Introduction
Irritable bowel syndrome (IBS) is a chronic
recurrent gastrointestinal disorder (1,2). IBS
comprises two subsets: sporadic (nonspecific) and postinfectious
(1,3). Sporadic IBS occurs in patients whose
symptoms have been present for a long time without any association
with gastrointestinal infections, while postinfectious IBS occurs
in patients who experience the sudden onset of symptoms following a
bout of gastroenteritis (1,3). The
absence of known anatomical, physiological, or biochemical defects
in IBS means that an IBS diagnosis is reached by exclusion, whereby
other gastrointestinal diseases that can cause symptoms similar to
those of IBS are ruled out (1–4).
Patients with IBS are therefore subjected to several expensive,
uncomfortable, and painful examinations before a diagnosis can be
made (1,3,4).
IBS and gastroesophageal reflux disease (GERD) are
common disorders in the population with prevalence of 11,2, and
20%, respectively (1–6). IBS and GERD overlap and meta-analysis
showed that the prevalence of GERD in IBS patients is four-fold
than in subjects without IBS (7–16).
Twins studies revealed that genetic factors are important in both
IBS and GERD (12). Moreover, IBS
and GERD symptoms cluster in families (12). It is not clear whether this overlap
occurs by chance as these disorders are common in the population or
because they share a common pathophysiology (17). However, population-based studies
showed that this overlap does not occur by chance (10). Whereas studies done on a large
number of Asian IBS patients have shown that IBS overlaps with
non-erosive esophagitis, but not with erosive esophagitis (7,16,18),
studies of a few European patients shown that erosive esophagitis
overlaps with IBS and occurs in 80% of IBS patients (8,19).
Symptom-based diagnosis criteria were introduced for
establishing a method for the positive diagnosis of IBS, with the
Rome IV criteria being the most recent (4,20–26).
The main goals of symptom-based diagnosis are to avoid unnecessary
expensive investigations and to facilitate the choice of treatment.
Rome criteria have been used extensively as inclusion criteria in
research studies as well as in clinical pharmacological trials.
However, there are several reasons why these criteria are not used
for the diagnosis of IBS in everyday clinical practice (4), such as clinicians being worried about
missing organic diseases that mimic IBS, and the complexity of
applying the criteria (4,27). Furthermore, patients are often
worried of having a serious or fatal disease, and are not reassured
without undergoing tests and examinations to rule out such diseases
(4).
The present retrospective study of a large number of
European patients, which has not been done before, aimed at
investigating the overlap of GERD with IBS and to determine whether
IBS is associated with erosive or non-erosive esophagitis.
Furthermore, it aimed at determining the probability of missing an
organic disease when applying the Rome criteria.
Materials and methods
Patients
Patients referred to the Section for
Gastroenterology, Stord Hospital from December 1, 2005 to December
31, 2016 who fulfilled the Rome III criteria for the diagnosis of
IBS were considered for inclusion in the study (26). Patients aged between 18 and 85
years without alarm features (red flags), any organic
gastrointestinal disease, or systemic disease were included in the
study. The red flags include unintentional weight loss, rectal
bleeding and/or anemia, signs of inflammation, family history of
colorectal cancer, inflammatory bowel disease (IBD), and celiac
disease (CD). Patients who had undergone any abdominal surgery were
excluded, with the exception of appendectomy, Cesarean section, and
hysterectomy.
In total, 1489 patients qualified for inclusion in
the study. They comprised 1331 females and 158 males with a mean
age of 51 years (range 18–82 years). Of these patients, 589 had
diarrhea as the predominant symptom, (IBS-D), 496 had constipation
as the predominant symptom, and 404 had a mixture of both diarrhea
and constipation (IBS-M). All patients underwent a thorough medical
history-taking and they were asked particularly about GERD
symptoms. Totally, 496 patients took proton pump inhibitor (PPI) on
demand. They were further investigated by blood tests, and had
normal findings for the full blood count, inflammatory markers,
electrolytes, folic acid, vitamin B12, and kidney, liver, and
thyroid function tests.
The Regional Committee for Medical and Health
Research Ethics West, Bergen, Norway waived the need for ethics
approval and the need to obtain consent for the collection,
analysis and publication of the retrospectively obtained and
anonymized data for this non-interventional study.
Endoscopy
All patients underwent standard gastroscopy and
colonoscopy, which were performed by an experienced single
gastroenterologist (MES). Gastroscopy was performed after an
overnight fast, during which four biopsy samples were taken from
the duodenum distal to the papilla of Vater. Patients used PPI were
asked not to take this medication one week prior to gastroscopy. A
routine colonoscopy was performed, during which two biopsies were
taken from each of the cecum, ascending colon, transverse colon,
descending colon, and sigmoid colon. Further biopsy samples were
taken from pathological findings when they were observed. The
biopsy samples were fixed overnight in 4% buffered
paraformaldehyde.
Histopathology and
immunohistochemistry
The biopsy samples obtained from the duodenum and
colon were processed to paraffin blocks that were cut into
5-µm-thick sections. The sections were stained with hematoxylin and
eosin and immunostained using the ultraView Universal DAB Detection
kit (v.1.02.0018; Venata Medical Systems, Basel, Switzerland) and
the BenchMark Ultra IHC/ISH staining module (Venata Medical
Systems). They were incubated with the primary antibody for 35 min
at 37°C. The primary antibodies used were monoclonal mouse
antihuman leukocytes CD45 (cat. no. IS751; Dako, Glostrup, Denmark)
and monoclonal antibodies to collagen type III (cat. no. P02461;
Acris, Herford, Germany). CD45 is considered a common leukocyte
antigen and is expressed exclusively on cells of the hematopoietic
system and their progenitors. The sections were examined for the
possible occurrence of CD using Marsh's modified classification.
Lymphocytic colitis was diagnosed in the presence of an increase in
intraepithelial lymphocytes (>15 lymphocytes/100 epithelial
cells), surface epithelial damage, increased lamina propria plasma
cells, and absent or minimal crypt architectural distribution
(28). Collagenous colitis was
diagnosed when there was an increase or irregularity in
subepithelial collagen (>10 µm) as well as the other
inflammatory changes seen in lymphocytic colitis (28).
Statistical analysis
The difference between IBS subtypes in the incidence
of GERD symptoms and erosive esophagitis were performed by
Chi-square test. Fisher's exact test was used for statistical
analysis, and the sensitivity, specificity, positive and negative
predictive values, and likelihood ratios when applying Rome III
criteria were calculated. The positive (+LR) and negative (-LR)
likelihood ratios are calculated as +LR=sensitivity/1−specificity)
and –LR=specificity/(1−sensitivity): +LR >10 is useful for
ruling IBS in and -LR <0.1 is useful for ruling IBS out
(29). These analyses were
performed using GraphPad Prism (v.7; La Jolla, CA, USA).
Results
Endoscopy and histopathology
Of the 1489 IBS patients, 983 (66%) complained, in
addition to IBS symptoms, of heartburn, acid regurgitation, nausea,
and globus (Table I). The
incidence of GERD symptom was higher in IBS-C and IBS-M than that
in IBS-D (Table II).
 | Table I.Gastroesophageal reflux disease
symptoms in the IBS patients studied. |
Table I.
Gastroesophageal reflux disease
symptoms in the IBS patients studied.
|
| Symptom observed,
n |
|---|
|
|
|
|---|
| Group | Heartburn | Regurgitation | Nausea | Globus |
|---|
| All IBS
patients | 802 | 798 | 345 | 10 |
| IBS-D | 205 | 198 | 2 | 1 |
| IBS-C | 341 | 342 | 56 | 14 |
| IBS-M | 310 | 298 | 1 | 0 |
| Table II.Prevalence of GERD and erosive
esophagitis in the total number of IBS patients studied and in the
IBS sub-types. |
Table II.
Prevalence of GERD and erosive
esophagitis in the total number of IBS patients studied and in the
IBS sub-types.
| Group | Patients with GERD,
n (%) | Patients with
erosive esophagitis, n (%) |
|---|
| IBS patients
total | 983 (66) | 14,449 (97) |
| IBS-D patients | 589 (55) | 575 (97) |
| IBS-C patients | 342
(69)a | 480 (97) |
| IBS-M patients | 320
(79)a | 394 (97) |
Gastroscopy revealed that of the 1489 IBS patients,
1449 have erosive esophagitis (97%), 25 had duodenal ulcers (1.7%),
and 9 had gastric ulcers (0.6%); the other patients had normal
endoscopy findings. Of the patients with erosive esophagitis 1128
(78%) esophagitis grade A, 298 (20.4%) grade B and 23 (1.6%) grade
C according to Los Angeles classification (30,31).
In IBS-D 575 (97%) patients had erosive esophagitis (97%). There
was no difference in the incidence of erosive esophagitis between
IBS-D and IBS-C (P=0.4), between IBS-D and IBS-M (P=0.9) or between
IBS-C and IBS-M (P=0.5) (Table
II).
The histopathological examinations of the duodenal
biopsies showed that 15 IBS-D patients had CD of Marsh type 1, 1
patient had CD of Marsh type 2, and 2 patients had CD of Marsh type
3b. The 15 patients with CD of Marsh type 1 underwent another
gastroscopy after 3–6 months, and new duodenal biopsy samples were
taken and re-examined histopathologically. Moreover, serological
tests for tissue transglutaminase antibodies (anti-tTG) IgA were
applied to these patients. Only 2 of the 15 original patients with
Marsh type 1 CD also showed Marsh type 1 CD in the second duodenal
biopsy samples, and positivity for anti-tTG IgA (Fig. 1). The other 13 patients had normal
histology findings and were negative for anti-tTG IgA. These five
patients with CD were all females (aged 20, 24, 36, 38, and 60
years) and belonging to the IBS-D subtype (Table III).
| Table III.Patients diagnosed with IBS by
applying the Rome III criteria and who were found to suffer from
other organic gastrointestinal diseases. |
Table III.
Patients diagnosed with IBS by
applying the Rome III criteria and who were found to suffer from
other organic gastrointestinal diseases.
| Number of patients,
n (females/males) | Endoscopy and
histopathological findings, n (%); (females/males) |
|---|
| Total | IBS-D | IBS-M | IBS-C | Celiac disease | Crohn's
disease | Ulcerative
colitis | Collagenous
colitis | Lymphocytic
colitis | Colon cancer |
|---|
| 1,489
(1,331/158) | 589 (531/58) | 404 (368/36) | 496 (432/64) | 5 (0.3); (5/0) | 3 (0.2); (3/0) | 1 (0.07);
(0/1) | 2 (0.1); (0/2) | 7 (0.5); (5/2) | 3 (0.2); (1/2) |
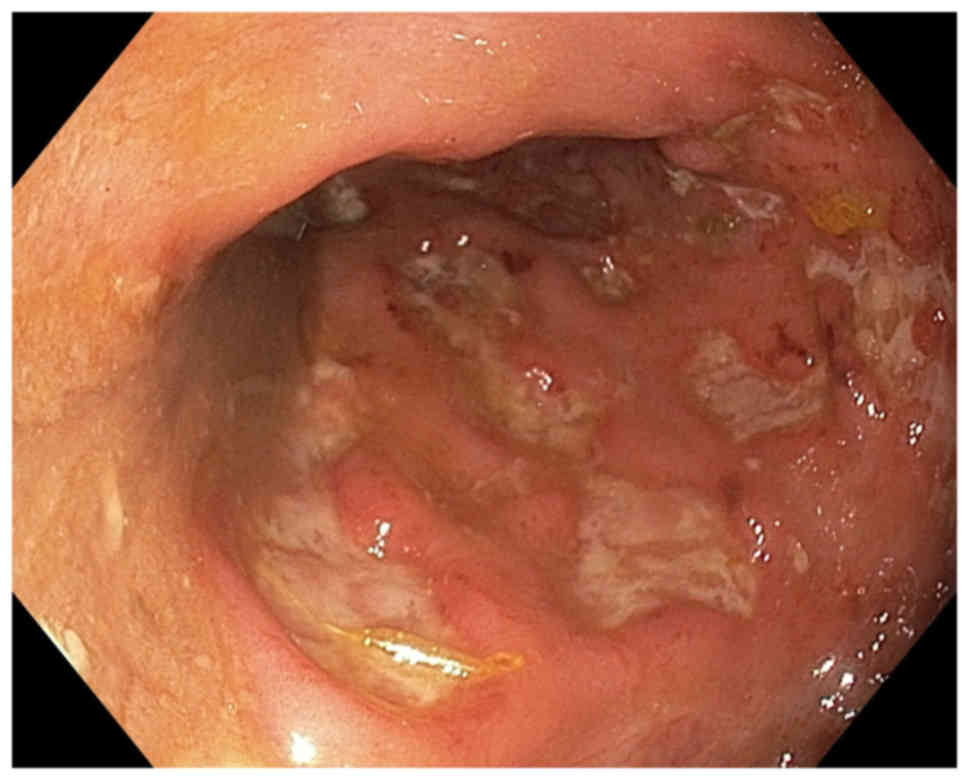
Colonoscopy examinations showed that the ileum,
colon, and rectum were endoscopically normal in all of the IBS
patients except for seven of those with IBS-D (Table III). Three of these patients had
scattered aphthoid ulcers in the mucosa of the terminal ileum
(Fig. 2). Histopathological
examinations confirmed the diagnosis of Crohn's disease. These
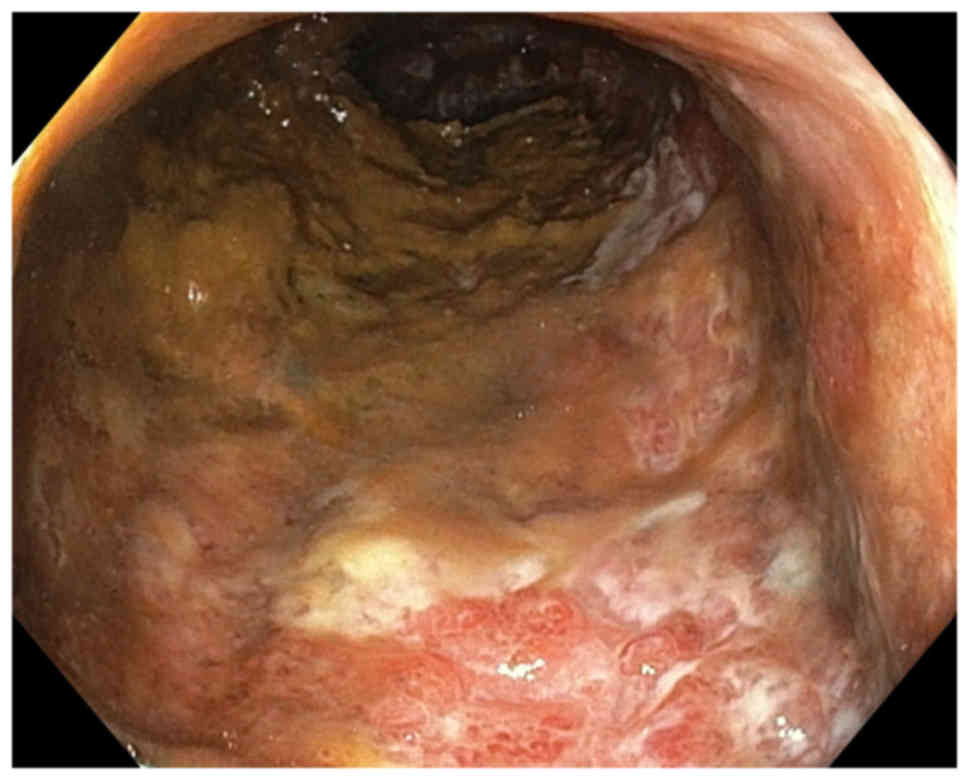
patients were all females, and were aged 28, 32, and 59 years. The
fourth patient had erythematous friable mucosa with loss of the
normal vascular pattern, with this lesion including 10 cm of the
sigmoid colon and the entire rectum (Fig. 3). Histopathological examinations of
the biopsy samples taken from the lesions revealed ulcerative
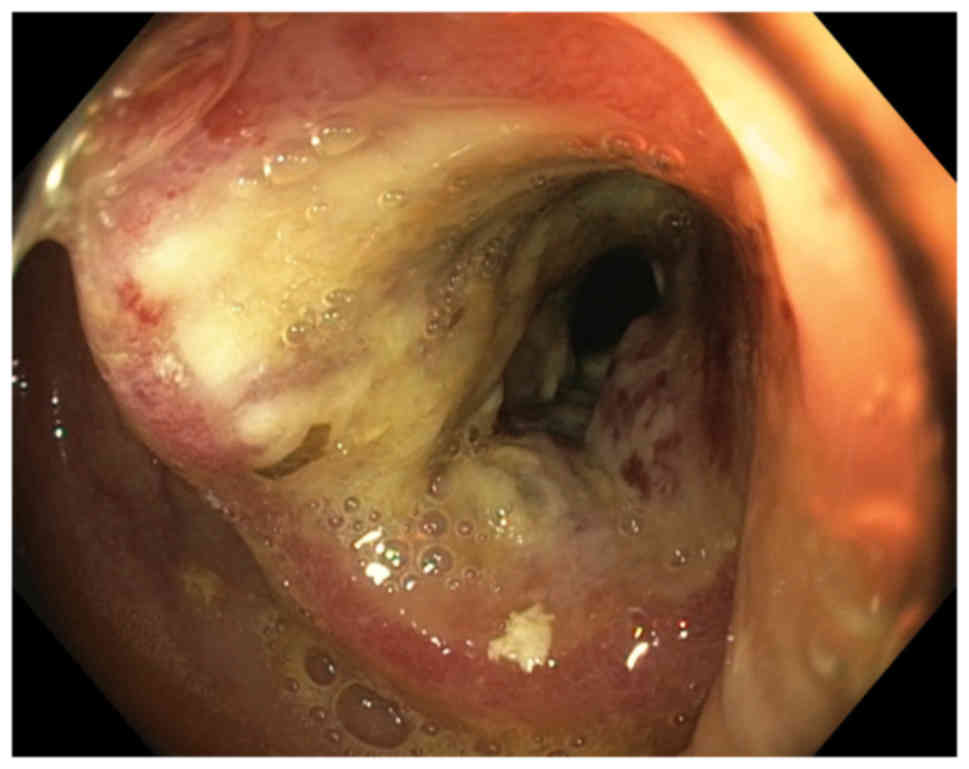
colitis. This patient was a female aged 57 years. The remaining
three patients each had a tumor in the sigmoid colon (Fig. 4), which histopathological
examinations of the biopsy samples revealed to be adenocarcinomas.
These patients were a female aged 58 years and two males aged 52
and 56 years.
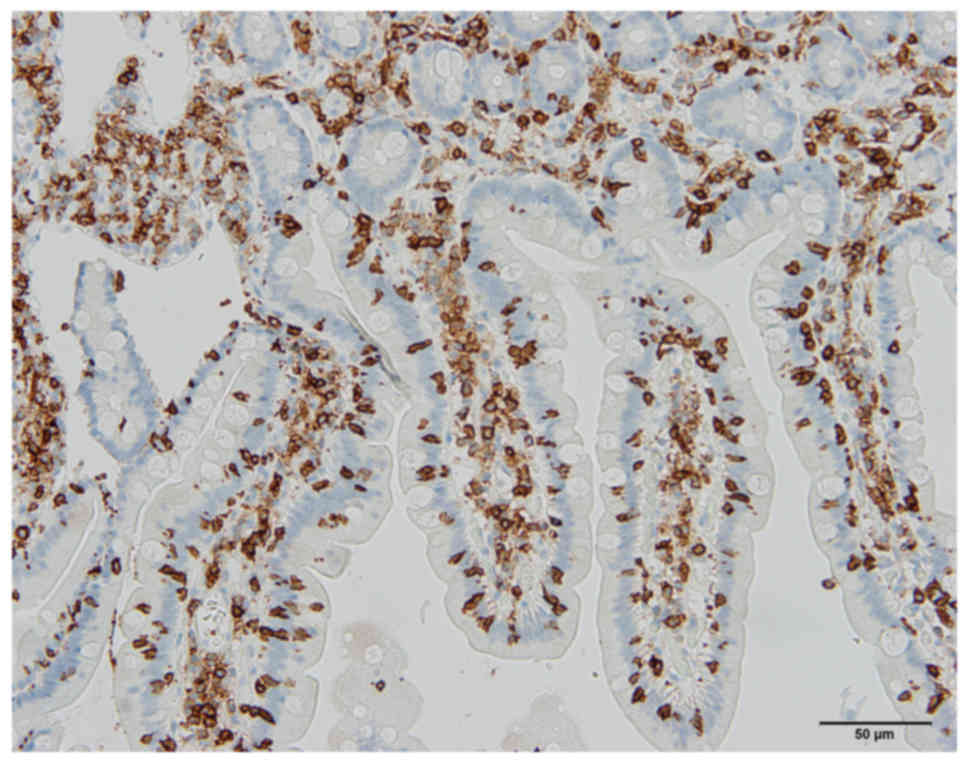
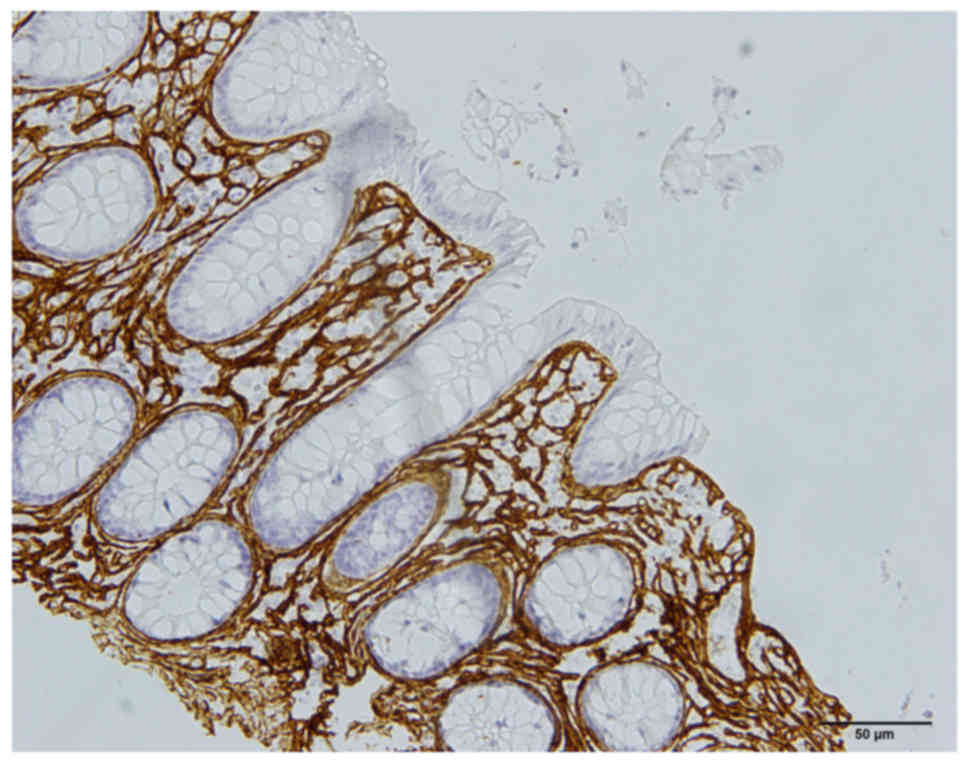
Histopathological examinations of the
macroscopically normal colon showed that two of the IBS-D patients
had collagenous colitis (Fig. 5)
and seven IBS-D patients had lymphocytic colitis. The two patients
with collagenous colitis were males, aged 36 and 42 years, while
those with lymphocytic colitis comprised five females and two males
aged 24, 27, 35, 36, 42, 79, and 82 years.
Applying the Rome III criteria produced a
sensitivity of 100% (95% confidence interval [CI]=99.8–100.0%), a
specificity of 98.7% (95% CI=98.0–99.2), a positive predictive
value of 98.7% (95% CI=98.8–99.2%), and a negative predictive value
of 100% (95% CI=99.7–100.0%). The LR was 74.4%. The calculated +LR
at 76.9 and -LR at 0%.
Clinical data
The five patients with CD adhered to gluten-free
diet, but they still suffered from diarrhea, recurrent abdominal
pain, and abdominal bloating. The histopathology findings for the
duodenal biopsy samples taken during a new gastroscopy were
normal.
The patients with IBD showed IBS symptoms during the
remission period. Similarly, those patients with colon cancer
suffered from IBS symptoms after receiving the surgical treatment
for their carcinoma. All patients with microscopic colitis (MC)
became symptom-free after receiving adequate treatment.
Discussion
Several factors contribute to the high prevalence of
esophagitis such as smoking, overweight, coffee drinking. However,
the present study aimed at investigating the occurrence of
esophagitis in an IBS population not in general population. We
assumed that the occurrence of these factors in the IBS sample
studied is the same as in the background population.
The present investigation is the first study of a
large cohort of European IBS patients to establish the correlation
between esophagitis and IBS. In the cohort of IBS patients studied
here, the prevalence of GERD symptoms was 66%, which agrees well
with the meta-analysis results reported earlier (17). The present study showed further
that the prevalence of GERD symptoms is higher in IBS-C and IBS-M
than that in IBS-D. Although 97% of the IBS patients in this study
had erosive esophagitis, only 66% complained of GERD symptoms. This
may due to that 496 of the patients (33%) took PPI on demand.
However, 506 patients (34%) of the IBS patients included in the
study were asymptomatic despite the esophageal lesions. It is also
probably that IBS symptoms over shadowed the GERD symptoms in the
asymptomatic patients. It is noteworthy that most of the erosive
esophagitis in IBS patients were of grade A. Esophagitis grade A
showed a high interobserver variation (32,33).
However, in this study the endoscopic diagnosis was made by an
experienced single gastroenterologist.
Whereas there is a general agreement that IBS
overlaps with GERD, it is controversial as whether IBS is
associated with non-erosive esophagitis or with erosive
esophagitis. It is noteworthy that studies done on a few IBS
patients in the Western world, showed an association between
erosive esophagitis and IBS (8,19).
In contrast, studies done on Asian IBS patients showed an
association between IBS and non-erosive esophagitis, but not with
erosive esophagitis (7,18). IBS in Asia differs considerably
from that in the Western world (USA and Europe). This difference
includes the prevalence, gender predominance, clinical
presentation, and probably the pathophysiology (34–58).
The difference between patients with IBS in the Western world and
those in Asia may account for the discrepancy in the association of
IBS with non-erosive and erosive esophagitis.
The Rome symptom-based criteria for the diagnosis of
IBS have been validated in several comprehensive reviews and found
to have a modest specificity and reasonable sensitivity (27,59–61).
The Rome criteria were recently validated by latent class analysis
in Canadian and British cohorts comprising 1981 and 360 IBS
patients, respectively (62). In
this model, the sensitivity in the Canadian and British cohorts
were 44.7, and 52.5%, respectively; the corresponding values for
specificity were 85.3 and 84.3% (62), while the +LRs were 3.03 and 3.35,
and the -LRs were 0.65 and 0.56 (62). In the present cohort of about 1 500
Norwegian IBS patients, the application of Rome III criteria
including red flags combined with medical history, normal physical
examination, and normal blood tests yielded sensitivity,
specificity, +LR, and -LR values of 100, 98.7, 76.9, and 0%,
respectively. The Kruis scoring system for the diagnosis of IBS
incorporated symptoms with negative physical findings and normal
laboratory tests (63). Moreover,
combining Rome criteria with red flags, medical history, and
limited diagnostic tests has previously been shown to improve the
diagnostic performance (29,59).
The gastrointestinal organic diseases whose symptoms
overlap those of IBS and which physicians are concerned about
missing when using symptom-based criteria are colorectal cancer,
CD, IBD, MC, bacterial overgrowth, and bile acid malabsorption
(4). It has been reported that
0.02–0.5% of IBS patients diagnosed using symptom-based criteria
had colorectal cancer, while 0.04–4.7% had CD, 0.4–1.9% had IBD,
and 0.7–1.5% had MC (1,3,4,64–83).
This means that 1.2–8.6% of patients suffering from other organic
diseases were misdiagnosed with IBS when applying symptom-based
criteria, which justifies the concerns of clinicians. In the
present study, endoscopic and histopathological examinations of
patients diagnosed using Rome III criteria revealed that 1.4% had
another gastrointestinal organic disease: 0.2, 0.3, 0.3, and 0.6%
had colorectal cancer, CD, IBD, and MC, respectively. It is
noteworthy that all of these patients had the IBS-D subtype. Would
these patients actually be missed in a clinical setting?
The patients with colorectal cancer detected in this
study were suffering from IBS, and the IBS symptoms were the reason
for visiting a doctor; that is, the colon cancer was found
incidentally. All three patients were older than 50 years. The
American College of Gastroenterology and the British Society of
Gastroenterology recommend colonoscopies for individuals aged
>50 years who have IBS symptoms (74,84).
The CD and IBD patients in the present study appeared to have IBS
in addition to their organic diseases. Typically 20–37% of CD
patients exhibit IBS symptoms despite adhering to a gluten-free
diet (85) and are believed to
have IBS in addition to CD (85).
The symptoms in these patients are triggered by the ingestion of
wheat and wheat products, and it is difficult to conclude whether
this is caused by gluten or by the long-sugar-polymer fructans in
wheat (86). This led to the
British Society of Gastroenterology recommending excluding CD in
all patients referred with IBS, and to the American College of
Gastroenterology advising excluding CD in patients with IBS-D or
IBS-M (74,84). Typically 32–39% of patients with
ulcerative colitis and 42–60% of patients with Crohn's disease
suffer from IBS when they are in remission (3,76–81).
The patients with IBD in the present study also suffered from IBS,
and it just happened that they had active disease when the
colonoscopies were performed. None of these patients would have
been misdiagnosed in a clinical setting. In contrast, patients with
MC could be misdiagnosed, and this group of patients should be kept
in mind when symptom-based criteria are used in the diagnosis of
IBS, especially in IBS patients with diarrhea as the predominant
symptom.
It is usual in clinical practice for some IBS
patients to seek health care not because of the symptoms but due to
concerns about possible serious or fatal underlying conditions
(87,88). Whereas negative gastroscopy
findings have been reported to reassure patients with functional
dyspepsia and improve their quality of life, this did not occur for
colonoscopy normal findings in patients with IBS (25). However, the health-care provider is
compelled to accommodate patients who desire endoscopic
examinations for reassurance.
In conclusion, Rome III symptom-based criteria with
red flags, history, negative physical findings, and normal blood
tests perform well in diagnosing IBS. As when applying other
diagnostic methods in the clinic, the overall view of the patient
should also be considered. The Rome Foundation is developing
methods to facilitate the use of Rome criteria in everyday clinic
practices (27). Patients who need
reassurance by performing further examinations should be
accommodated.
Because of the strong association of GERD with IBS,
it has been recommended that physicians who encountered IBS
patients should screen them routinely for the co-existence of GERD
(17). The findings of high
prevalence of erosive esophagitis in IBS patients found here
support this recommendation.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from
Helse-Vest (grant no. 912234), and Helse-Fonna (grant no.
40415).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
MES designed the study, recruited the patients,
obtained the medical histories, and physically examined and
performed gastroscopies and colonoscopies on the IBS patients. MES
also further analyzed the data and drafted the manuscript. OHG and
JGH contributed to the design of the study, analyzed the data, and
reviewed the manuscript.
Ethics approval and consent to
participate
The Regional Committee for Medical and Health
Research Ethics West (Bergen, Norway) waived the need for ethical
approval and the need to obtain consent for the collection,
analysis and publication of the retrospectively obtained and
anonymized data for this non-interventional study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
El-Salhy M: Irritable bowel syndrome:
Diagnosis and pathogenesis. World J Gastroenterol. 18:5151–5163.
2012.PubMed/NCBI
|
|
2
|
El-Salhy M: Recent developments in the
pathophysiology of irritable bowel syndrome. World J Gastroenterol.
21:7621–7636. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
El-Salhy M, Hatlebakk JG, Gilja OH and
Hausken T: Irritable bowel syndrome: Recent developments in
diagnosis, pathophysiology, and treatment. Expert Rev Gastroenterol
Hepatol. 8:435–443. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
El-Salhy M: Recent advances in the
diagnosis of irritable bowel syndrome. Expert Rev Gastroenterol
Hepatol. 9:1161–1174. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Locke GR III, Talley NJ, Fett SL,
Zinsmeister AR and Melton LJ III: Prevalence and clinical spectrum
of gastroesophageal reflux: A population-based study in Olmsted
County, Minnesota. Gastroenterology. 112:1448–1456. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Canavan C, West J and Card T: The
epidemiology of irritable bowel syndrome. Clin Epidemiol. 6:71–80.
2014.PubMed/NCBI
|
|
7
|
Nam SY, Ryu KH and Park BJ: Irritable
bowel syndrome is associated with gastroesophageal reflux symptom
but not erosive esophagitis. J Neurogastroenterol Motil.
19:521–531. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Smart HL, Nicholson DA and Atkinson M:
Gastro-oesophageal reflux in the irritable bowel syndrome. Gut.
27:1127–1131. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lee SY, Lee KJ, Kim SJ and Cho SW:
Prevalence and risk factors for overlaps between gastroesophageal
reflux disease, dyspepsia, and irritable bowel syndrome: A
population-based study. Digestion. 79:196–201. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jung HK, Halder S, McNally M, Locke GR
III, Schleck CD, Zinsmeister AR and Talley NJ; Overlap of
gastro-oesophageal reflux disease, irritable bowel syndrome, :
Prevalence and risk factors in the general population. Aliment
Pharmacol Ther. 26:453–461. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Talley NJ: Overlapping abdominal symptoms:
Why do GERD and IBS often coexist? Drugs Today (Barc). 42 (Suppl
B):S3–S8. 2006.
|
|
12
|
Lembo A, Zaman M, Jones M and Talley NJ:
Influence of genetics on irritable bowel syndrome,
gastro-oesophageal reflux and dyspepsia: A twin study. Aliment
Pharmacol Ther. 25:1343–1350. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cheung TK, Lam KF, Hu WH, Lam CL, Wong WM,
Hui WM, Lai KC, Lam SK and Wong BC: Positive association between
gastro-oesophageal reflux disease and irritable bowel syndrome in a
Chinese population. Aliment Pharmacol Ther. 25:1099–1104. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wu JC, Cheung CM, Wong VW and Sung JJ:
Distinct clinical characteristics between patients with nonerosive
reflux disease and those with reflux esophagitis. Clin
Gastroenterol Hepatol. 5:690–695. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lovell RM and Ford AC: Global prevalence
of and risk factors for irritable bowel syndrome: A meta-analysis.
Clin Gastroenterol Hepatol. 10:712–721 e4. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Noh YW, Jung HK, Kim SE and Jung SA:
Overlap of erosive and non-erosive Reflux diseases with functional
gastrointestinal disorders according to Rome III criteria. J
Neurogastroenterol Motil. 16:148–156. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lovell RM and Ford AC: Prevalence of
gastro-esophageal reflux-type symptoms in individuals with
irritable bowel syndrome in the community: A meta-analysis. Am J
Gastroenterol. 107:1793–1802. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhao Y, Zou D, Wang R, Ma X, Yan X, Man X,
Gao L, Fang J, Yan H, Kang X, et al: Dyspepsia and irritable bowel
syndrome in China: A population-based endoscopy study of prevalence
and impact. Aliment Pharmacol Ther. 32:562–572. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Neumann H, Monkemuller K, Kandulski A and
Malfertheiner P: Dyspepsia and IBS symptoms in patients with NERD,
ERD and Barrett's esophagus. Dig Dis. 26:243–247. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schmulson MJ and Drossman DA: What is new
in Rome IV. J Neurogastroenterol Motil. 23:151–163. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Manning AP, Thompson WG, Heaton KW and
Morris AF: Towards positive diagnosis of the irritable bowel. Br
Med J. 2:653–654. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jellema P, van der Windt DA, Schellevis FG
and van der Horst HE: Systematic review: Accuracy of symptom-based
criteria for diagnosis of irritable bowel syndrome in primary care.
Aliment Pharmacol Ther. 30:695–706. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ford AC, Talley NJ, Veldhuyzen van Zanten
SJ, Vakil NB, Simel DL and Moayyedi P: Will the history and
physical examination help establish that irritable bowel syndrome
is causing this patient's lower gastrointestinal tract symptoms?
JAMA. 300:1793–1805. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Drossman DA: The functional
gastrointestinal disorders and the Rome II process. Gut. 45 (Suppl
2):II1–II5. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lin OS: Colonoscopy in irritable bowel
syndrome: Whom are we reassuring? Gastrointest Endosc. 62:900–902.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Longstreth GF, Thompson WG, Chey WD,
Houghton LA, Mearin F and Spiller RC: Functional bowel disorders.
Gastroenterology. 130:1480–1491. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Whitehead WE, Palsson OS and Simrén M:
Irritable bowel syndrome: What do the new Rome IV diagnostic
guidelines mean for patient management? Expert Rev Gastroenterol
Hepatol. 11:281–283. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pardi DS, Smyrk TC, Tremaine WJ and
Sandborn WJ: Microscopic colitis: A review. Am J Gastroenterol.
97:794–802. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sood R, Camilleri M, Gracie DJ, Gold MJ,
To N, Law GR and Ford AC: Enhancing diagnostic performance of
symptom-based criteria for irritable bowel syndrome by additional
history and limited diagnostic evaluation. Am J Gastroenterol.
111:1446–1454. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Armstrong D, Bennett JR, Blum AL, Dent J,
De Dombal FT, Galmiche JP, Lundell L, Margulies M, Richter JE,
Spechler SJ, et al: The endoscopic assessment of esophagitis: A
progress report on observer agreement. Gastroenterology. 111:85–92.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lundell LR, Dent J, Bennett JR, Blum AL,
Armstrong D, Galmiche JP, Johnson F, Hongo M, Richter JE, Spechler
SJ, et al: Endoscopic assessment of oesophagitis: Clinical and
functional correlates and further validation of the Los Angeles
classification. Gut. 45:172–180. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Takashima T, Iwakiri R, Sakata Y,
Yamaguchi D, Tsuruoka N, Akutagawa K, Komatsu-Tanaka M, Higuchi T,
Tanaka Y, Shimoda R, et al: Endoscopic reflux esophagitis and
Helicobacter pylori infection in young healthy Japanese volunteers.
Digestion. 86:55–58. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gyawali CP, Kahrilas PJ, Savarino E,
Zerbib F, Mion F, Smout AJPM, Vaezi M, Sifrim D, Fox MR, Vela MF,
et al: Modern diagnosis of GERD: The Lyon Consensus. Gut.
67:1351–1362. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Gwee KA, Lu CL and Ghoshal UC:
Epidemiology of irritable bowel syndrome in Asia: Something old,
something new, something borrowed. J Gastroenterol Hepatol.
24:1601–1607. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hoseini-Asl MK and Amra B: Prevalence of
irritable bowel syndrome in Shahrekord, Iran. Indian J
Gastroenterol. 22:215–216. 2003.PubMed/NCBI
|
|
36
|
Shah SS, Bhatia SJ and Mistry FP:
Epidemiology of dyspepsia in the general population in Mumbai.
Indian J Gastroenterol. 20:103–106. 2001.PubMed/NCBI
|
|
37
|
Ghoshal UC, Abraham P, Bhatt C, Choudhuri
G, Bhatia SJ, Shenoy KT, Banka NH, Bose K, Bohidar NP, Chakravartty
K, et al: Epidemiological and clinical profile of irritable bowel
syndrome in India: Report of the Indian Society of Gastroenterology
Task Force. Indian J Gastroenterol. 27:22–28. 2008.PubMed/NCBI
|
|
38
|
Han SH, Lee OY, Bae SC, Lee SH, Chang YK,
Yang SY, Yoon BC, Choi HS, Hahm JS, Lee MH, et al: Prevalence of
irritable bowel syndrome in Korea: Population-based survey using
the Rome II criteria. J Gastroenterol Hepatol. 21:1687–1692. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kwan AC, Hu WH, Chan YK, Yeung YW, Lai TS
and Yuen H: Prevalence of irritable bowel syndrome in Hong Kong. J
Gastroenterol Hepatol. 17:1180–1186. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Husain N, Chaudhry IB, Jafri F, Niaz SK,
Tomenson B and Creed F: A population-based study of irritable bowel
syndrome in a non-Western population. Neurogastroenterol Motil.
20:1022–1029. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Xiong LS, Chen MH, Chen HX, Xu AG, Wang WA
and Hu PJ: A population-based epidemiologic study of irritable
bowel syndrome in South China: Stratified randomized study by
cluster sampling. Aliment Pharmacol Ther. 19:1217–1224. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Chang FY, Lu CL and Chen TS: The current
prevalence of irritable bowel syndrome in Asia. J
Neurogastroenterol Motil. 16:389–400. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Karaman N, Türkay C and Yönem O: Irritable
bowel syndrome prevalence in city center of Sivas. Turk J
Gastroenterol. 14:128–131. 2003.PubMed/NCBI
|
|
44
|
Celebi S, Acik Y, Deveci SE, Bahcecioglu
IH, Ayar A, Demir A and Durukan P: Epidemiological features of
irritable bowel syndrome in a Turkish urban society. J
Gastroenterol Hepatol. 19:738–743. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Masud MA, Hasan M and Khan AK: Irritable
bowel syndrome in a rural community in Bangladesh: Prevalence,
symptoms pattern, and health care seeking behavior. Am J
Gastroenterol. 96:1547–1552. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Quigley EM, Locke GR, Mueller-Lissner S,
Paulo LG, Tytgat GN, Helfrich I and Schaefer E: Prevalence and
management of abdominal cramping and pain: A multinational survey.
Aliment Pharmacol Ther. 24:411–419. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Vandvik PO, Lydersen S and Farup PG:
Prevalence, comorbidity and impact of irritable bowel syndrome in
Norway. Scand J Gastroenterol. 41:650–656. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Drossman DA, Li Z, Andruzzi E, Temple RD,
Talley NJ, Thompson WG, Whitehead WE, Janssens J, Funch-Jensen P,
Corazziari E, et al: U.S. householder survey of functional
gastrointestinal disorders. Prevalence, sociodemography, and health
impact. Dig Dis Sci. 38:1569–1580. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Saito YA, Schoenfeld P and Locke GR III:
The epidemiology of irritable bowel syndrome in North America: A
systematic review. Am J Gastroenterol. 97:1910–1915. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Boekema PJ, van Dam van Isselt EF, Bots ML
and Smout AJ: Functional bowel symptoms in a general Dutch
population and associations with common stimulants. Neth J Med.
59:23–30. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Agréus L, Svärdsudd K, Nyrén O and Tibblin
G: Irritable bowel syndrome and dyspepsia in the general
population: Overlap and lack of stability over time.
Gastroenterology. 109:671–680. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Hillilä MT and Färkkilä MA: Prevalence of
irritable bowel syndrome according to different diagnostic criteria
in a non-selected adult population. Aliment Pharmacol Ther.
20:339–345. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Kay L, Jørgensen T and Jensen KH: The
epidemiology of irritable bowel syndrome in a random population:
Prevalence, incidence, natural history and risk factors. J Intern
Med. 236:23–30. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Thompson WG, Irvine EJ, Pare P, Ferrazzi S
and Rance L: Functional gastrointestinal disorders in Canada: first
population-based survey using Rome II criteria with suggestions for
improving the questionnaire. Dig Dis Sci. 47:225–235. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Boyce PM, Koloski NA and Talley NJ:
Irritable bowel syndrome according to varying diagnostic criteria:
Are the new Rome II criteria unnecessarily restrictive for research
and practice? Am J Gastroenterol. 95:3176–3183. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Mearin F, Badia X, Balboa A, Baró E,
Caldwell E, Cucala M, Díaz-Rubio M, Fueyo A, Ponce J and Roset M:
Irritable bowel syndrome prevalence varies enormously depending on
the employed diagnostic criteria: Comparison of Rome II versus
previous criteria in a general population. Scand J Gastroenterol.
36:1155–1161. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
El-Salhy M, Patcharatrakul T, Hatlebakk
JG, Hausken T, Gilja OH and Gonlachanvit S: Chromogranin A cell
density in the large intestine of Asian and European patients with
irritable bowel syndrome. Scand J Gastroenterol. 52:691–697. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
El-Salhy M, Patcharatrakul T, Hatlebakk
JG, Hausken T, Gilja OH and Gonlachanvit S: Enteroendocrine,
Musashi 1 and neurogenin 3 cells in the large intestine of Thai and
Norwegian patients with irritable bowel syndrome. Scand J
Gastroenterol. 52:1331–1339. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Whitehead WE and Drossman DA: Validation
of symptom-based diagnostic criteria for irritable bowel syndrome:
A critical review. Am J Gastroenterol. 105:814–820; quiz 813, 821.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Moayyedi P and Ford AC: Symptom-based
diagnostic criteria for irritable bowel syndrome: The more things
change, the more they stay the same. Gastroenterol Clin North Am.
40:87–103. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Palsson OS, Whitehead WE, van Tilburg MA,
Chang L, Chey W, Crowell MD, Keefer L, Lembo AJ, Parkman HP, Rao
SS, et al: Rome IV diagnostic questionnaires and tables for
investigators and clinicians. Gastroenterology. Feb 13–2016.(Epub
ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Sood R, Gracie DJ, Gold MJ, To N,
Pinto-Sanchez MI, Bercik P, Moayyedi P, Ford AC and Law GR;
Derivation and validation of a diagnostic test for irritable bowel
syndrome using latent class analysis, : Aliment Pharmacol Ther.
45:824–832. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Kruis W, Thieme C, Weinzierl M, Schüssler
P, Holl J and Paulus W: A diagnostic score for the irritable bowel
syndrome. Its value in the exclusion of organic disease.
Gastroenterology. 87:1–7. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Fasano A, Berti I, Gerarduzzi T, Not T,
Colletti RB, Drago S, Elitsur Y, Green PH, Guandalini S, Hill ID,
et al: Prevalence of celiac disease in at-risk and not-at-risk
groups in the United States: A large multicenter study. Arch Intern
Med. 163:286–292. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
van der Wouden EJ, Nelis GF and Vecht J:
Screening for coeliac disease in patients fulfilling the Rome II
criteria for irritable bowel syndrome in a secondary care hospital
in The Netherlands: A prospective observational study. Gut.
56:444–445. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Locke GR III, Murray JA, Zinsmeister AR,
Melton LJ III and Talley NJ: Celiac disease serology in irritable
bowel syndrome and dyspepsia: a population-based case-control
study. Mayo Clin Proc. 79:476–482. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Hin H, Bird G, Fisher P, Mahy N and Jewell
D: Coeliac disease in primary care: Case finding study. BMJ.
318:164–167. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Shahbazkhani B, Forootan M, Merat S,
Akbari MR, Nasserimoghadam S, Vahedi H and Malekzadeh R: Coeliac
disease presenting with symptoms of irritable bowel syndrome.
Aliment Pharmacol Ther. 18:231–235. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Catassi C, Kryszak D, Louis-Jacques O,
Duerksen DR, Hill I, Crowe SE, Brown AR, Procaccini NJ, Wonderly
BA, Hartley P, et al: Detection of Celiac disease in primary care:
A multicenter case-finding study in North America. Am J
Gastroenterol. 102:1454–1460. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Sanders DS, Carter MJ, Hurlstone DP,
Pearce A, Ward AM, McAlindon ME and Lobo AJ: Association of adult
coeliac disease with irritable bowel syndrome: A case-control study
in patients fulfilling Rome II criteria referred to secondary care.
Lancet. 358:1504–1508. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Korkut E, Bektas M, Oztas E, Kurt M,
Cetinkaya H and Ozden A: The prevalence of celiac disease in
patients fulfilling Rome III criteria for irritable bowel syndrome.
Eur J Intern Med. 21:389–392. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Sanders DS, Patel D, Stephenson TJ, Ward
AM, McCloskey EV, Hadjivassiliou M and Lobo AJ: A primary care
cross-sectional study of undiagnosed adult coeliac disease. Eur J
Gastroenterol Hepatol. 15:407–413. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
El-Salhy M, Lomholt-Beck B and Gundersen
D: The prevalence of celiac disease in patients with irritable
bowel syndrome. Mol Med Report. 4:403–405. 2011.
|
|
74
|
Aziz I and Sanders DS: The irritable bowel
syndrome-celiac disease connection. Gastrointest Endosc Clin N Am.
22:623–637. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Cash BD, Rubenstein JH, Young PE, Gentry
A, Nojkov B, Lee D, Andrews AH, Dobhan R and Chey WD: The
prevalence of celiac disease among patients with nonconstipated
irritable bowel syndrome is similar to controls. Gastroenterology.
141:1187–1193. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Isgar B, Harman M, Kaye MD and Whorwell
PJ: Symptoms of irritable bowel syndrome in ulcerative colitis in
remission. Gut. 24:190–192. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
El-Salhy M, Gundersen D, Gilja OH,
Hatlebakk JG and Hausken T: Is irritable bowel syndrome an organic
disorder? World J Gastroenterol. 20:384–400. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Ansari R, Attari F, Razjouyan H, Etemadi
A, Amjadi H, Merat S and Malekzadeh R: Ulcerative colitis and
irritable bowel syndrome: Relationships with quality of life. Eur J
Gastroenterol Hepatol. 20:46–50. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Simrén M, Axelsson J, Gillberg R,
Abrahamsson H, Svedlund J and Björnsson ES: Quality of life in
inflammatory bowel disease in remission: The impact of IBS-like
symptoms and associated psychological factors. Am J Gastroenterol.
97:389–396. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Keohane J, O'Mahony C, O'Mahony L,
O'Mahony S, Quigley EM and Shanahan F: Irritable bowel
syndrome-type symptoms in patients with inflammatory bowel disease:
A real association or reflection of occult inflammation? Am J
Gastroenterol. 105:1788, 1789–1794; quiz 1795. 2010. View Article : Google Scholar
|
|
81
|
Minderhoud IM, Oldenburg B, Wismeijer JA,
van Berge Henegouwen GP and Smout AJ: IBS-like symptoms in patients
with inflammatory bowel disease in remission; relationships with
quality of life and coping behavior. Dig Dis Sci. 49:469–474. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
82
|
El-Salhy M, Halwe J, Lomholt-Beck B and
Gundersen D: The prevalence of inflammatory bowel diseases,
microscopic colitis, and colorectal cancer in patients with
irritable bowel syndrome. Gastroenterol Insights. 3:e32011.
View Article : Google Scholar
|
|
83
|
Tolliver BA, Herrera JL and DiPalma JA:
Evaluation of patients who meet clinical criteria for irritable
bowel syndrome. Am J Gastroenterol. 89:176–178. 1994.PubMed/NCBI
|
|
84
|
Spiller R, Aziz Q, Creed F, Emmanuel A,
Houghton L, Hungin P, Jones R, Kumar D, Rubin G, Trudgill N, et al:
Guidelines on the irritable bowel syndrome: Mechanisms and
practical management. Gut. 56:1770–1798. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
El-Salhy M, Hatlebakk JG, Gilja OH and
Hausken T: The relation between celiac disease, nonceliac gluten
sensitivity and irritable bowel syndrome. Nutr J. 14:922015.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Heizer WD, Southern S and McGovern S: The
role of diet in symptoms of irritable bowel syndrome in adults: A
narrative review. J Am Diet Assoc. 109:1204–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
O'Sullivan MA, Mahmud N, Kelleher DP,
Lovett E and O'Morain CA: Patient knowledge and educational needs
in irritable bowel syndrome. Eur J Gastroenterol Hepatol. 12:39–43.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Stenner PH, Dancey CP and Watts S: The
understanding of their illness amongst people with irritable bowel
syndrome: A Q methodological study. Soc Sci Med. 51:439–452. 2000.
View Article : Google Scholar : PubMed/NCBI
|