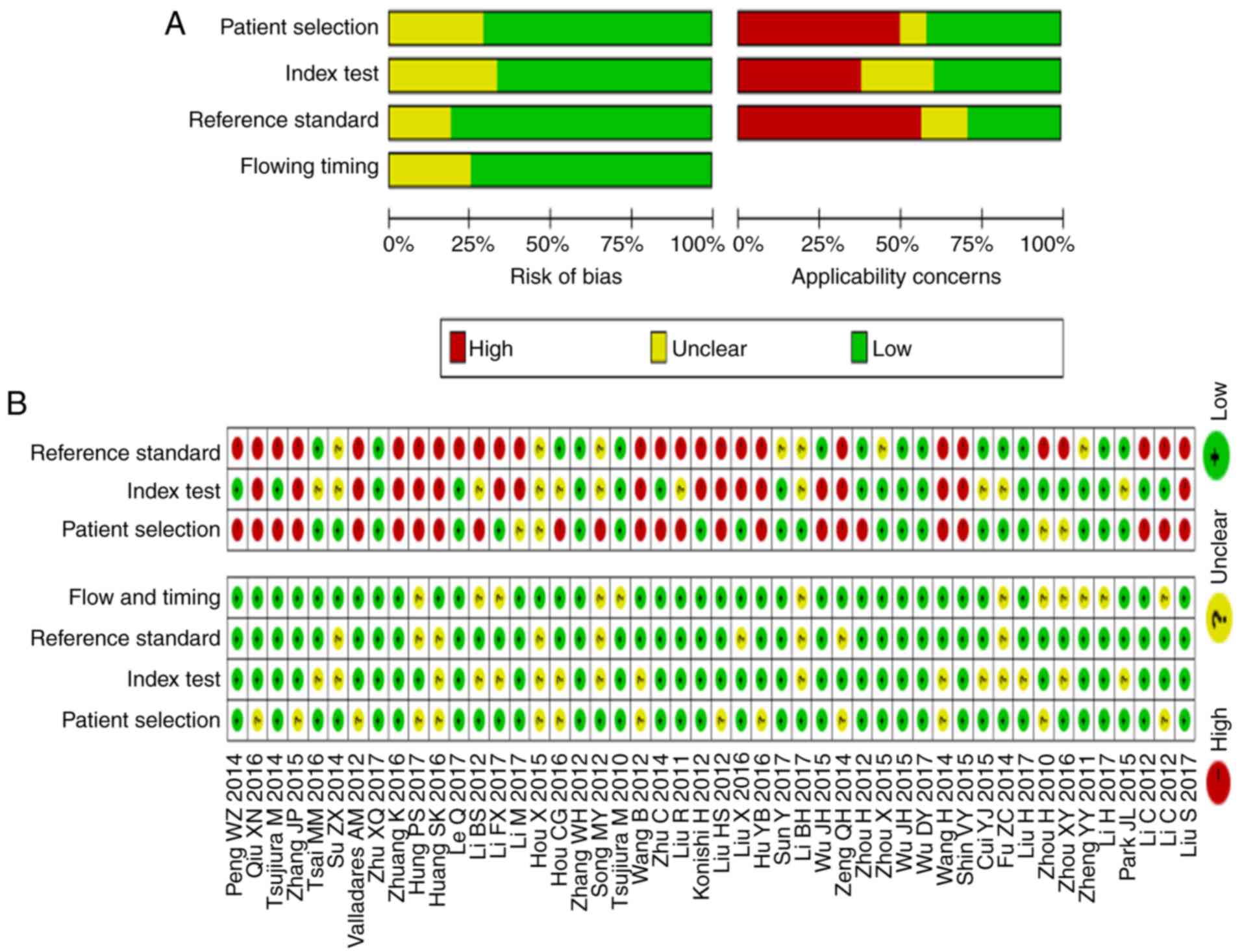
The quality assessment of the studies included in
the present study was performed by two authors independently using
the Quality Assessment of Diagnostic Accuracy studies (QUADAS-2)
(20) checklist in Rev Man 5.0
software (http://ims.cochrane.org/revman/download). This scale
was composed of four domains consisting of patient selection, index
test, reference standard, and flow and timing domain. Each
signaling question was judged as ‘yes’, ‘no’, or ‘unclear’ and each
study's risk of bias and concern for applicability was estimated as
‘high’, ‘low’, or ‘unclear’ except for the flow and timing domain,
for which the applicability concern did not apply. An answer of
‘yes’ meant that the risk of bias could be judged as being low,
whereas an answer of ‘no’ or ‘unclear’ meant that the risk of bias
could be judged as being high. A third reviewer was consulted in
the case of conflict and inconsistency was dealt with by a
multilateral argument.
Statistical methods
To evaluate the diagnostic accuracy of miRNA assays
for detecting GC, the sensitivity and specificity parameters were
extracted from each study and the number of patients with TP, FP,
TN, and FN results from each included article were extracted or
calculated. Based on the 2×2 tables, meta-analyses were performed
with Meta-Disc software version 1.4 (http://www.hrc.es/investigacion/metadisc_en.htm.)
and STATA software version 12.0 (Stata Corporation, College
Station, TX, USA) to evaluate the pooled statistics (95% CI) of
sensitivity, specificity, positive and negative likelihood ratios
(PLR and NLR) [PLR = sensitivity/(1 - specificity), NLR = (1 -
sensitivity)/specificity], diagnostic odds ratio (DOR), and area
under the summary receiver operating characteristic curves
(AUSROC), with standard errors (SE) and Q index with SE for the
test's performance using miRNA for GC detection. If sufficient
information was not available, we recalculated these values on the
basis of the sensitivity and specificity offered. Summary
statistics revealed the diagnostic threshold effects that were
analyzed by Spearman's correlation coefficient and P-value. If
there was no significant threshold effect, the diagnostic accuracy
was estimated by pooled statistics, whereas the diagnostic accuracy
was evaluated only by AUSROC and Q indices rather than
sensitivities, specificities, PLR, NLR, and DOR.
Positive and negative likelihood ratios describe the
discriminatory properties of positive and negative test results,
respectively (21). Likelihood
ratios state how many times more likely particular test results are
in patients with disease than in those without disease (22). Positive likelihood ratios above 10
and negative likelihood ratios below 0.1 have been noted as
providing convincing diagnostic evidence, whereas PLR>5.0 and
NLR<0.2 imply higher diagnostic evidence (23). DOR represented the positive odds of
aberrant miRNA expression in patients with GC compared to the
probability of the healthy control. AUSROC values of 0.5–0.7,
0.7–0.9, and 0.9–1.0 were applied to indicate low, moderate, and
high diagnostic accuracy, respectively. A smaller Q index indicated
a lower diagnostic accuracy.
Heterogeneity was determined by Cochran's Q
statistic based on the Chi-square test and I2
statistics. I2 values of 0–40, 40–70, and 70–100%
indicated low, moderate, and high variance, respectively (24). If moderate heterogeneity existed or
different clinical characteristics were noted, the DerSimonian and
Laird random-effects model was applied. Considerable heterogeneity
was considered if I2>50% and/or P<0.05 (25,26).
Sources of heterogeneity were explored by meta-regression analysis
based on possible characteristics and a subsequent subgroup
analysis was performed to identify potential covariates.
Furthermore, subgroup and meta-regression analyses were performed
to detect the extent of heterogeneity between studies. Publication
bias was checked using Deeks' funnel plot analysis (24). All of the aforementioned statistical
calculations were made with Meta-DiSc and STATA 12.0 software.
Results
Literature search
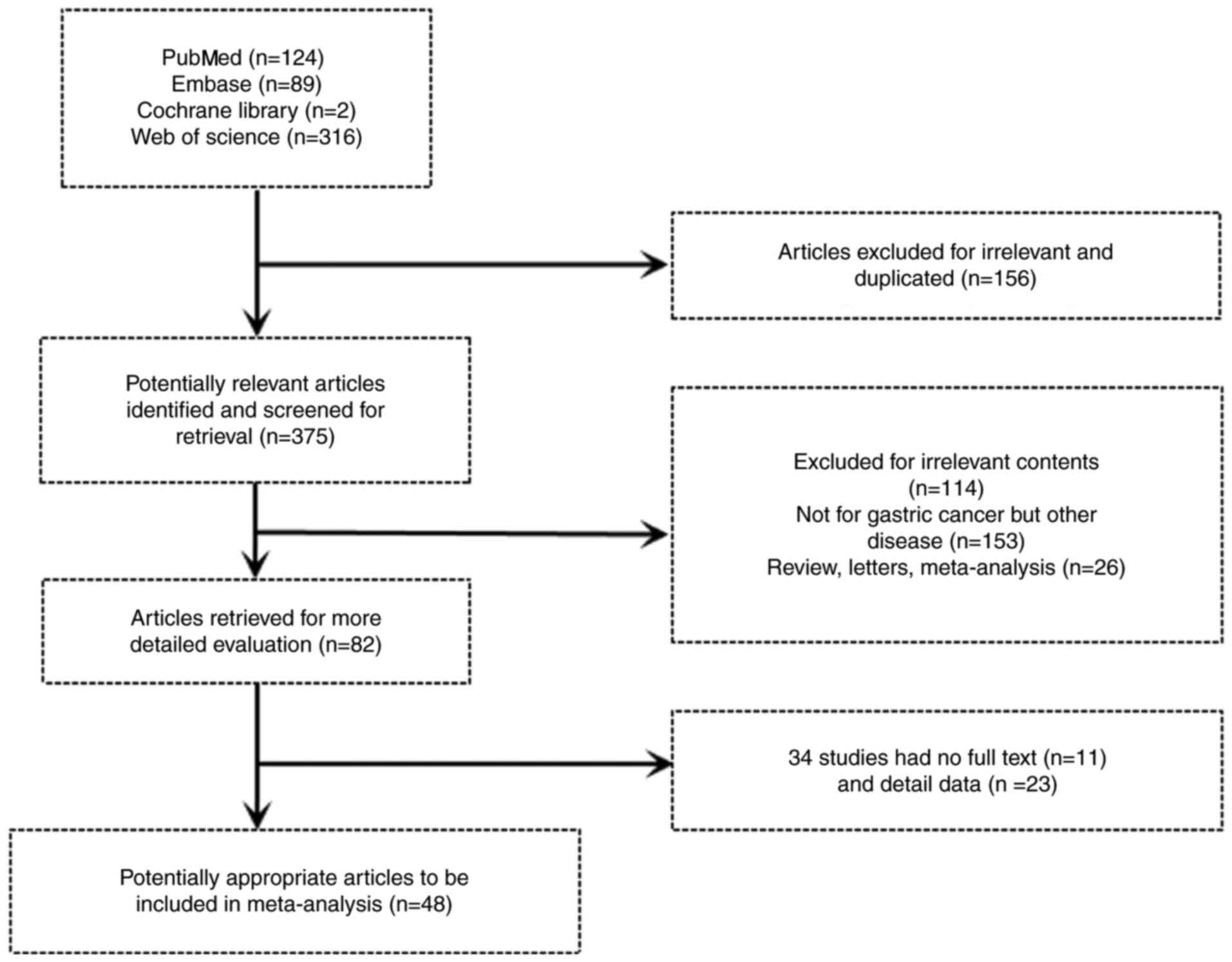
In Fig. 1, the
flowchart for the selection of included articles is presented.
Searching Pubmed, Embase, the Cochrane library, and Web of Science
resulted in the inclusion of 531 articles. After a review of titles
and abstracts, 156 publications were found to be irrelevant or
duplicated. Next, we, intensively read the remaining studies,
whereby 114 of these publications were removed for irrelevant
content, 153 articles were eliminated owing to the study being
unrelated to gastric cancer, and 26 studies were not considered as
they were review letters and meta-analyses. After a more detailed
evaluation, 34 studies were removed as they did not contain full
text or had insufficient data for extraction. Finally, the
selection process revealed 48 studies that were eligible for
diagnostic analysis.
Study characteristics and quality
assessment
The main characteristics of the 48 qualified
articles included 77 microRNAs, of which one study was performed in
Europe and 47 studies were undertaken in Asia. The evaluated
studies included a total of 3,829 cases and 3,175 controls for the
present meta-analysis. These are presented in Table I. In the tumor-node-metastasis (TNM)
classification, 20 articles included patients in stages I–IV. The
other 13 included patients in stages I–II, of which only one study
involved patients in stage I, whereas the remainder of the eligible
studies (n=15) did not mention the TNM stage. Analysis of data from
the nine included studies that used miRNA microarray chips and
revealed a number of miRNAs with altered expression, where
candidate miRNAs were chosen via the training and validation
design, whereas candidate miRNAs from the remaining articles (n=39)
were chosen directly without microchip procession. Meanwhile, 42 of
the 48 studies investigated the diagnostic value of a single miRNA
used in GC detection, while only nine researched a set of miRNAs.
Of the selected miRNAs, three were from the single miRNA studies.
In terms of samples, circulating miRNAs from GC and healthy
individuals were classified as serum (n=17), plasma (n=25), and
peripheral blood (n=6). We also summarized miRNAs whose expression
was upregulated in 33 studies and downregulated in 15 studies. One
study (8) was excluded due to the
unclear description about miRNA regulation, while another study
(38) involved both upreguated and
downregulated miRNAs. In particular, the expression of 58 miRNAs,
including miR-21, was most frequently upregulated and that of 18
miRNAs (miR-26a and miR-199) was downregulated.
 | Table I.Descriptive characteristics of the
eligible studies. |
Table I.
Descriptive characteristics of the
eligible studies.
|
|
|
| Case/control |
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|---|
| Author | Year | Region | Sample size
(n) | Mean age
(case/control) (year) | Male ratio
(case/control) (%) | Sample/methods | miRNA
profiling | Patients TNM
(I/II/III/IV) | (Refs.) |
|---|
| Peng WZ | 2014 | China | 57/58 | NM | NM | Serum/qRT-PCR | miR-191 | NM | (27) |
| Qiu X | 2016 | China | 280/280 | 63.3/63.2 | 63.2/63.2 | Plasma/qRT-PCR | miR-26a | 65/61/135/16/3
(I/II/III/IV/missing) | (28) |
| Tsujiura M | 2015 | Japan | 104/65 | NM | NM | Plasma/qRT-PCR | miR-18a | 66/14/15/9 | (29) |
| Zhang J | 2015 | China | 155/111 | 56.6/47.4 | 71/63 | Plasma/qRT-PCR | miR-16-5p,
19b-3p | 33/26/59/25/12
(I/II/III/IV/unknown) | (30) |
| Tsai MM | 2016 | Taiwan | 98/126 | 64.1/66.4 | 58.2/47.6 | Plasma/qRT-PCR | miR-196a, 196b, and
both | 30/12/38/18 | (31) |
| Su ZX | 2014 | China | 82/65 | 69.0/71.2 | 58.5/60.0 | Plasma/qRT-PCR | miR-18a | NM | (32) |
| Valladares-Ayerbes
M | 2012 | Spain | 52/15 | 65.9/65.3 | 81/80 | Blood/qRT-PCR | miR-200c | 9/12/31
(I–II/III/IV) | (33) |
| Zhu X | 2017 | China | 114/95 | NM | 62.0/64.1 | Serum/qRT-PCR | miR-145 | 35/79
(I+II/III+IV) | (34) |
| Zhuang K | 2016 | China | 138/50 | NM | 61.6/NM | Plasma/qRT-PCR | miR-23b | NM | (35) |
| Hung PS | 2017 | Taiwan | 65/108 | 67.7/56.1 | 72.3/62.0 | Plasma/qRT-PCR | miR-376c | 30/14/16/5 | (36) |
| Huang S | 2016 | China | 62/59 | 58/57 | NM | Serum/qRT-PCR | miR-21, 31, 92a,
181b, 203 | NM | (8) |
| Le Q | 2017 | China | 41/41 | NM | 58.5/53.7 | Blood/qRT-PCR | miR-25 | NM | (37) |
| Li BS | 2012 | China | 70/70 | NM | 70/63 | Plasma/qRT-PCR | miR-223, 21,
218 | 12/11/36/11 | (38) |
| Li F | 2017 | China | 65/65 | 54.1/56.2 | 76.92/76.92 | Plasma/RT-PCR | miR-106b, 93,
25 | 29/36
(I+II/III+IV) | (39) |
| Li M | 2017 | China | 51/51 | NM | 62.7/NM | Plasma/qRT-PCR | miR-200c | NM | (40) |
| Hou X | 2015 | China | 80/80 | 68.0/67.0 | 57.5/55 | Plasma/qRT-PCR | miR-106a | 45/35
(I+II/III+IV) | (41) |
| Hou CG | 2016 | China | 150/150 | NM | 65.33/NM | Serum/qRT-PCR | miR-206 | 57/93
(I+II/III+IV) | (42) |
| Zhang WH | 2012 | China | 20/20 | 60.9/NM | 75/NM | Serum/qRT-PCR | miR-375 | 1/1/1/6/4/7
(Ib/II/IIIa/IIIb/IV/unknown) | (43) |
| Song MY | 2012 | China | 68/68 | NM | NM | Serum/qRT-PCR | miR-221, 376c,
744 | NM | (44) |
| Tsujiura M | 2010 | Japan | 69/30 | NM | NM | Plasma/qRT-PCR |
miR-106a/let-7a | 38/13/14/4 | (45) |
| Wang B | 2012 | China | 30/39 | 58.0/46.0 | 73.3/23.1 | Serum/qRT-PCR | miR-21 | 11/19
(I+II/III+IV) | (46) |
| Zhu C | 2014 | China | 48/102 | 56.6/54.0 | 72.9/70.6 | Plasma/qRT-PCR | miR-16, 25, 92a,
451, 486-5p, and combination |
|
|
| Liu R | 2011 | China | 82/64 | 60.2/60.0 | 84.0/78.0 | Serum/qRT-PCR | Combined (miR-1,
20a, 27a, 34a, 423-5p) | 29/56/48/23/8
(I/II/III/IV/unknown) | (48) |
| Konishi H | 2012 | Japan | 56/30 | NM | NM | Plasma/qRT-PCR | miR-451, 486 | NM | (49) |
| Liu H | 2012 | China | 40/41 | 56.0/58.0 | 65.6/65.6 | Plasma/qRT-PCR | miR-378 | 4/12/11/13 | (50) |
| Liu X | 2016 | Hong Kong | 80/70 | 67.0/56.0 | 66.9/59.0 | Plasma/qRT-PCR | miR-940 | 20/10/28/22 | (51) |
| Hu Y | 2016 | China | 137/79 | NM | 53.3/NM | Serum/qRT-PCR | miR-133a | 58/79
(I+II/III+IV) | (52) |
| Sun Y | 2017 | China | 76/26 | NM | 96.7/61.5 | Serum/qRT-PCR | miR-183 | 15/10/30/21 | (53) |
| Li B | 2017 | China | 116/85 | NM | 66.38/NM | Plasma/qRT-PCR | miR-320 | 68/48
(I+II/III+IV) | (54) |
| Wu J | 2015 | China | 90/90 | NM | 48.9/NM | Serum and
PBMCs/qRT-PCR | miR-421 | 32/21/9/28 | (55) |
| Zeng Q | 2014 | China | 40/36 | NM | 70/NM | Serum/qRT-PCR | miR-17, 106b and
both | 9/31
(I/II)/(III/IV) | (56) |
| Zhou H | 2012 | China | 40/17 | NM | 75/NM | Blood/qRT-PCR | miR-421 | 8/13/4/5/10
(I/II/III/IV/unknown) | (57) |
| Zhou X | 2015 | China | 32/18 | NM | 65.6/61.1 | Plasma/qRT-PCR | Multiple (miR-185,
20a, 210, 25, 92b) | 6/5/17/4 | (58) |
| Wu J | 2015 | China | 50/50 | NM | 48/NM | Serum and
PBMCs/qRT-PCR | miR-21 | 9/11/10/18/2
(I/II/III/IV/unknown) | (59) |
| Wu D | 2017 | China | 32/32 | NM | NM | Serum
samples/qRT-PCR | miR-503 | NM | (60) |
| Wang H | 2014 | China | 50/47 | NM | 54/NM | Serum/qRT-PCR | miR-223, 16,
100 | 31/19
(I+II/III+IV) | (61) |
| Shin VY | 2015 | Hong Kong | 108/96 | NM | NM | Plasma/qRT-PCR | Multiple (miR-627,
629, 652) | 16/13/41/38 | (62) |
| Cui YJ | 2015 | China | 46/40 | NM | 67.4/55 | Plasma/RFQ-PCR | miR-27b-3p | 8/15/12/11 | (63) |
| Fu Z | 2014 | China | 114/56 | NM | 47.36/NM | Plasma/qRT-PCR | miR-222 | 17/25/34/38 | (64) |
| Liu H | 2017 | China | 137/145 | 54.3/53.6 | 62/64.1 | Plasma/qRT-PCR | miR-217 | 43/94
(I+II/III+IV) | (65) |
| Zhou H | 2010 | China | 41/27 | NM | NM | PMNCs/qRT-PCR | miR-106a, 17,
both | NM | (66) |
| Zhou X | 2016 | China | 45/45 | NM | NM | Serum/qRT-PCR | miR-223 | NM | (67) |
| Zheng Y | 2011 | China | 52/20 | NM | NM | Blood/qRT-PCR | miR-21 | NM | (68) |
| Li H | 2017 | China | 75/38 | NM | NM | Blood/qRT-PCR | miR-17-3p, 17-5p,
18a-5p, 19a-3p, 20a-5p, 92a-3p | NM | (69) |
| Park JL | 2015 | Korea | 35/35 | 51.8/48.9 | 51.4/51.4 | Plasma/qRT-PCR | miR-27a | NM | (70) |
| Li C | 2013 | China | 80/70 | 56.7/58.9 | 68.8/64.3 | Plasma/qRT-PCR | miR-199a-3p | 69/7/4
(Ia/Ib/IIa) | (71) |
| Li C | 2013 | China | 180/130 | 58.1/58.9 | 68.9/65.4 | Plasma/qRT-PCR | miR-199a-3p | 40/29/93/18 | (72) |
| Liu S | 2017 | China | 96/40 | NM | NM | Serum/qRT-PCR | miR-144 | 47/49
(I+II/III+IV) | (73) |
The quality of the eligible studies which were
assessed, based on the QUADAS-2 criteria, was independently
appraised by reviewers and is reported in Fig. 2A and B. In total, only five studies
were valued as being low risk for bias and applicability concerns.
The remaining studies were estimated as suboptimal for unclear risk
in areas including index test, reference standard, flow, and
timing. Most of the studies were identified as having a potential
bias risk for patient selection and reference standard.
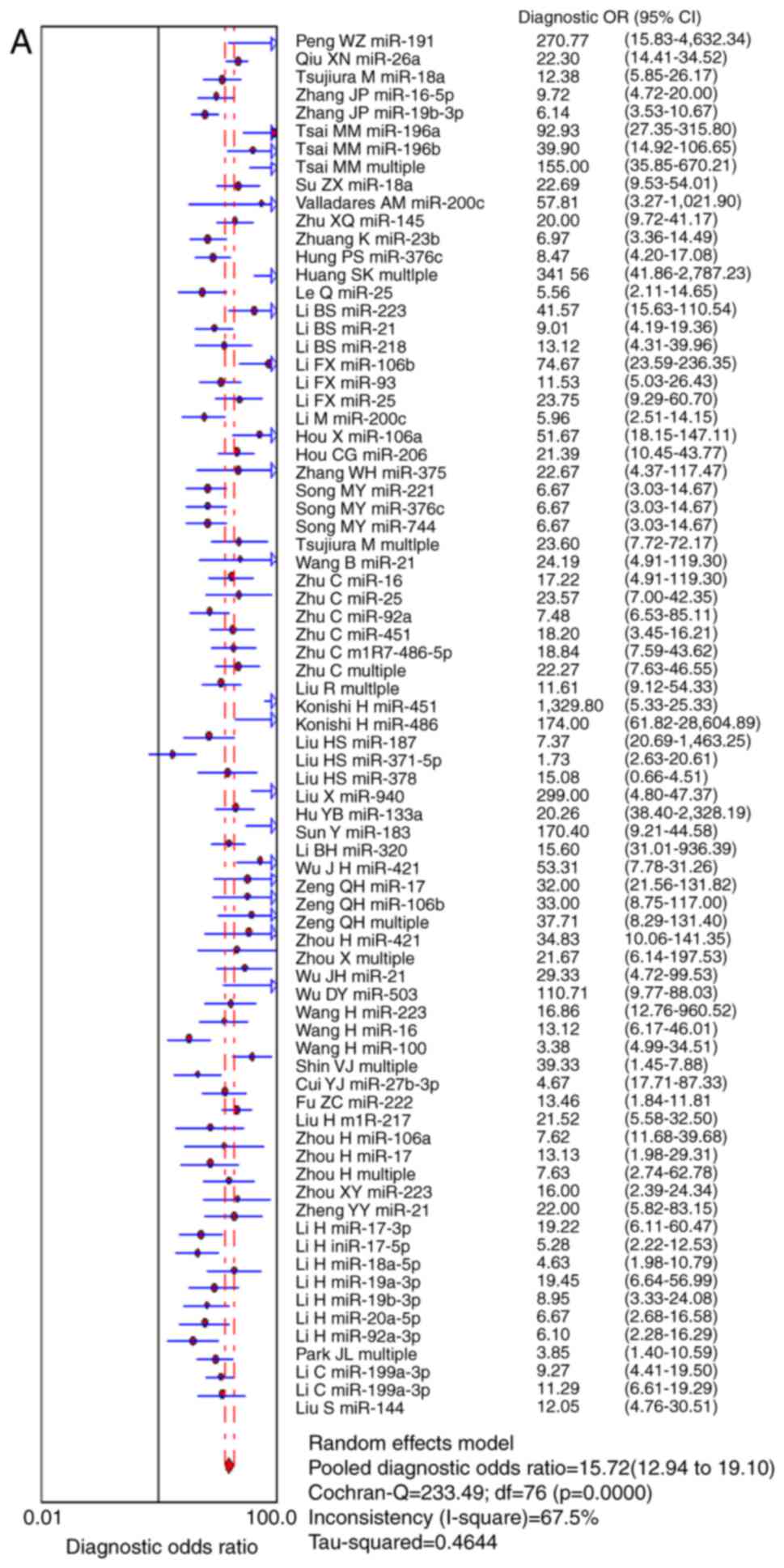
Diagnostic accuracy of circulating
miRNA in GC
First, Meta-DiSc software version 1.4 was used to
analyze the data. The heterogeneity test found that Q test and
I2 values of DOR were 233.49 and 67.5%, respectively
(P=0.0000) (Fig. 3A). Next, we
generated forest plots of sensitivity and specificity, both of
which did not display a straight line distribution and the
Cochran-Q values were 369.52 and 555.63 (Fig. 3B and C), respectively, which
reflected substantial heterogeneity (79.4 and 86.3%, respectively)
among these studies. Random-effects models were then selected to
re-analyze the data and the diagnostic threshold was analyzed. The
Spearman's correlation coefficient was 0.253 (P=0.026),
illustrating that the significant heterogeneity was partially
caused by the diagnostic threshold. In addition, this may be caused
by discrepancies in the study approaches, specimen type, endogenous
reference, or total sample size. Thus, we could not calculate the
statistical outcomes indirectly by neglecting the different factors
and owing to the high heterogeneity. The data could not simply be
pooled and was only suitable for subgroup analyses for illustrating
heterogeneity.
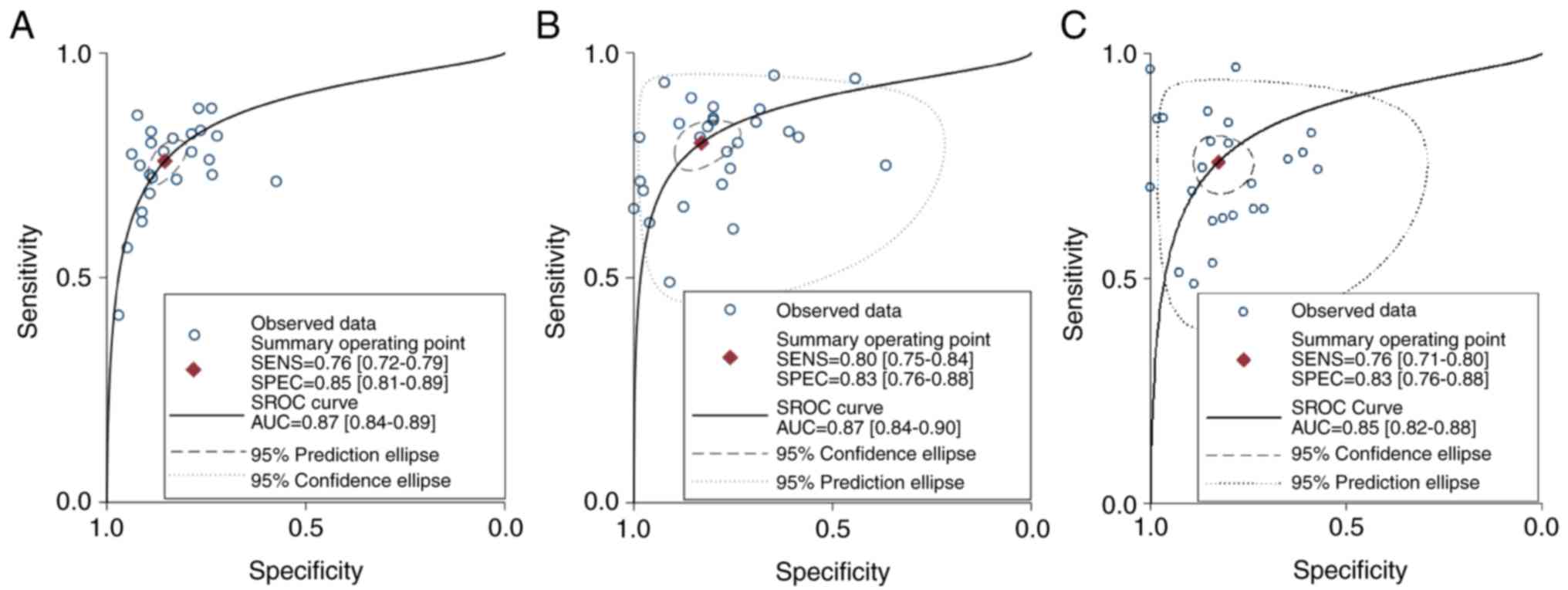
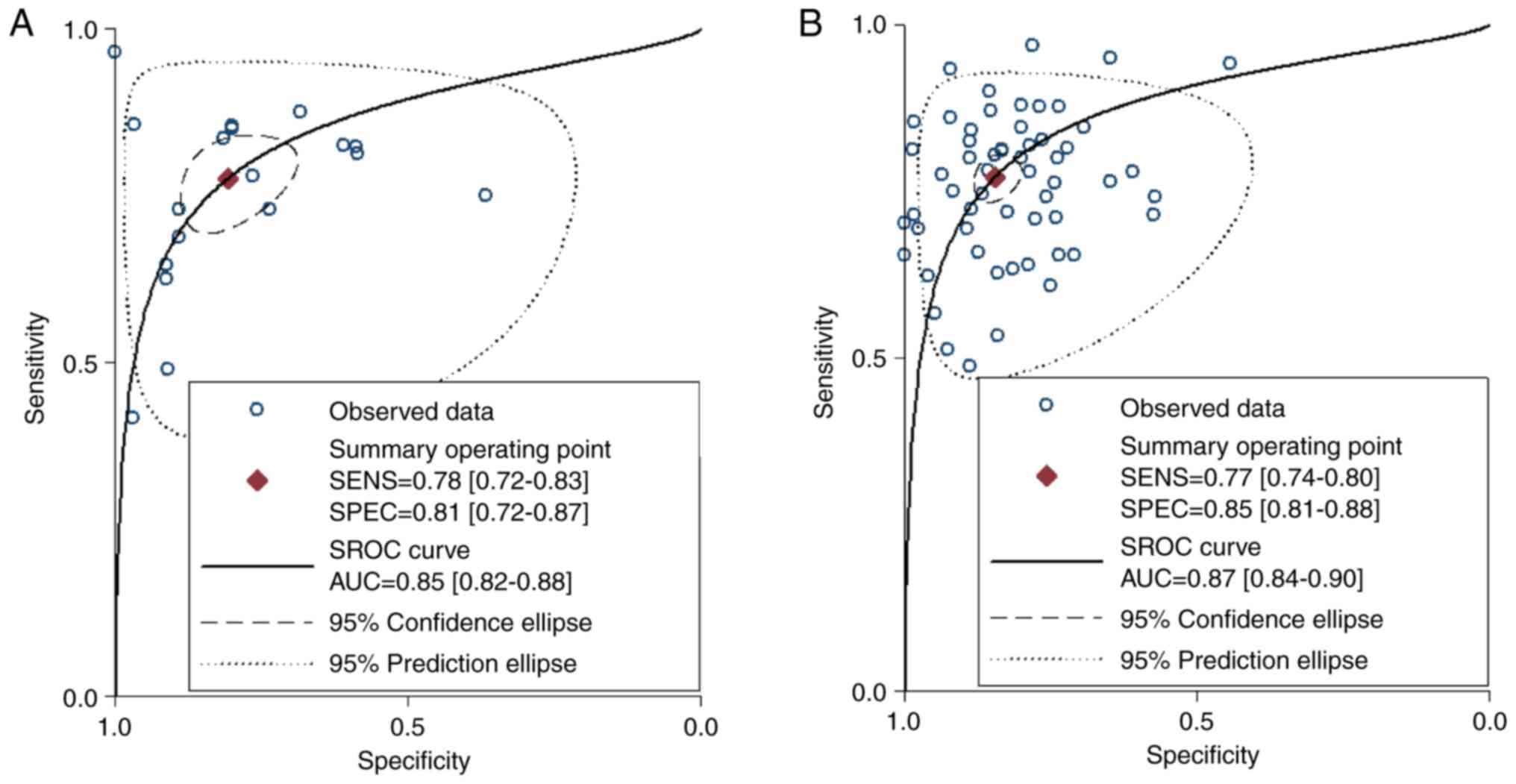
Covariates and subgroup analysis
After stratification in accordance with the five
pre-specified covariates, including patients' stage of GC (early
TNM stage I–II vs. all TNM stages I–IV), miRNA profiling (single
miRNA vs. multiple miRNAs), specimen types (plasma vs. serum vs.
blood), miRNA screening approaches (microarray processing vs
non-microarray processing), and aberrant expression (upregulation
vs. down-regulation). we next assessed their impact on sensitivity
or/and specificity as shown in Table
II and Fig. 4. Comparing
different TNM stages of GC patients with altered expression of
circulating miRNAs, the results revealed that the diagnostic
accuracy of miRNA detection during early stages I–II (sensitivity,
0.76; specificity, 0.85; PLR, 5.20; NLR, 0.28; DOR, 17.63; and AUC,
0.87) was similar to that during all stages I–IV (sensitivity,
0.80; specificity, 0.83; PLR, 4.70; NLR, 0.24; DOR, 18.01; and AUC,
0.87) and non-description stages (sensitivity, 0.76; specificity,
0.83; PLR, 4.40; NLR, 0.29; DOR, 12.18; and AUC, 0.85) with respect
to all parameters except for the slight disparity in DOR. These
results indicated that these biomarkers could not differentiate
early GC from other later TNM stages in accordance with the
diagnostic value.
| Table II.Summary estimates of diagnostic
criteria and their 95% confidence intervals. |
Table II.
Summary estimates of diagnostic
criteria and their 95% confidence intervals.
| Subgroup | N (miR) | SEN (95% CI) | SPE (95% CI) | PLR (95% CI) | NLR (95% CI) | DOR (95% CI) | I2
(%) | AUC (95% CI) |
|---|
| TNM stage |
| TNM
(I–II) | 24 | 0.76
(0.72–0.79) | 0.85
(0.81–0.89) | 5.20
(4.16–6.52) | 0.28
(0.25–0.32) | 17.63
(13.82–22.48) | 41.2 | 0.87
(0.84–0.89) |
| TNM
(I–IV) | 27 | 0.80
(0.75–0.84) | 0.83
(0.76–0.88) | 4.70
(3.32–6.66) | 0.24
(0.20–0.29) | 18.01
(12.56–25.81) | 74.5 | 0.87
(0.84–0.90) |
|
Unclassified TNM stage | 26 | 0.76
(0.71–0.80) | 0.83
(0.76–0.88) | 4.40
(3.12–6.21) | 0.29
(0.24–0.36) | 12.18
(8.40–17.68) | 67.5 | 0.85
(0.82–0.88) |
| miRNA
screening |
|
Mircroarray | 20 | 0.78
(0.72–0.83) | 0.81
(0.72–0.87) | 4.04
(2.81–5.80) | 0.28
(0.22–0.35) | 12.35
(8.63–17.68) | 68.7 | 0.85
(0.82–0.88) |
|
Unrelated microarray | 57 | 0.77
(0.74–0.80) | 0.85
(0.81–0.88) | 5.01
(4.11–6.12) | 0.27
(0.24–0.30) | 17.20
(13.66–21.64) | 66.7 | 0.87
(0.84–0.90) |
| miRNA expression
profiling |
| Single
miR | 68 | 0.77
(0.74–0.80) | 0.84
(0.80–0.87) | 4.69
(3.87–5.67) | 0.28
(0.25–0.31) | 17.00
(13.39–21.56) | 67.2 | 0.86
(0.83–0.89) |
|
Multiple miRs | 9 | 0.80
(0.75–0.84) | 0.85
(0.76–0.90) | 5.21
(3.22–8.43) | 0.23
(0.18–0.31) | 22.22
(11.03–44.77) | 68.2 | 0.87
(0.84–0.90) |
| Sample type |
|
Serum | 23 | 0.81
(0.78–0.84) | 0.83
(0.77–0.88) | 4.89
(3.55–6.72) | 0.23
(0.19–0.27) | 19.44
(13.33–28.36) | 65.8 | 0.88
(0.85–0.90) |
|
Plasma | 40 | 0.78
(0.74–0.81) | 0.84
(0.79–0.88) | 4.90
(3.74–6.43) | 0.27
(0.23–0.31) | 16.47
(12.62–21.49) | 72.2 | 0.86
(0.83–0.89) |
|
Peripheral blood | 14 | 0.68
(0.61–0.74) | 0.81
(0.75–0.86) | 3.62
(2.81–4.65) | 0.39
(0.33–0.47) | 8.82
(6.36–12.24) | 15.6 | 0.82
(0.79–0.85) |
| Altered
miRNAa |
|
Upregulation | 58 | 0.76
(0.73–0.79) | 0.84
(0.80–0.87) | 4.75
(3.84–5.88) | 0.28
(0.25–0.32) | 15.18
(11.98–19.25) | 68.3 | 0.86
(0.82–0.89) |
|
Downregulation | 18 | 0.80
(0.75–0.84) | 0.81
(0.75–0.82) | 4.25
(3.22–5.61) | 0.25
(0.20–0.31) | 15.93
(11.61–21.86) | 59.8 | 0.87
(0.84–0.90) |
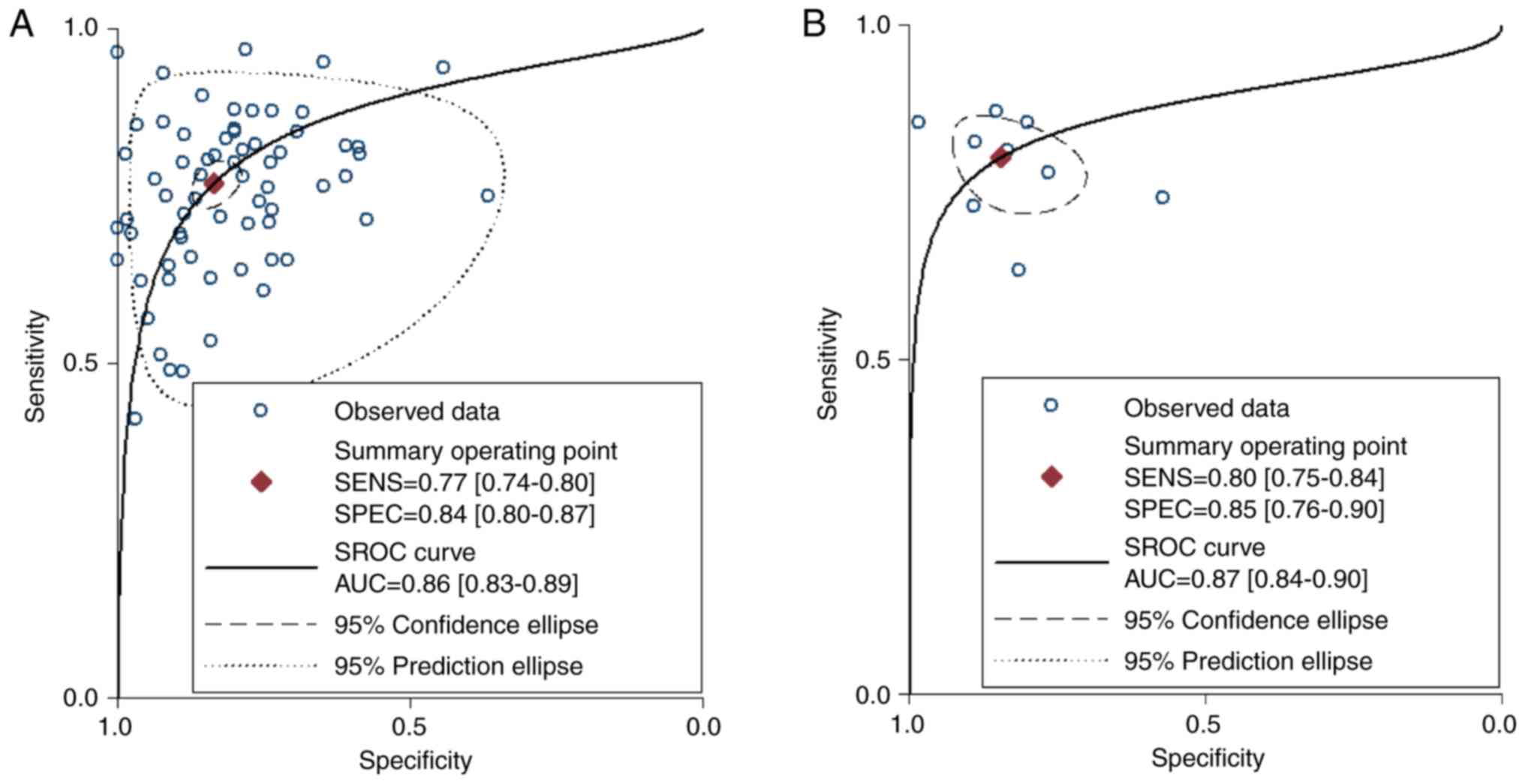
Subsequently, we focused on the different screening
approaches, such as microarray processing vs. non-microarray
processing, and applied these approaches to candidate miRNAs. The
differences between the pooled estimates of DOR (Table II) between miRNAs originating from
microarray and miRNAs selected directly implied that the diagnostic
ability of the former was inferior to the latter. The AUSROC
(Fig. 5) indicated that the
diagnostic accuracy of miRNAs in microarray screening was slightly
less than the non-microarray selection group. In addition, we
conducted subgroup analyses based on miRNA profiling, including
single miRNA and multiple miRNAs. In the subgroup analysis
(Table II and Fig. 6), compared to that of single miRNA,
the diagnostic ability of multiple miRNAs was better, with the
sensitivity increasing from 0.77 to 0.80 and the specificity
increasing from 0.84 to 0.85. AUC varied from 0.86 to 0.87 and the
DOR value markedly increased from 17.00 to 22.22, whereas AUROC
implied that there were parallel diagnostic accuracies between
both.
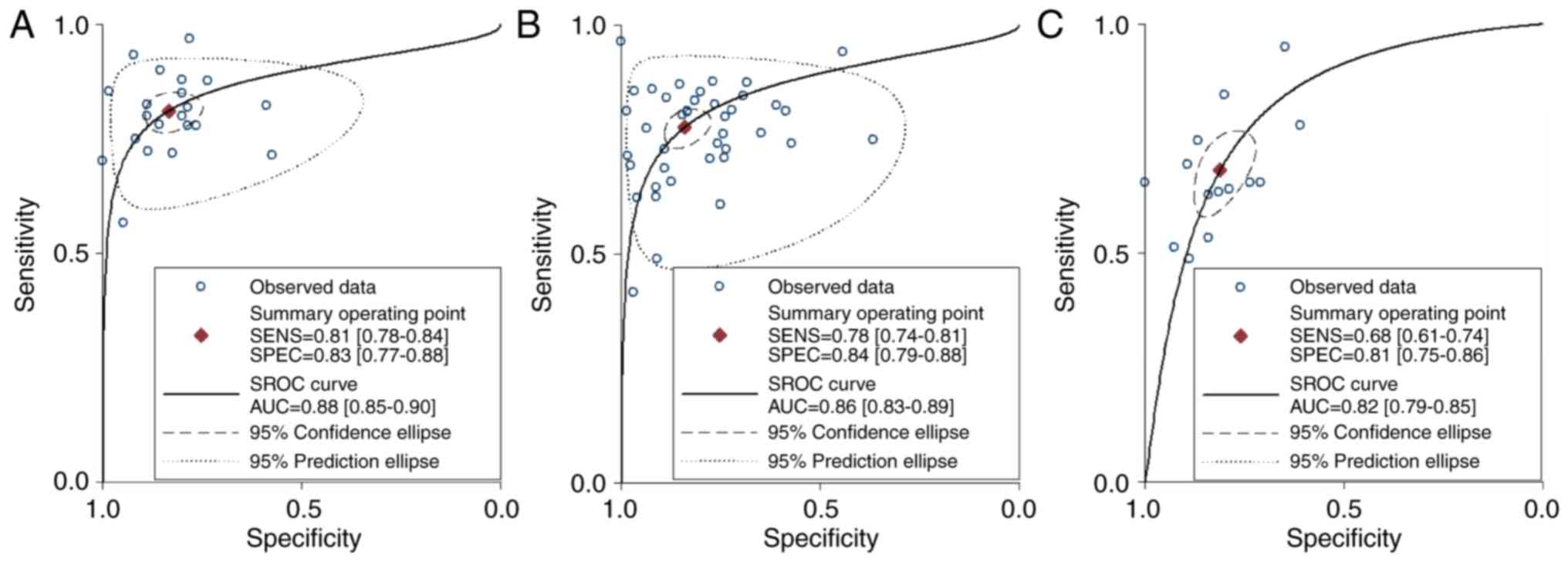
Subgroup analysis of specimen types and aberrant
expression were conducted to identify whether the candidate miRNAs
could clearly discriminate GC sufficient diagnostic performance and
accuracy. In the specimen type subgroup revealed in Table II and Fig. 7, the diagnostic sensitivity of
miRNAs extracted from serum was 0.81 and the specificity was 0.83,
with a pooled DOR of 19.44 and AUC of 0.88. The sensitivity and
specificity of miRNAs from plasma-based studies were 0.78 and 0.84,
respectively, with a summary DOR of 16.47 and AUC of 0.86. However,
for the peripheral blood assay, sensitivity and specificity were
0.68 and 0.81, respectively, with a pooled DOR of 8.82 and AUC of
0.82, which indicated that the serum-based miRNA detection had a
higher diagnostic value for GC than either the plasma or the
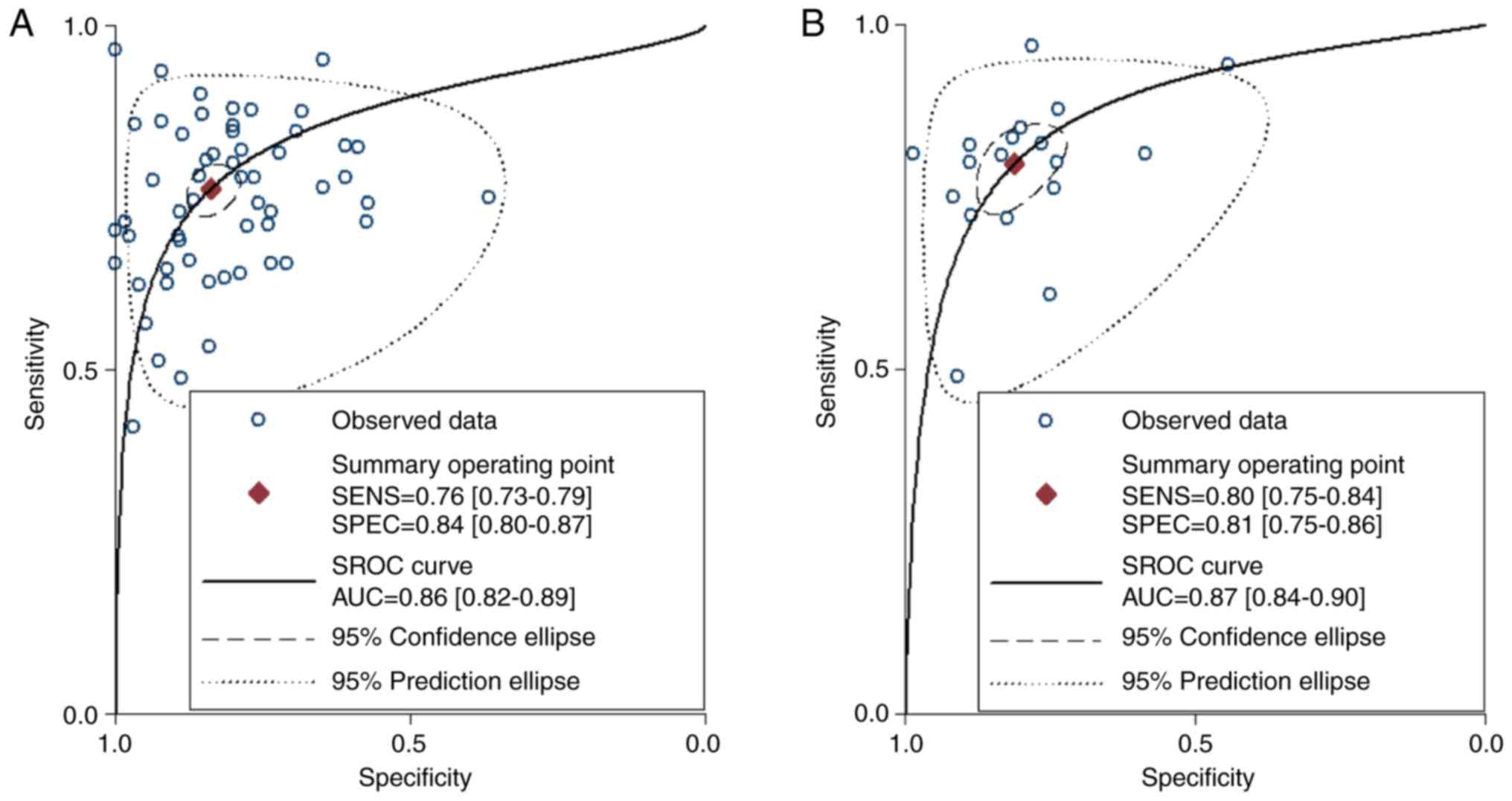
peripheral blood-based assays. Moreover, further research was
conducted to identify whether the upregulated miRNAs had better
diagnostic accuracy than the downregulated miRNAs. Thus, the
altered expression subgroup analyses for all miRNAs are shown in
Table II and Fig. 8, the variable value in both changed
slightly, according to the data of DOR (15.18 and 15.93) and AUC
(0.86 and 0.87), which revealed that the diagnostic performance of
miRNAs for GC detection in the high expression group was similar to
that in the low expression group. From the above subgroup analysis
that sought to determine the source of heterogeneity, the results
indicated that the subgroups involving patients in the TNM (I–II)
stage (I2=41.2%) using peripheral blood samples
(I2=15.6%), contributed to moderate and mild
heterogeneity, respectively. In addition, the decreasing trend in
alteration implicitly suggested that the two factors may possibly
be the source of heterogeneity. Nevertheless, further steps were
taken to determine whether the aforementioned controversy led to
the heterogeneity partly or entirely, which was confirmed by
meta-regression analysis.
Meta-regression analysis
Based on the characteristics of the included
studies, covariates, including TNM classification of GC, miRNA
profiling, specimen types, miRNAs screening approaches, and
aberrant expression status were applied to investigate inter-study
heterogeneity using a meta-regression model shown in Table III (A-E). In the meta-regression
analysis, sources of significant heterogeneity statistically
indicated that the specimen type of the miRNA contributed
significantly (P=0.0014), while the heterogeneity of results was
not significantly influenced by the rest of the covariates. In
accordance with the above results, the study sample type could be
considered as a source of heterogeneity for GC detection in
meta-regression.
| Table III.Meta regression to evaluate the
inter-subgroup heterogeneity of miRNAs for the diagnosis of gastric
cancer patients. |
Table III.
Meta regression to evaluate the
inter-subgroup heterogeneity of miRNAs for the diagnosis of gastric
cancer patients.
| A, Five
covariates |
|---|
|
|---|
| Variables | Coeff. | Sth. Err | P-value | RDOR | (95% CI) |
|---|
| Cte. | 3.059 | 0.4343 | 0.0000 | – | – |
| S | −0.301 | 0.0735 | 0.0001 | – | – |
| TNM stage | 0.186 | 0.1119 | 0.1004 | 1.20 | (0.96;1.51) |
|
Up/downregulation | −0.012 | 0.2047 | 0.9535 | 0.99 | (0.66;1.49) |
| miR screening | −0.478 | 0.2051 | 0.0226 | 0.62 | (0.41;0.93) |
| Sample type | −0.415 | 0.1361 | 0.0032 | 0.66 | (0.50;0.87) |
|
Single/multiple | 0.254 | 0.2299 | 0.2728 | 1.29 | (0.82;2.04) |
|
| Tau-squared
estimate=0.2689 (convergence is achieved after 6 iterations).
Restricted Maximum Likelihood estimation (REML). No. studies=48
containing 77 miRNAs. Filter OFF. Add 1/2 to all cells of the
studies with zero. Cte, constant coefficient; S, statistic; RDOR,
relative diagnostic odds ratio. |
|
| B, Four
covariates |
|
|
Variables | Coeff. | Std.
Err | P-value | RDOR | (95%
CI) |
|
| Cte. | 3.048 | 0.4183 | 0.0000 | – | – |
| S | −0.300 | 0.0730 | 0.0001 | – | – |
| TNM stage | 0.188 | 0.1078 | 0.0851 | 1.21 | (0.97;1.50) |
| miR screening | −0.479 | 0.2029 | 0.0209 | 0.62 | (0.41;0.93) |
| Sample type | −0.416 | 0.1329 | 0.0025 | 0.66 | (0.51;0.86) |
|
Single/multiple | 0.255 | 0.2272 | 0.2658 | 1.29 | (0.82;2.03) |
|
| Tau-squared
estimate=0.2606 (convergence is achieved after 6 iterations).
Restricted Maximum Likelihood estimation (REML). No. studies=48
containing 77 miRNAs. Filter OFF. Add 1/2 to all cells of the
studies with zero. Cte, constant coefficient; S, Statistic; RDOR,
relative diagnostic odds ratio. |
|
| C, Three
covariates |
|
|
Variables | Coeff. | Std.
Err | P-value | RDOR | (95%
CI) |
|
| Cte. | 3.364 | 0.3156 | 0.0000 | – | – |
| S | −0.328 | 0.0696 | 0.0000 | – | – |
| TNM stage | 0.176 | 0.1086 | 0.1085 | 1.19 | (0.96;1.48) |
| miR screening | −0.402 | 0.1932 | 0.0409 | 0.67 | (0.46;0.98) |
| Sample type | −0.428 | 0.1340 | 0.0021 | 0.65 | (0.50;0.85) |
|
| Tau-squared
estimate=0.2727 (convergence is achieved after 6 iterations).
Restricted Maximum Likelihood estimation (REML). No. studies=48
containing 77 miRNAs. Filter OFF. Add 1/2 to all cells of the
studies with zero. Cte, constant coefficient; S, Statistic; RDOR,
relative diagnostic odds ratio. |
|
| D, Two
covariates |
|
|
Variables | Coeff. | Std.
Err | P-value | RDOR | (95%
CI) |
|
| Cte. | 3.630 | 0.2759 | 0.0000 | – | – |
| S | −0.328 | 0.0706 | 0.0000 | – | – |
| miR screening | −0.355 | 0.1944 | 0.0716 | 0.70 | (0.48;1.03) |
| Sample type | −0.476 | 0.1328 | 0.0006 | 0.62 | (0.48;0.81) |
|
| Tau-squared
estimate=0.2899 (convergence is achieved after 6 iterations).
Restricted Maximum Likelihood estimation (REML). No. studies=48
containing 77 miRNAs. Filter OFF. Add 1/2 to all cells of the
studies with zero. Cte, constant coefficient; S, Statistic; RDOR,
relative diagnostic odds ratio. |
|
| E, One
covariate |
|
|
Variables | Coeff. | Std.
Err | P-value | RDOR | (95%
CI) |
|
| Cte. | 3.474 | 0.2661 | 0.0000 | – | – |
| S | −0.335 | 0.0717 | 0.0000 | – | – |
| Sample type | −0.445 | 0.1340 | 0.0014 | 0.64 | (0.49;0.84) |
| Tau-squared
estimate=0.3116 (convergence is achieved after 6 iterations).
Restricted Maximum Likelihood estimation (REML). No. studies=48
containing 77 miRNAs. Filter OFF. Add 1/2 to all cells of the
studies with zero. Cte, constant coefficient; S, Statistic; RDOR,
relative diagnostic odds ratio. |
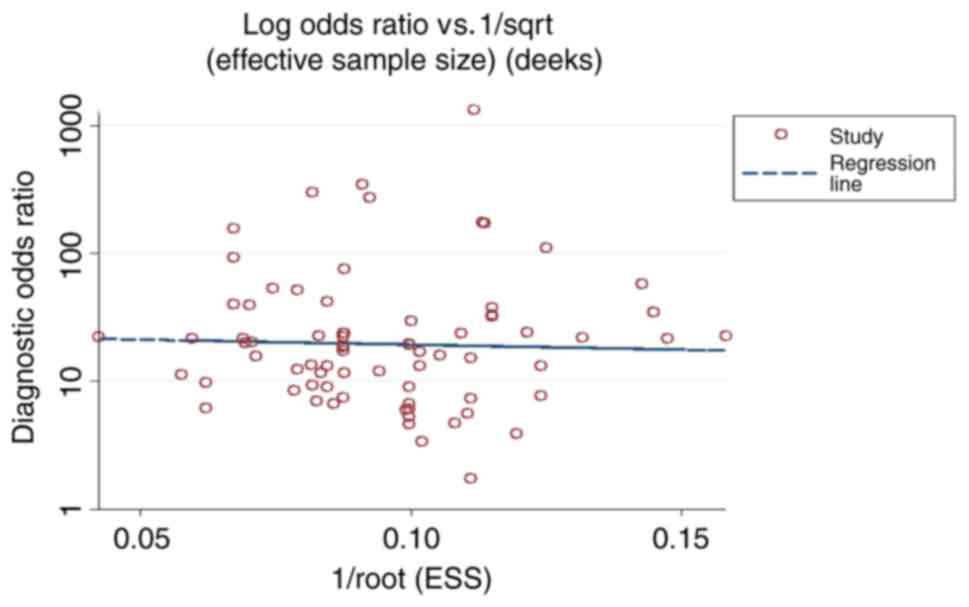
Publication bias
Deeks' funnel plot asymmetry test was applied to
explore the publication bias of meta-analysis in diagnostic
accuracy (24). The slope
coefficient was associated with a P-value of 0.756 for GC detection
(Fig. 9), suggesting a low
likelihood of publication bias in our meta-analysis.
Discussion
GC is responsible for the highest number of
cancer-related mortalities (74),
and the egregious mortality of GC is immeasurably more acute than
ever before, primarily since the majority of patients have a
terminal disease at stage III or IV at the time of diagnosis
(75). In addition, there are many
investigated biomarkers, such as CEA and CA724, which lack
sufficient sensitivity and specificity for early GC diagnosis
(76), and universal screening
tools, such as endoscopic examinations and biopsies, are invasive,
unpleasant, and inconvenient, leading to potential errors in GC
detection. Hence, ideal non-invasive biomarkers are urgently
required to reinforce GC detection. At present, a large number of
studies on the search for novel tumor biomarkers have revealed that
miRNAs may play a pivotal role in cancer suppression, owing to the
diverse miRNA expression levels that are observed between cancer
patients and healthy controls (45,48,77,78).
Subsequently, research has gravitated towards miRNAs as biological
markers for tumor diagnosis. Nevertheless, the results of research
on the use of miRNAs for gastrointestinal cancer detection are
conflicting among different studies (33,38,44,45,47,48,79,80).
To the best of our knowledge, several meta-analysis studies have
been undertaken to determine the differentially expressed miRNAs in
GC patients. Unfortunately, as a result of insufficient data or
inconsistent results, abundant heterogeneity influenced the
results. Furthermore, the accuracy of performance using the pooled
results influenced interpretation. In the present meta-analysis, we
included 48 studies involving miRNA expression profiling to
systematically and comprehensively evaluate the potential
diagnostic value of circulating miRNAs as diagnostic markers for
GC. We considered different perspectives while avoiding statistical
outcomes that included the absence of homogeneity.
The pooled outcomes of sensitivity, specificity, and
AUC (0.76, 0.81, and 0.86, respectively) with the random effects
model revealed that circulating miRNAs have better diagnostic value
than CEA and CAA199 (AUC of 0.55 and 0.60, respectively) in
distinguishing GC patients from control groups. Moreover, the DOR
of circulating miRNAs for GC detection was 15.72, reflecting higher
diagnostic performance as a combinative parameter of sensitivity
and specificity. In fact, by pooling data in this manner, the
diagnostic value would be inaccurate due to the significant
heterogeneity and diagnostic threshold. Thus, we could not
interpret the statistical outcomes blindly while neglecting high
heterogeneity. Additionally, it was suitable to explore subgroup
and regression analyses.
From the subgroup analysis, our results indicated
that the non-microarray screening approach, multiple miRNA assay,
and serum-based miRNA assay manifested a relatively higher
diagnostic value and accuracy for GC than the single-miRNA,
microarray profiling screening, and plasma-based miRNA groups. The
altered expression of the single miRNA in serum or plasma
fluctuated not only in GC but also in other tumors, infectious
diseases, nonspecific inflammation, and acute injuries. In other
words, single miRNAs lacked specificity in cancer detection.
However, for multiple miRNAs with complex molecular mechanisms,
such as a competing endogenous RNA (ceRNA) network intersecting at
tumorigenesis (e.g., initiation and development of a severe
neoplasm), the association may be valuable for early GC detection.
Hence, studies highlighting individual cancer-specific miRNAs in
serum or plasma usually arrived at unsatisfactory results.
Non-microarray screening and serum-based diagnostic
tests yielded better outcomes than microarray screening pathways
and plasma-based investigations of GC. However, the origin of
source-related differences was still unclear. There are many
complex factors that must be accounted for, such as lower
homogeneity of included studies and a limited number of samples.
Therefore, large-scale investigations and multiple center trials
should be undertaken in the future to uncover the underlying
mechanism of aberrant expression of miRNAs and to determine whether
the source-related discrepancies truly exist or not.
Another finding was that the diagnostic value of
miRNAs in early stages I–II and high expression groups were
approximately similar to those in stages I–IV and lower expression
groups in the detection of GC. In the GC microenvironment, a
variety of differentiated tumor cells and cancer-associated cells,
such as different types of immune cells and cells with different
proliferative activity, lead to the transcriptome dysfunction
during the tumorigenesis process due to inactivation of tumor
suppressors and activation of proto-oncogenes. With respect to
cancer, immune cells have the capacity to release exosomes that
accompany cell migration, shuttling the ceRNA network into
circulation (81), whereas the
circulating tumor cells may express non-coding RNA under the
control of an oncogene. Moreover, the overexpression of miRNAs may
silence the mRNAs from tumor suppressor genes and downregulated
miRNAs may facilitate the expression of oncogene mRNAs by binding
the 3′-untranslated region of the target mRNA. In early and
advanced GC, the aberrant and abundant expression of some miRNAs
may be associated with this process. Moreover, a lack of
specificity in the aforementioned may occur not only in GC but in
many tumors, leading to various conclusions regarding GC
discrimination. For instance, Liu et al (50) suggested that miRNA expression levels
during earlier stages (I and II) were different from those during
later stages (III and IV), exhibiting that this miRNA could be
valuable for the early detection of GC. Evidently, we arrived at a
paradox with our results conflicting with the conclusions of these
authors. Therefore, it is difficult to distinguish which is a
suitable and specific biomarker for GC. It would be beneficial to
study individual miRNAs by determining their molecular mechanism
rather than using the combination methodology.
The present study does have some limitations that
must be addressed. First, methodologies for a precise uniform
quantification of miRNAs face a lack of consistent criteria,
limiting the comparisons made between studies that are conducted by
different laboratories who have their own study design, use of
miRNA chips, pathology type, localization of GC lesions, and
different endogenous miRNA references. Second, there are some
specific circulating miRNAs that are always prone to be selected by
certain studies in determining the correlation between grade and
stage of cancer. Consequently, a standardized protocol, which would
be preferable, is required to abate bias. Moreover, the included
studies in the present meta-analysis only distinguished the tumor
patients from healthy controls, but other risk factors, such as
chronic gastritis, infectious disease, genetic, ulcers, and diet,
were not included and these may contribute to altered miRNA
expression (4,82). Therefore, further accurate studies
on the use of miRNAs for distinguishing cancer from other diseases
are urgently needed.
In conclusion, our meta-analysis found that the
combination of multiple miRNAs, non-microarray chip screening, and
serum-based miRNA assays may present a better performance for the
diagnosis of GC. However, many unclear molecular mechanisms
hindered discovery for clear GC detection biomarkers. Therefore,
the results should be interpreted cautiously given the uncertainty
of the results. Further large-scale prospective studies are
required to validate the potential applicability in human cancer
diagnosis.
Acknowledgements
I would like to thank all authors that were involved
in this study. In addition, we are appreciative of the support from
Professors YPW and WMS.
Funding
This study was supported by the National Natural
Science Foundation of China (81570783), the National Key Research
and Development Program of China (2016YFC1302200), the Gansu
Natural Science Foundation of China (1606RJZA136), the Health
Industry Research Project of the Gansu Province (GWGL2014-01), the
Scientific Research Project of Traditional Chinese Medicine
Administration in Gansu Province (GZK-2017-48), the Open Fund of
State Key Laboratory of Cancer Biology (CBSKL201718), and the
Fundamental Research Funds for the Central Universities
(lzujbky-2015-258).
Availability of data and materials
All data generated or analyzed in this study are
included in this published article.
Authors' contributions
HuiW, KP, XGL, BXL, HSZ, HuanW, HaoW, WMS and YPW
contributed to the conception and design of the study, literature
review and analysis, drafting and critical revision and editing,
and approval of the final version.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AUROC
|
area under the receiver operating
characteristic curve
|
|
CI
|
confidence interval
|
|
DOR
|
diagnostic odds ratio
|
|
FN
|
false negative
|
|
FP
|
false positive
|
|
GC
|
gastric cancer
|
|
LR
|
likelihood ratio
|
|
QUADAS
|
quality assessment of diagnostic
accuracy studies
|
|
SE
|
sensitivity
|
|
SP
|
specificity
|
|
TP
|
true positive
|
|
TN
|
true negative
|
|
TNM
|
tumor-node-metastasis
|
References
|
1
|
Liu L, Wang S, Cao X and Liu J: Diagnostic
value of circulating microRNAs for gastric cancer in Asian
populations: A meta-analysis. Tumor Biol. 35:11995–2004. 2014.
View Article : Google Scholar
|
|
2
|
World Health Organization. Cancer Fact
Sheets. http://globocan.iarc.fr/Pages/fact_sheets_population.aspx
|
|
3
|
Duguan FU: Epigenetic alterations in
gastric cancer (Review). Mol Med Rep. 12:3223–3230. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang QX, Zhu YQ, Zhang H and Xiao J:
Altered MiRNA expression in gastric cancer: A systematic review and
meta-analysis. Cell Physiol Biochem. 35:933–944. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Charalampakis N, Economopoulou P,
Kotsantis I, Tolia M, Schizas D, Liakakos T, Elimova E, Ajani JA
and Psyrri A: Medical management of gastric cancer: A 2017 update.
Cancer Med. 7:123–133. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hu N, Yin JF, Ji Z, Hong Y, Wu P, Bian B,
Song Z, Li R, Liu Q and Wu F: Strengthening gastric cancer therapy
by trastuzumab-conjugated nanoparticles with simultaneous
encapsulation of anti-MiR-21 and 5-Fluorouridine. Cell Physiol
Biochem. 44:2158–2173. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Huang S, Wang J, Li J, Luo Q, Zhao M,
Zheng L, Dong X, Chen C, Che Y, Liu P, et al: Serum microRNA
expression profile as a diagnostic panel for gastric cancer. Jpn J
Clin Oncol. 46:8112016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kitano S, Shiraishi N, Uyama I, Sugihara K
and Tanigawa N: Japanese Laparoscopic Surgery Study Group: A
multicenter study on oncologic outcome of laparoscopic gastrectomy
for early cancer in Japan. Ann Surg. 245:68–72. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Uedo N, Takeuchi Y and Ishihara R:
Endoscopic management of early gastric cancer: Endoscopic mucosal
resection or endoscopic submucosal dissection: Data from a Japanese
high-volume center and literature review. Ann Gastroenterol.
25:281–290. 2012.PubMed/NCBI
|
|
11
|
Kaneko S and Yoshimura T: Time trend
analysis of gastric cancer incidence in Japan by histological
types. 1975–1989. Br J Cancer. 84:400–405. 2001. View Article : Google Scholar
|
|
12
|
Bonenkamp JJ, Hermans J, Sasako M, van de
Velde CJ, Welvaart K, Songun I, Meyer S, Plukker JT, Van Elk P,
Obertop H, et al: Extended lymph-node dissection for gastric
cancer. N Engl J Med. 340:908–914. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Garrido M, Bustos M, Orellana E, Madrid J,
Galindo H, Sánchez C, Pimentel F, Guzmán S, Ibáñez L, Butte JM, et
al: Postoperative radio chemotherapy in locally advanced gastric
cancer. Rev Med Chil. 136:844–850. 2008.(In Spanish). PubMed/NCBI
|
|
14
|
Madhavan D, Cuk K, Burwinkel B and Yang R:
Cancer diagnosis and prognosis decoded by blood-based circulating
microRNA signatures. Front Genet. 4:1162013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Komatsu S, Ichikawa D, Tsujiura M, Konishi
H, Takeshita H, Nagata H, Kawaguchi T, Hirajima S, Arita T,
Shiozaki A, et al: Prognostic impact of circulating miR-21 in the
plasma of patients with gastric carcinoma. Anticancer Res.
33:271–276. 2013.PubMed/NCBI
|
|
16
|
Chen CZ: MicroRNAs as oncogenes and tumor
suppressors. N Engl J Med. 353:1768–1771. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee RC, Feinbaum RL and Ambros V: The C.
elegans heterochronic gene lin-4 encodes small RNAs with antisense
complementarity to lin-14. Cell. 75:843–854. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gorur A, Balci Fidanci S, Dogruer Unal N,
Ayaz L, Akbayir S, Yildirim Yaroglu H, Dirlik M, Serin MS and Tamer
L: Determination of plasma microRNA for early detection of gastric
cancer. Mol Biol Rep. 40:2091–2096. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mitchell PS, Parkin RK, Kroh EM, Fritz BR,
Wyman SK, Pogosova-Agadjanyan EL, Peterson A, Noteboom J, O'Briant
KC, Allen A, et al: Circulating microRNAs as stable blood-based
markers for cancer detection. Proc Natl Acad Sci USA.
105:10513–10518. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Whiting PF, Rutjes AW, Westwood ME,
Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA and Bossuyt
PM: QUADAS-2 Group: QUADAS-2: A revised tool for the quality
assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Deeks JJ and Morris JM: 6 Evaluating
diagnostic tests. Baillière's Clin Obstet Gynaecol. 10:613–630.
1996. View Article : Google Scholar
|
|
22
|
Deeks JJ: Systematic reviews in health
care: Systematic reviews of evaluations of diagnostic and screening
tests. BMJ. 323:157–162. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jaeschke R, Guyatt GH and Sackett DL:
Users' guides to the medical literature. III. How to use an article
about a diagnostic test. B. What are the results and will they help
me in caring for my patients? The Evidence-Based Medicine Working
Group. JAMA. 271:703–707. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Deeks JJ, Macaskill P and Irwig L: The
performance of tests of publication bias and other sample size
effects in systematic reviews of diagnostic test accuracy was
assessed. J Clin Epidemiol. 58:882–893. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Jackson D, White IR and Thompson SG:
Extending DerSimonian and Laird's methodology to perform
multivariate random effects meta-analyses. Stat Med. 29:1282–1297.
2010. View
Article : Google Scholar : PubMed/NCBI
|
|
27
|
Peng WZ, Ma R, Wang F, Yu J and Liu ZB:
Role of miR-191/425 cluster in tumorigenesis and diagnosis of
gastric cancer. Int J Mol Sci. 15:4031–4048. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Qiu X, Zhang J, Shi W, Liu S, Kang M, Chu
H, Wu D, Tong N, Gong W, Tao G, et al: Circulating microRNA-26a in
plasma and its potential diagnostic value in gastric cancer. PLoS
One. 11:e01513452016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tsujiura M, Komatsu S, Ichikawa D,
Shiozaki A, Konishi H, Takeshita H, Moriumura R, Nagata H,
Kawaguchi T, Hirajima S, et al: Circulating miR-18a in plasma
contributes to cancer detection and monitoring in patients with
gastric cancer. Gastric Cancer. 18:271–279. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhang J, Song Y, Zhang C, Zhi X, Fu H, Ma
Y, Chen Y, Pan F, Wang K, Ni J, et al: Circulating MiR-16-5p and
MiR-19b-3p as two novel potential biomarkers to indicate
progression of gastric cancer. Theranostics. 5:733–745. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tsai MM, Wang CS, Tsai CY, Huang CG, Lee
KF, Huang HW, Lin YH, Chi HC, Kuo LM, Lu PH and Lin KH: Circulating
microRNA-196a/b are novel biomarkers associated with metastatic
gastric cancer. Eur J Cancer. 64:137–148. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Su ZX, Zhao J, Rong ZH, Wu YG, Geng WM and
Qin CK: Diagnostic and prognostic value of circulating miR-18a in
the plasma of patients with gastric cancer. Tumor Biol.
35:12119–12125. 2014. View Article : Google Scholar
|
|
33
|
Valladares-Ayerbes M, Reboredo M,
Medina-Villaamil V, Iglesias-Díaz P, Lorenzo-Patiño MJ, Haz M,
Santamarina I, Blanco M, Fernández-Tajes J, Quindós M, et al:
Circulating miR-200c as a diagnostic and prognostic biomarker for
gastric cancer. J Transl Med. 10:1862012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhu X, Yang Z, Zhang J and Liu H:
Investigation of microRNA-145 as a serum diagnostic and prognostic
biomarker for gastric cancer: A Chinese cohort-based study. Int J
Clin Exp Med. 10:9440–9447. 2017.
|
|
35
|
Zhuang K, Han K, Tang H, Yin X, Zhang J,
Zhang X and Zhang L: Up-regulation of plasma miR-23b is associated
with poor prognosis of gastric cancer. Med Sci Monit. 22:356–361.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hung PS, Chen CY, Chen WT, Kuo CY, Fang
WL, Huang KH, Chiu PC and Lo SS: MiR-376c promotes carcinogenesis
and serves as a plasma marker for gastric carcinoma. PLoS One.
12:e01773462017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Le Q, Jianhua N, Mulati, Yu X and Jiageng
H: Increased miR-25 expression in serum of gastric cancer patients
is correlated with CA19-9 and acts as a potential diagnostic
biomarker. Open Medicine. 12:266–270. 2017. View Article : Google Scholar
|
|
38
|
Li BS, Zhao YL, Guo G, Li W, Zhu ED, Luo
X, Mao XH, Zou QM, Yu PW, Zuo QF, et al: Plasma microRNAs, miR-223,
miR-21 and miR-218, as novel potential biomarkers for gastric
cancer detection. PLoS One. 7:e416292012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Li F, Guo Y, Liu J and Zhang R: The
significance of elevated plasma expression of microRNA 106b~25
clusters in gastric cancer. PLoS One. 12:e01784272017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Li M, Gu K, Liu W, Xie X and Huang X:
MicroRNA-200c as a prognostic and sensitivity marker for platinum
chemotherapy in advanced gastric cancer. Oncotarget. 8:51190–51199.
2017.PubMed/NCBI
|
|
41
|
Hou X, Zhang M and Qiao H: Diagnostic
significance of miR-106a in gastric cancer. Int J Clin Exp Pathol.
8:13096–13101. 2015.PubMed/NCBI
|
|
42
|
Hou CG, Luo XY and Li G: Diagnostic and
prognostic value of serum MicroRNA-206 in patients with gastric
cancer. Cell Physiol Biochem. 39:1512–1520. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhang WH, Gui JH, Wang CZ, Chang Q, Xu SP,
Cai CH, Li YN, Tian YP, Yan L and Wu B: The identification of
miR-375 as a potential biomarker in distal gastric adenocarcinoma.
Oncol Res. 20:139–147. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Song MY, Pan KF, Su HJ, Zhang L, Ma JL, Li
JY, Yuasa Y, Kang D, Kim YS and You WC: Identification of serum
microRNAs as novel non-invasive biomarkers for early detection of
gastric cancer. PLoS One. 7:e336082012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Tsujiura M, Ichikawa D, Komatsu S,
Shiozaki A, Takeshita H, Kosuga T, Konishi H, Morimura R, Deguchi
K, Fujiwara H, et al: Circulating microRNAs in plasma of patients
with gastric cancers. Br J Cancer. 102:1174–1179. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wang B and Zhang Q: The expression and
clinical significance of circulating microRNA-21 in serum of five
solid tumors. J Cancer Res Clin Oncol. 138:1659–1666. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zhu C, Ren C, Han J, Ding Y, Du J, Dai N,
Dai J, Ma H, Hu Z, Shen H, et al: A five-microRNA panel in plasma
was identified as potential biomarker for early detection of
gastric cancer. Br J Cancer. 110:2291–2299. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Liu R, Zhang C, Hu Z, Li G, Wang C, Yang
C, Huang D, Chen X, Zhang H, Zhuang R, et al: A five-microRNA
signature identified from genome-wide serum microRNA expression
profiling serves as a fingerprint for gastric cancer diagnosis. Eur
J Cancer. 47:784–791. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Konishi H, Ichikawa D, Komatsu S, Shiozaki
A, Tsujiura M, Takeshita H, Morimura R, Nagata H, Arita T,
Kawaguchi T, et al: Detection of gastric cancer-associated
microRNAs on microRNA microarray comparing pre- and post-operative
plasma. Br J Cancer. 106:740–747. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Liu H, Zhu L, Liu B, Yang L, Meng X, Zhang
W, Ma Y and Xiao H: Genome-wide microRNA profiles identify miR-378
as a serum biomarker for early detection of gastric cancer. Cancer
Lett. 316:196–203. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Liu X, Kwong A, Sihoe A and Chu KM: Plasma
miR-940 may serve as a novel biomarker for gastric cancer. Tumor
Biol. 37:3589–3597. 2016. View Article : Google Scholar
|
|
52
|
Hu Y, Wang J, Han Y, Liu Q and Niu Q:
Serum miR-133a is down-regulated and associated with the diagnosis
of patients with gastric cancer. Int J Clin Exp Pathol.
9:2015–2020. 2016.
|
|
53
|
Sun Y, Ma J, Hu M, Zheng X, Li J and Gu
Wei: Level of miR-183 in peripheral blood of the patients with
gastric cancer. J Shanghai Jiaotong Univ. 37:75–79. 2017.
|
|
54
|
Li B and Zhang H: Plasma microRNA-320 is a
potential diagnostic and prognostic bio-marker in gastric cancer.
Int J Clin Exp Pathol. 10:7356–7361. 2017.
|
|
55
|
Wu J, Li G, Yao Y, Wang Z, Sun W and Wang
J: MicroRNA-421 is a new potential diagnosis biomarker with higher
sensitivity and specificity than carcinoembryonic antigen and
cancer antigen 125 in gastric cancer. Biomarkers. 20:58–63. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Zeng Q, Jin C, Chen W, Xia F, Wang Q, Fan
F, Du J, Guo Y, Lin C, Yang K, et al: Downregulation of serum
miR-17 and miR-106b levels in gastric cancer and benign gastric
diseases. Chin J Cancer Res. 26:711–716. 2014.PubMed/NCBI
|
|
57
|
Zhou H, Xiao B, Zhou F, Deng H, Zhang X,
Lou Y, Gong Z, Du C and Guo J: MiR-421 is a functional marker of
circulating tumor cells in gastric cancer patients. Biomarkers.
17:104–110. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Zhou X, Zhu W, Li H, Wen W, Cheng W, Wang
F, Wu Y, Qi L, Fan Y, Chen Y, et al: Diagnostic value of a plasma
microRNA signature in gastric cancer: A microRNA expression
analysis. Sci Rep. 5:112512015. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Wu J, Li G, Wang Z, Yao Y, Chen R, Pu X
and Wang J: Circulating MicroRNA-21 is a potential diagnostic
biomarker in gastric cancer. Dis Markers. 2015:4356562015.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Wu D, Cao G, Huang Z, Jin K, Hu H, Yu J
and Zeng Y: Decreased miR-503 expression in gastric cancer is
inversely correlated with serum carcinoembryonic antigen and acts
as a potential prognostic and diagnostic biomarker. OncoTargets
Ther. 10:129–135. 2017. View Article : Google Scholar
|
|
61
|
Wang H, Wang L, Wu Z, Sun R, Jin H, Ma J,
Liu L, Ling R, Yi J, Wang L, et al: Three dysregulated microRNAs in
serum as novel biomarkers for gastric cancer screening. Med Oncol.
31:2982014. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Shin VY, Ng EK, Chan VW, Kwong A and Chu
KM: A three-miRNA signature as promising non-invasive diagnostic
marker for gastric cancer. Mol Cancer. 14:2022015. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Cui YJ, Xie XH, Xing YF, Yuan ZH, Wu QY
and Wei YM: Feasibility study on plasmatic microRNA-27b-3p as a
potential biomarker for early diagnosis of gastric cancer. Tumor.
35:183–189. 2015.
|
|
64
|
Fu Z, Qian F, Yang X, Jiang H, Chen Y and
Liu S: Circulating miR-222 in plasma and its potential diagnostic
and prognostic value in gastric cancer. Med Oncol. 31:1642014.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Liu H, Yang Z, Zhang J and Zhu X:
MicroRNA-217 in plasma: A potential biomarker in gastric cancer.
Int J Clin Exp Med. 10:3313–3320. 2017.
|
|
66
|
Zhou H, Guo JM, Lou YR, Zhang XJ, Zhong
FD, Jiang Z, Cheng J and Xiao BX: Detection of circulating tumor
cells in peripheral blood from patients with gastric cancer using
microRNA as a marker. J Mol Med (Berl). 88:709–717. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zhou X and Zhang G: Exosome-mediated
transfer of miR-223 increases tumor malignancy in gastric cancer. J
Gastroen Hepatol (Australia). 31:45–46. 2016.
|
|
68
|
Zheng Y, Cui L, Sun W, Zhou H, Yuan X, Huo
M, Chen J, Lou Y and Guo J: MicroRNA-21 is a new marker of
circulating tumor cells in gastric cancer patients. Cancer Biomark.
10:71–77. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Li H, Wu Q, Li T, Liu C, Xue L, Ding J,
Shi Y and Fan D: The miR-17-92 cluster as a potential biomarker for
the early diagnosis of gastric cancer: Evidence and literature
review. Oncotarget. 8:45060–45071. 2017.PubMed/NCBI
|
|
70
|
Park JL, Kim M, Song KS, Kim SY and Kim
YS: Cell-Free miR-27a, a potential diagnostic and prognostic
biomarker for gastric cancer. Genomics Inform. 13:70–75. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Li C, Li JF, Cai Q, Qiu QQ, Yan M, Liu BY
and Zhu ZG: MiRNA-199a-3p: A potential circulating diagnostic
biomarker for early gastric cancer. J Surg Oncol. 108:89–92. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Li C, Li JF, Cai Q, Qiu QQ, Yan M, Liu BY
and Zhu ZG: MiRNA-199a-3p in plasma as a potential diagnostic
biomarker for gastric cancer. Ann Surg Oncol. 20((Suppl 3)):
S397–S405. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Liu S, Suo J, Wang C, Sun X, Wang D, He L,
Zhang Y and Li W: Prognostic significance of low miR-144 expression
in gastric cancer. Cancer Biomark. 20:547–552. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Lurje G, Schiesser M, Claudius A and
Schneider PM: Circulating tumor cells in gastrointestinal
malignancies: Current techniques and clinical implications. J
Oncol. 2010:3926522010. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Leung WK, Wu MS, Kakugawa Y, Kim JJ, Yeoh
KG, Goh KL, Wu KC, Wu DC, Sollano J, Kachintorn U, et al: Screening
for gastric cancer in Asia: Current evidence and practice. Lancet
Oncol. 9:279–287. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Redova M, Sana J and Slaby O: Circulating
miRNAs as new blood-based biomarkers for solid cancers. Future
Oncol. 9:387–402. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Shen J, Stass SA and Jiang F: MicroRNAs as
potential biomarkers in human solid tumors. Cancer Lett.
329:125–136. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Ng EK, Chong WW, Jin H, Lam EK, Shin VY,
Yu J, Poon TC, Ng SS and Sung JJ: Differential expression of
microRNAs in plasma of patients with colorectal cancer: A potential
marker for colorectal cancer screening. Gut. 58:1375–1381. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Zanutto S, Pizzamiglio S, Ghilotti M,
Bertan C, Ravagnani F, Perrone F, Leo E, Pilotti S, Verderio P,
Gariboldi M and Pierotti MA: Circulating miR-378 in plasma: A
reliable haemolysis independent biomarker for colorectal cancer. Br
J Cancer. 110:1001–1007. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Valadi H, Ekström K, Bossios A, Sjöstrand
M, Lee JJ and Lötvall JO: Exosome-mediated transfer of mRNAs and
microRNAs is a novel mechanism of genetic exchange between cells.
Nat Cell Biol. 9:654–659. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Matsushima K, Isomoto H, Inoue N, Nakayama
T, Hayashi T, Nakayama M, Nakao K, Hirayama T and Kohno S: MicroRNA
signatures in Helicobacter pylori-infected gastric mucosa. Int J
Cancer. 128:361–370. 2011. View Article : Google Scholar : PubMed/NCBI
|