Introduction
Polycystic ovary syndrome (PCOS) is the most common
endocrinological disorder and affects 12–21% of reproductive-aged
women with reproductive, cardiometabolic, and psychological
impacts; however, the mechanism of PCOS development remains unclear
(1–3). It is well established that the major
cause of PCOS pathogenesis, and its associated metabolic disorders,
is hyperandrogenism. A previous study demonstrated that abnormal
expression of cytochrome P450c17α and cytochrome P450 aromatase
(P450arom) has a vital role in local ovarian hyperandrogenism
during PCOS (4). Since insulin
resistance is a common feature of women with PCOS, it is in turn
associated with compensatory hyperinsulinemia, which has an
important role in determining androgen excess production rates. A
large number of researches indicate that glucose transporters
(GLUTs) are responsible for transport of glucose across the plasma
cell membrane, which is the rate-limiting step in glucose
metabolism (5,6). Recent studies have demonstrated that
the changes in GLUT4 expression or translocation in the uterus or
muscle tissues are involved in insulin resistance during PCOS
(7,8). In addition, leptin, which was the
first adipokine to be discovered, has a crucial role in maintaining
food intake and energy balance, and regulates reproduction function
(9–11). Our previous study suggested that
there was a state of chronic low-grade inflammation in the
hypothalamus of PCOS model rats, which may account for central
leptin resistance rats (12). The
exact mechanism of PCOS remains unclear and requires further
research.
Treatment for PCOS involves hormone therapy,
ovulation induction and surgery. Western treatment of PCOS can
promote ovulation, normalize endocrine metabolism, and improve
clinical symptoms (13,14). However, drug dependence or relapse
following use of drugs and toxic side effects of oral medication
greatly limit the clinical use of western medicine (15). Traditional Chinese medicine (TCM),
which originated in China >3,000 years ago, is an important
feature of complementary medicine. From the perspective of TCM,
reproductive function is governed by the kidneys. According to TCM,
the etiology and pathogenesis of PCOS are associated with disorders
of the kidneys, liver and spleen, and kidney deficit (in TCM
terms), is viewed as the primary problem in PCOS (16,17).
Bao Gui capsule (BGC), a Chinese medicinal formula used to treat
PCOS, has been demonstrated to improve hyperandrogenism and insulin
resistance in clinical practice (18,19).
According to the TCM theory, BGC has an important role in the
special therapeutic method of ‘nourishing kidney, strengthening
spleen, removing dampness, dissolving phlegm and eliminating blood
stasis’ (18,19). Sun and Yu (20) reported that BGC has an important
role in central regulation of proopiomelanocortin, neuropeptide Y
and leptin receptor, and reduces serum leptin levels in
androgen-sterilized rat at 9 days old. Although the mechanism of
BGC in treating PCOS remains unclear, studies on patients and
animal model in the past years have demonstrated that BGC may have
a role in regulating the neuro-endocrine-metabolic network
(19,21). Kuek et al (22) report that the effects of BGC on
hyperandrogenism are not as marked as Diane-35, but more effective
than metformin. The effects of BGC on hyperinsulinemia are not as
marked as metformin, but more effective than Diane-35.
The current study was undertaken to observe the
effect of BGC on the expression of P450arom and P450c17α in ovarian
tissues, and the expression of GLUT4 in uterus and muscle tissue of
rats in a PCOS model. Furthermore, regarding the effect of
low-grade chronic inflammation on leptin resistance in PCOS rats,
expression of interleukin (IL)-1β, IL-6, tumor necrosis factor-α
(TNF-α) and nuclear factor-κB kinase subunit β (IKKβ)/nuclear
factor-κB (NF-κB) in the hypothalamus was determined.
Materials and methods
Drugs and preparation
BGC was obtained from the Obstetrics and Gynecology
Hospital of Fudan University (Shanghai, China), and is patented and
approved by Shanghai Food and Drug Administration (no. YZ120296).
BGC is composed of Herba Epimedium, Rhizoma Polygonati, Fructus
Psoraleae, Carapax et Plastrum Testudinis, Radix Rehmanniae,
Rhizoma Anemarrhenae, Radix Angelicae Sinensis, Semen Persicae,
Rhizoma Acori Tatarinowii, Radix Polygoni Cuspidati, Herba Verbenae
Officinalis and Radix Ophiopogonis. It is a hospital prescription
which was produced by Cai Tong De Shanghai Pharmaceutical Co. Ltd.
(http://www.ctdtzy.com/) and termed Tian Gui
Capsule. In 2012 it was renamed Bao Gui Capsule and produced by
Fang Xin Shanghai Pharmaceutical Co. Ltd. (www.fangxinhealth.com). The ingredients of the BGC
capsule were carefully analyzed and quality-controlled by the
manufacturer. Each capsule weighed 0.3 g, which is equivalent to
3.75 g of crude drug. According to the clinical dosage of 5.4 g/60
kg/day, the corresponding dose of BGC tablet for rats was 0.567
g/kg per day (23). The BGC powder
was suspended in solvent [1% carboxymethyl cellulose sodium
(CMC-Na)] and stored at 4°C prior to subsequent use. In the current
study, rats in the low dose (BGC-L) and high dose (BGC-H) groups
received 0.28 and 0.57 g/kg/day BGC by oral gavage once daily for 3
consecutive weeks.
Animals
Inbred female Sprague-Dawley rats (n=39;
6-weeks-old; specific-pathogen free; body weight, 220–240 g) were
purchased from Shanghai Jie Esprit Laboratory Animal Technology
Co., Ltd. [Shanghai, China; animal license no. SCXK (Shanghai)
2013-0006, http://www.jsj-lab.com]. Rats were
housed and experiments were performed at Shanghai Gynecology and
Obstetrics Hospital of Fudan University (Shanghai, China). Rats
were housed in a temperature-controlled room with a 12/12 h
light-dark cycle, with ad libitum access to food and water
in their cages. All experiments in the current study followed the
Criteria of the Medical Laboratory Animal Administrative Committee
of Shanghai and the Guide for Care and Use of Laboratory Animals
(http://www.shanghai.gov.cn/nw2/nw2314/nw2319/nw2407/nw26170/u26aw27198.html),
and were approved by the Institutional Experimental Animals Review
Board of Shanghai Gynecology and Obstetrics Hospital, Fudan
University (No. 20130215).
Grouping and treatment
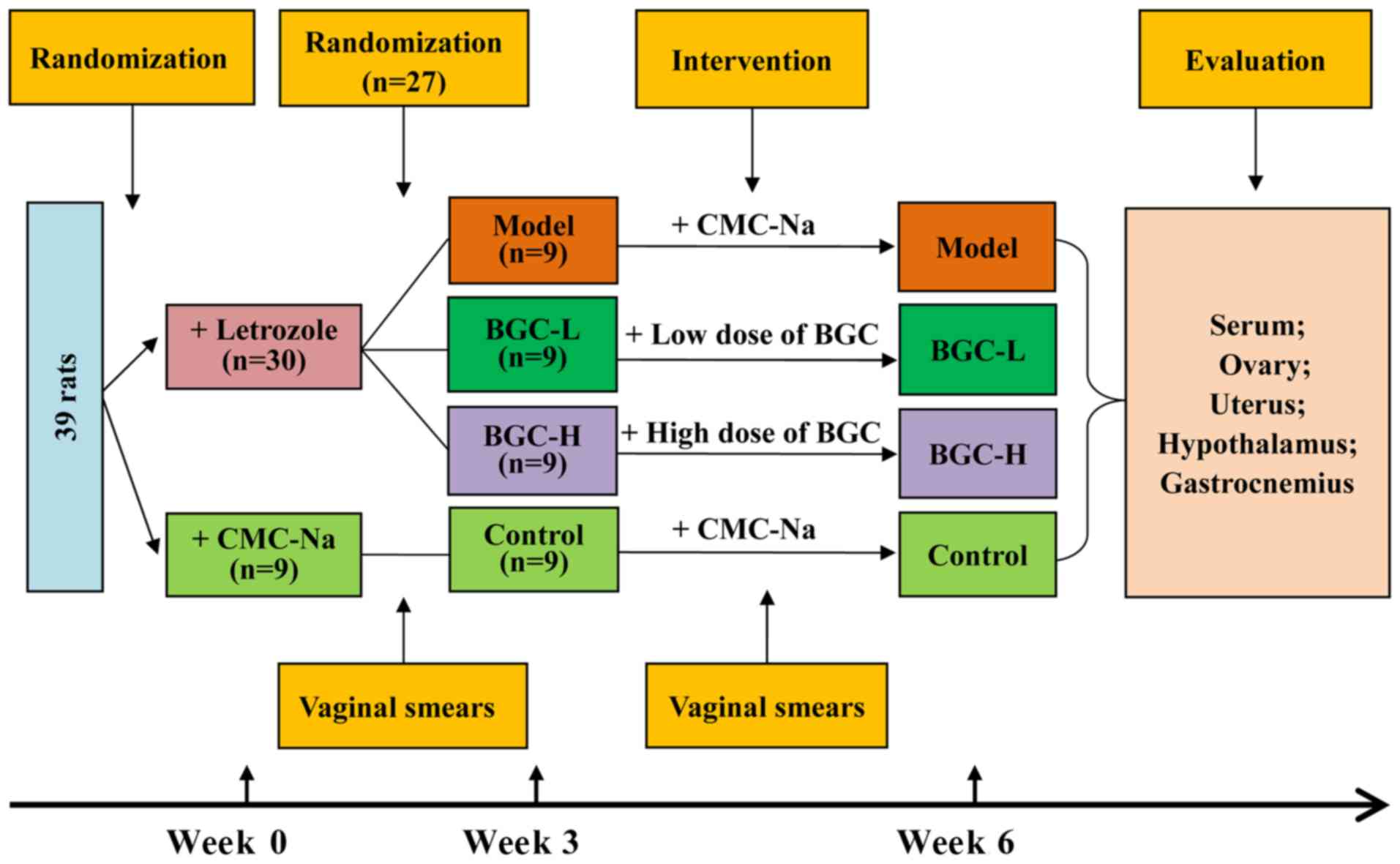
Fig. 1 presents a
schematic diagram illustrating the design of the experiment. After
3 days of acclimatization, 30 rats were administered a gavage of
1.0 mg/kg of letrozole (HengRui Pharmaceutical Factory, Jiangsu,
China, http://www.hrs.com.cn/index.html) solution once daily
for 21 consecutive days to establish the rat model of PCOS, while
the other 9 rats (as the Control group) were treated with an equal
volume of CMC-Na daily for 21 days. Vaginal smears of rats were
taken to determine the successful generation of the PCOS model
rats. The disordered estrous cycle of rats indicated a successful
PCOS rat model. PCOS was successfully induced in 27 rats, which
were randomly divided into three groups as follows: Model group
(n=9), BGC-L (n=9) and BGC-H (n=9). Rats in the BGC-L and BGC-H
group received 0.28 and 0.57 g/kg/day of BGC by oral gavage for 21
days. Rats in the Model and Control group were given an equal
volume of CMC-Na for 21 days. Body weight and vaginal smears were
recorded daily.
Specimen collection
At the end of the 3-week treatment, all rats were
anaesthetized with intraperitoneal injection of pentobarbital (40
mg/kg) and blood (~5–7 ml) was rapidly drawn from the hearts
following an overnight fast. The serum samples were stored at
−20°C. Following euthanasia with an overdose of pentobarbital
sodium (200 mg/kg), the brain were rapidly dissected on ice, then
flash frozen in liquid nitrogen. The hypothalamic region extending
from the organum vasculosum of the lamina terminalis to the arcuate
nucleus was microdissected, and then stored at −80°C. Ovary, uterus
and gastrocnemius tissues of each group were dissected, with half
of each sample immediately put into 4% paraformaldehyde solution
for immunohistochemical analysis, and the remaining tissue stored
at −80°C for subsequent western blot analysis.
ELISA
Four hypothalamus tissues of each group were
collected, and total proteins were extracted in
radioimmunoprecipitation assay (RIPA) buffer (Cell Signaling
Technology, Inc., Danvers, MA, USA) following the manufacturer's
instructions. Serum levels of follicle-stimulating hormone (FSH),
luteinizing hormone (LH), testosterone (T), estradiol
(E2), fasting insulin (INS) and leptin, and IL-1β, IL-6,
TNF-α concentration in hypothalamus tissues, were detected using
ELISA kits according to the manufacturer's protocols (Table S1).
Immunohistochemistry
The samples were fixed in 4% paraformaldehyde over
24 h at 4°C prior to embedding in paraffin blocks, and sliced into
4 µm thick sections. Following routine deparaffinization in xylene,
and rehydration in a graded ethanol series, the sections were
immersed in hematoxylin staining solution (C0107, Beyotime
Institute of Biotechnology) for 5 min at room temperature.
Following rinsing with distilled water, sections were immersed in
Eosin staining solution (C0109, Beyotime Institute of
Biotechnology) for 1 min at room temperature. Then the sections
were dehydrated in ethanol, and mounted with coverslips for
pathological confirmation under a light microscope. Tissue slides
were subjected to antigen retrieval using citric acid (0.1 mol/l)
by being immersed in citric acid and boiling for 15 min using an
800 W microwave oven, and then were left to cool naturally at room
temperature before being washed well in phosphate-buffered saline
(PBS) (10 mmol/l, pH 7.4). The rabbit polyclonal antibodies against
P450c17α (cat. no. ab125022; Abcam, Cambridge, MA, USA; 1:100),
P450arom (cat. no. ab18995; Abcam; 1:200), and GLUT4 (cat. no.
ab654; Abcam; 1:100) used as primary antibodies. Sections were
incubated with primary antibody overnight at 4°C, and then
biotinylated secondary antibody (cat. no. MR-M100; MingRui BioTech,
Co., Ltd., Shanghai, China; 1:300) for 30 min at room temperature.
Diaminobenzidine staining was performed until appropriate for
microscopic examination. The primary antibody was replaced with PBS
for negative control slides. Immunoreactivity staining was
characterized quantitatively by digital image analysis using the
Image Pro-Plus 6.0 (Media Cybernetics, Inc., Rockville, MD,
USA).
Western blot analysis
Following the manufacturer's instructions, total
proteins were extracted using RIPA (Cell Signaling Technology,
Inc.) and protein concentrations were determined using
bicinchoninic acid assay (Beyotime Institute of Biotechnology,
Haimen, China). Following denaturation, protein (40 µg) was
separated by SDS-PAGE on 12% gels and then transferred onto a
nitrocellulose membrane (EMD Millipore, Billerica, MA, USA), which
were blocked in 5% skimmed milk for 1 h at room temperature. The
membranes were incubated overnight at 4°C with specific primary
antibodies. The primary antibody dilutions were 1:1,000 for
antibodies against P450c17α and P450arom, and 1:5,000 for GADPH
(cat. no. ab181603; Abcam). The membranes were subsequently
incubated with a horseradish peroxidase (HRP)-conjugated secondary
antibody (1:10,000, 4414, Cell Signaling Technology, Inc.) for 1 h
at room temperature. Antibody binding was detected by enhanced
chemiluminescence using a Prolight HRP western blotting detection
reagent (cat. no. WBKLS0100; Merck KGaA, Darmstadt, Germany).
Relative band intensities were analyzed using Image Lab software
(version 4.0; Bio-Rad Laboratories, Inc., Hercules, CA, USA).
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA was extracted from hypothalamus tissue
using TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA) according to the manufacturer's instructions.
Purified RNA samples were resuspended in diethypyrocarbonate water.
Then RNA was reverse transcribed in 20 µl total volume using the
Reverse Transcription Reagent kit (Takara Bio, Inc., Dalian, China)
for 60 min at 42°C and 5 min at 70°C. qPCR was performed in an ABI
PRISM 7000HT system (Applied Biosystem; Thermo Fisher Scientific,
Inc.) in triplicates using the SYBR Green Master Mix (Takara Bio,
Inc.). The primers sequences used are presented in Table I. The PCR conditions were as
follows: 15 sec at 95°C, 1 cycle; 5 sec at 95°C and 34 sec at 60°C,
40 cycles. β-actin served as the internal control. The
2−ΔΔCq method was used to calculate the relative mRNA
levels (24).
 | Table I.Primer sequences of target genes. |
Table I.
Primer sequences of target genes.
| Target gene | Primer
sequences | Length (bp) |
|---|
| NF-κB |
5′-TCTTCGACTACGCGGTTACGG-3′ | 21 |
|
|
5′-CTCACGAGCTGAGCATGAAGG-3′ | 21 |
| SOCS3 |
5′-TCAACGGTCACCTGGACTCCTA-3′ | 22 |
|
|
5′-GGTCCAGGAACTCCCGAATG-3′ | 20 |
| IKKβ |
5′-GCACCCTGGCCTTTGAATG-3′ | 19 |
|
|
5′-TCCGTTCAAGTCCTCGCTAACA-3′ | 22 |
| β-actin |
5′-GGAGATTACTGCCCTGGCTCCTA-3′ | 23 |
|
|
5′-GACTCATCGTACTCCTGCTTGCTG-3′ | 24 |
Statistical analysis
Data are expressed as the mean ± standard deviation.
The comparison among four groups was analyzed by one-way analysis
of variance. The least significant difference test was performed to
compare the differences between two groups. All computations were
performed using SPSS 17.0 (SPSS, Inc., Chicago, IL, USA). P<0.05
was considered to indicate a statistically significant
difference.
Results
Effect of BGC treatment on rat body
weight and histology of ovaries
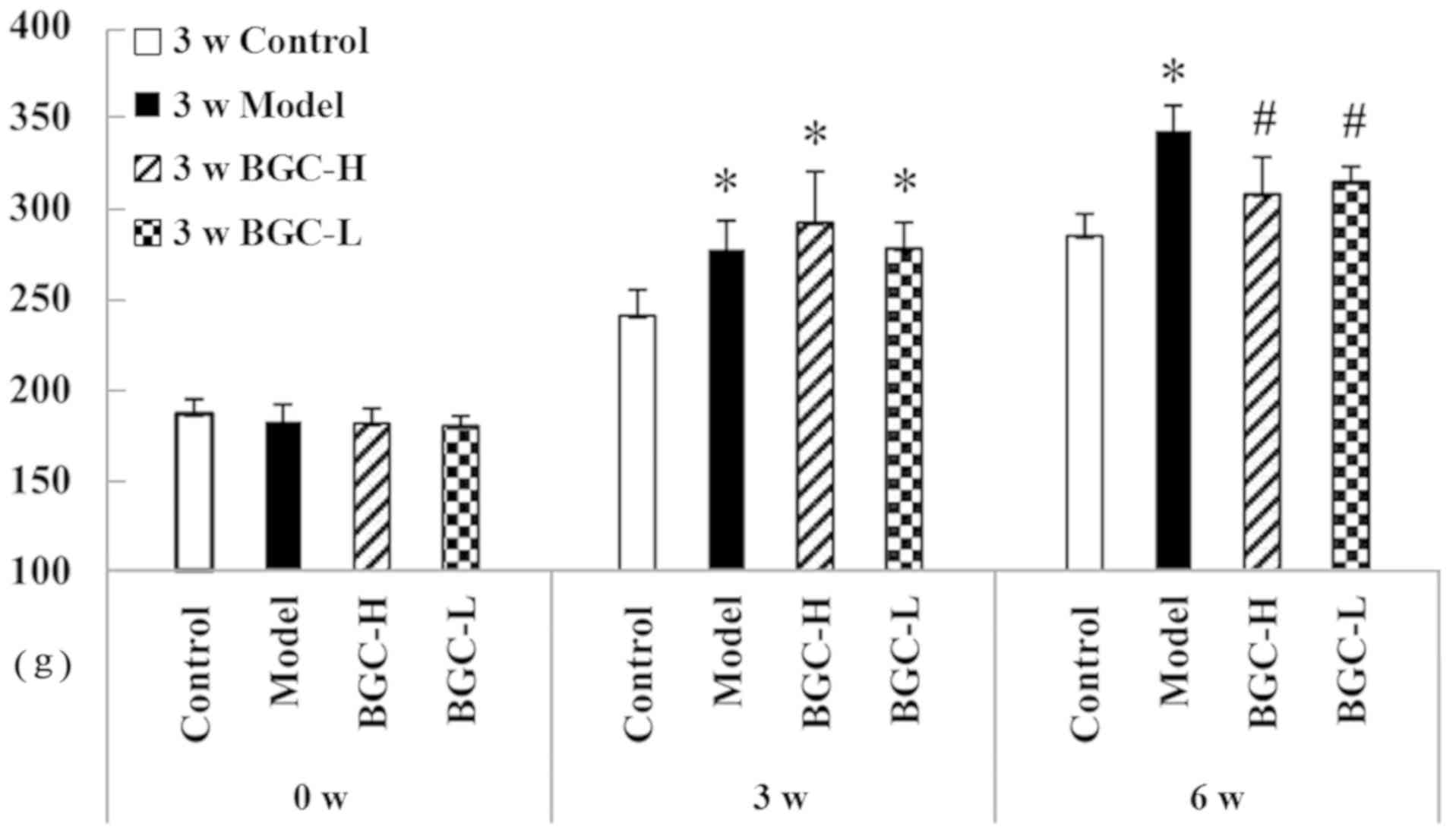
As demonstrated in Fig.
2, there was no difference in body weight among the four groups
before treatment (P>0.05). Rats treated with letrozole gained
significantly more body weight than those treated with CMC-Na after
3 weeks (P<0.05). Treatment with either dose of BGC
significantly decreased body weight compared with those in the
Model group at week 6 (P<0.05).
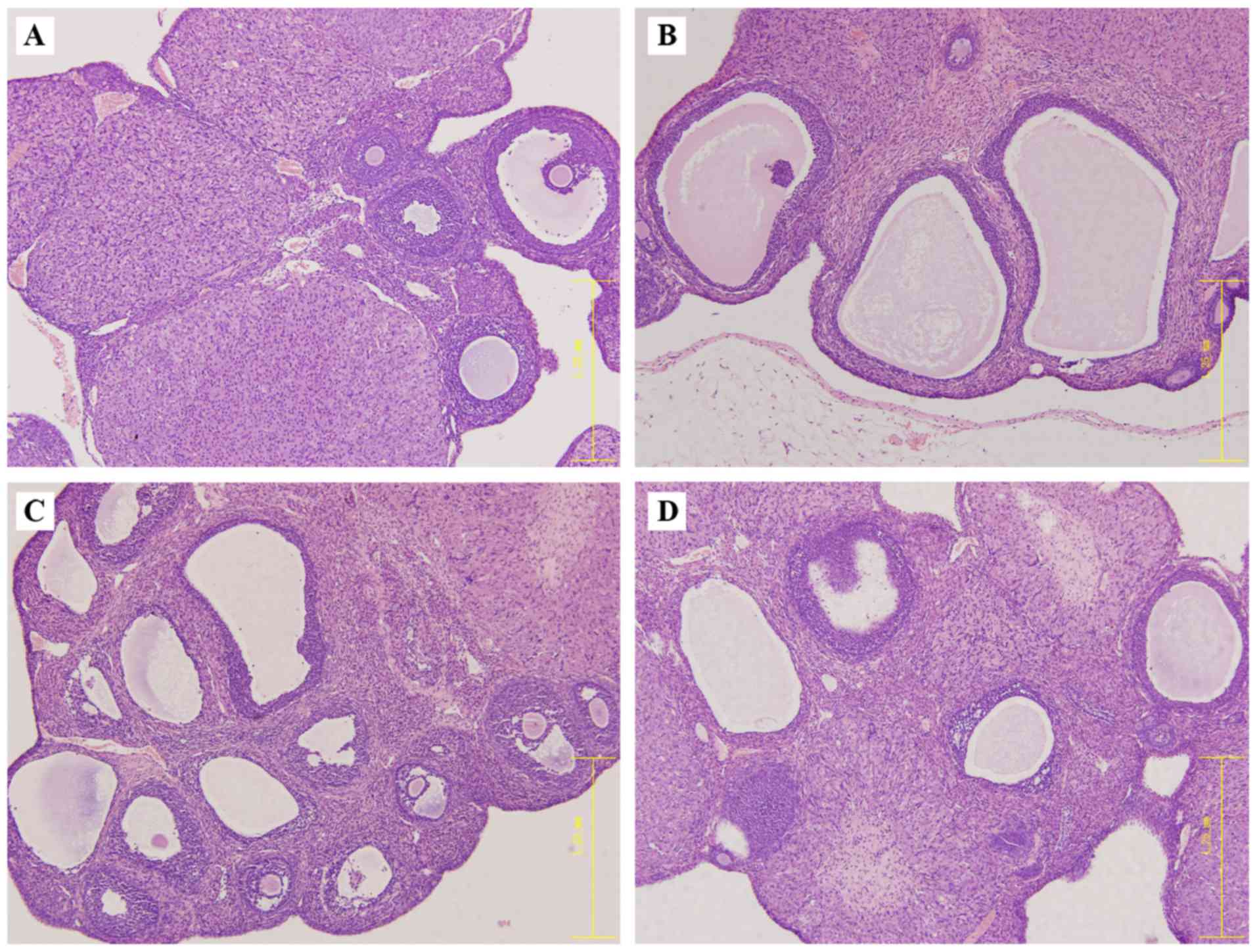
Under light microscopy, follicles of different
developmental stages and a few corpora lutea were observed in the
Control group (Fig. 3A). In the
PCOS group, there were many follicles with saccular dilatation, and
fewer layers of granular cells and thickening surface albuginea
(Fig. 3B). The ovaries of rats
treated with BGC exhibited increased granular cell layers,
decreased dilated follicles, and increased corpus luteum compared
with the PCOS model group (Fig. 3C and
D).
Effect of BGC treatment on the serum
levels of LH/FSH, T, logT/E2, insulin and leptin, and
the estrous cycle
Serum LH/FSH, T, logT/E2, insulin and
leptin concentrations were significantly higher in the Model group
compared with the Control group (P<0.05; Fig. 4A-E). Compared with the Model group,
the serum levels of LH/FSH, T, logT/E2, insulin and
leptin were significantly reduced in rats treated with the low and
high dose of BGC (P<0.05; Fig.
4A-E). The results of vaginal smears indicated that estrous
cycles of rat were routine in the Control group, comprising
proestrus, estrus, metestrus and diestrus. Rats experienced
prolonged diestrus beginning on the day 11 after the letrozole
gavage. Of 30 rats, 27 exhibited vaginal keratosis and an irregular
estrous cycle at week 3, suggesting the successful induction of
PCOS. Following 6 weeks of letrozole, only 1 of 9 rats in the Model
group demonstrated a regular estrous cycle. In the BGC-L and BGC-H
groups, 5 and 6 of the 9 rats exhibited recovered estrous cycles,
respectively. The recovery rates in the Model, BGC-L, and BGC-H
groups were 11.11, 55.56 and 66.67%, respectively (Fig. 4F).
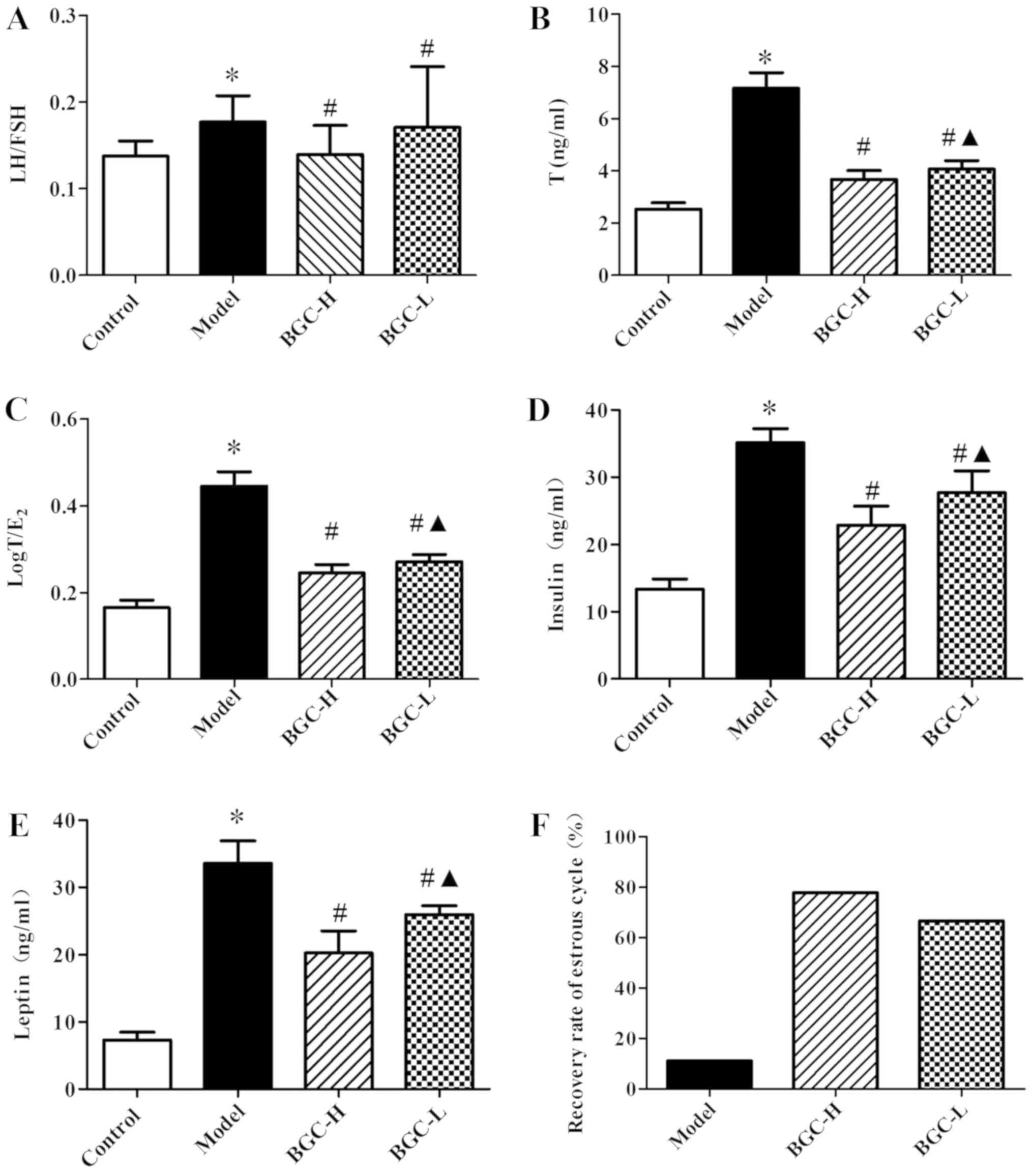 | Figure 4.Effects of BGC on serum concentrations
of LH/FSH, T, log T/E2, insulin, leptin and effects on
estrous cycle. Serum levels of (A) LH/FSH, (B) T, (C) log
T/E2, (D) insulin, (E) leptin and (F) estrous cycle
(n=9). Data are expressed as the mean ± standard deviation (n=9).
*P<0.05 vs. Control group. #P<0.05 vs. Model
group. ▲P<0.05 vs. BGC-H group. FSH,
follicle-stimulating hormone; BGC, Bao Gui capsule; BGC-L, low
dose; BGC-H, high dose; LH, luteinizing hormone; T, testosterone;
E2, estradiol; INS, fasting insulin. |
Effect of BGC treatment on the
expression of P450c17α and P450arom in ovarian tissues
As presented in Fig. 5A
and B, increased immunostaining of P450c17α and decreased
immunostaining of P450arom were observed in the ovarian granulosa
cells of rats in the Model group compared with rats in the Control
group (P<0.05). Treatment with BGC reduced expression of
P450c17α and increased expression of P450arom in the ovarian
granulosa cells of PCOS model rats (P<0.05).
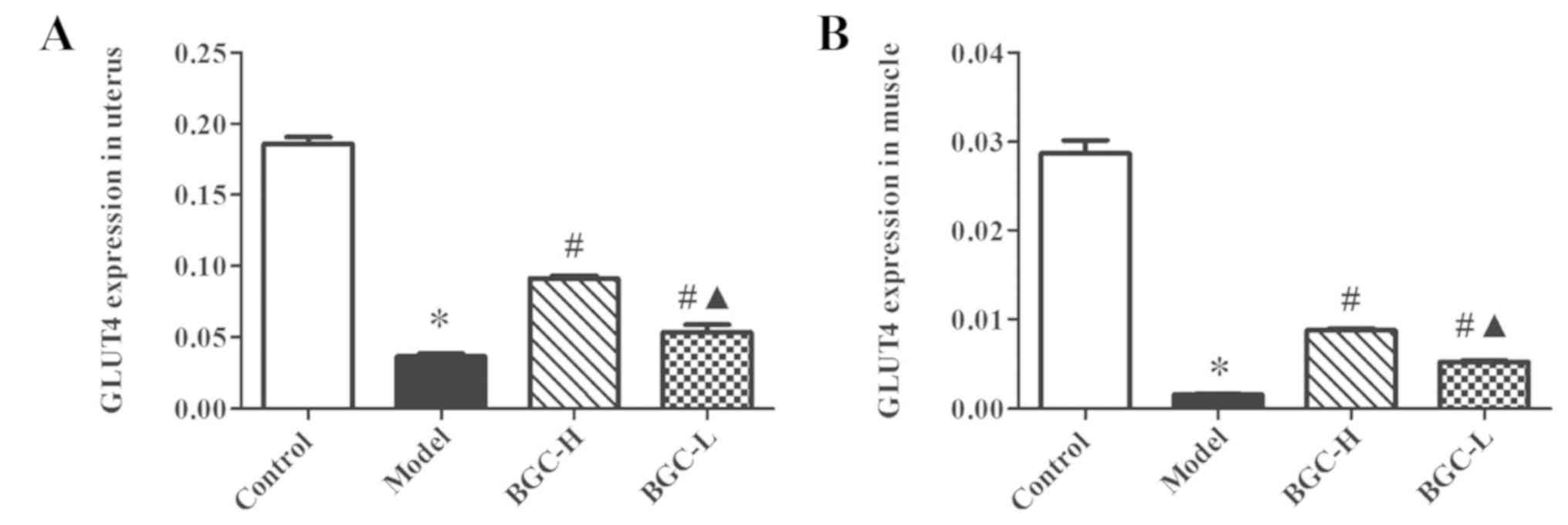
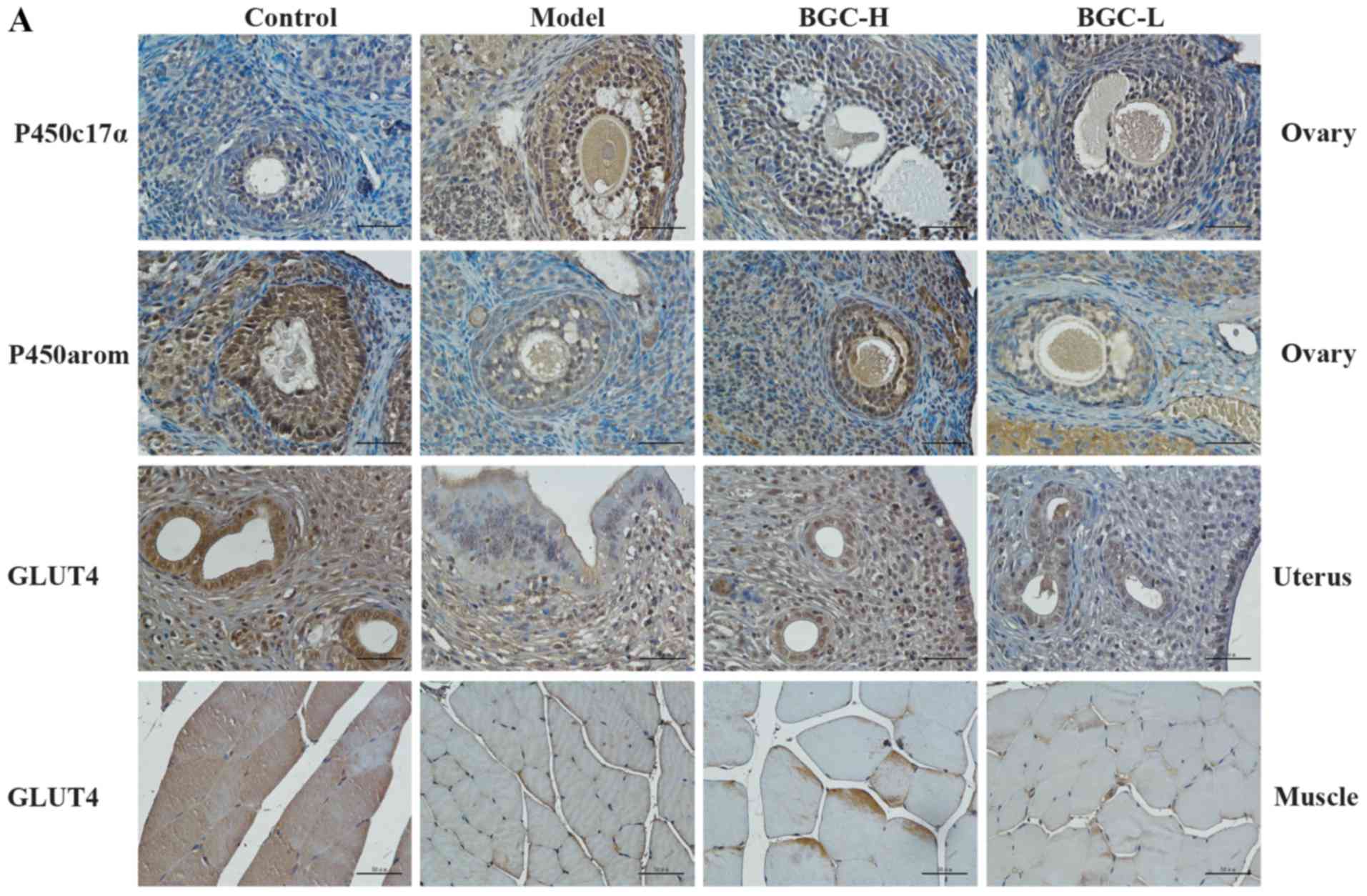 | Figure 5.Effects of BGC on the expression of
P450c17α and P450arom in ovarian tissues, and GLUT4 in uterus and
muscle tissues analyzed by immunohistochemistry. (A)
Immunohistochemical staining of P450c17α and P450arom in ovarian
tissues, and GLUT4 in uterus and muscle tissues (magnification,
×400). Statistical analysis of the protein expression of (B)
P450c17α and (C) P450arom in ovarian tissues, and GLUT4 in (D)
uterus and (E) muscle tissue.. Data are expressed as the mean ±
standard deviation (n=9). *P<0.05 vs. Control group.
#P<0.05 vs. Model group. ▲P<0.05 vs.
BGC-H group. BGC, Bao Gui capsule; BGC-L, low dose; BGC-H, high
dose; P450c17α, cytochrome P450c17α; P450arom, cytochrome P450
aromatase; GLUT4, glucose transporter 4. |
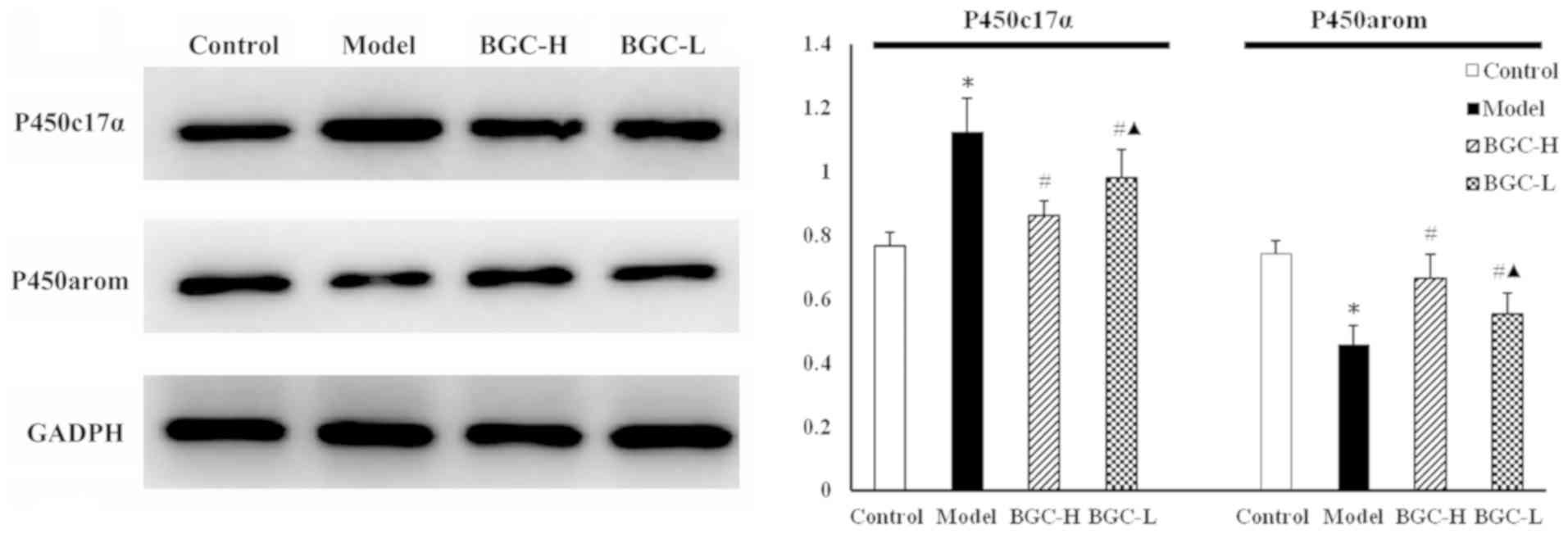
Furthermore, the protein levels of P450c17α and
P450arom in the ovarian tissues were assessed via western blot
analysis (Fig. 6). The protein
expression exhibited a tendency similar to the immunohistochemical
staining results.
BGC treatment increased the expression
of GLUT4 in uterus and muscle tissues
Compared with the Control group, the expression of
GLUT4 in uterus and muscle tissues were significantly decreased in
the Model group (P<0.05). The expression of GLUT4 was
significantly increased in low dose and high dose BGC treatment
groups compared with the Model group (P<0.05; Fig. 7).
BGC treatment reduces low-grade
chronic inflammation in the hypothalamus and may improve central
leptin resistance
The protein levels of IL-1β, IL-6 and TNF-α in the
hypothalamus were determined via ELISA. The IL-1β, IL-6 and TNF-α
concentrations in the hypothalamus were significantly increased in
the Model group compared with the Control group (P<0.05).
Compared with the Model group, the protein levels of IL-6 and TNF-α
were significantly decreased in BGC-H group in a dose-dependent
manner (P<0.05, Fig. 8A-C).
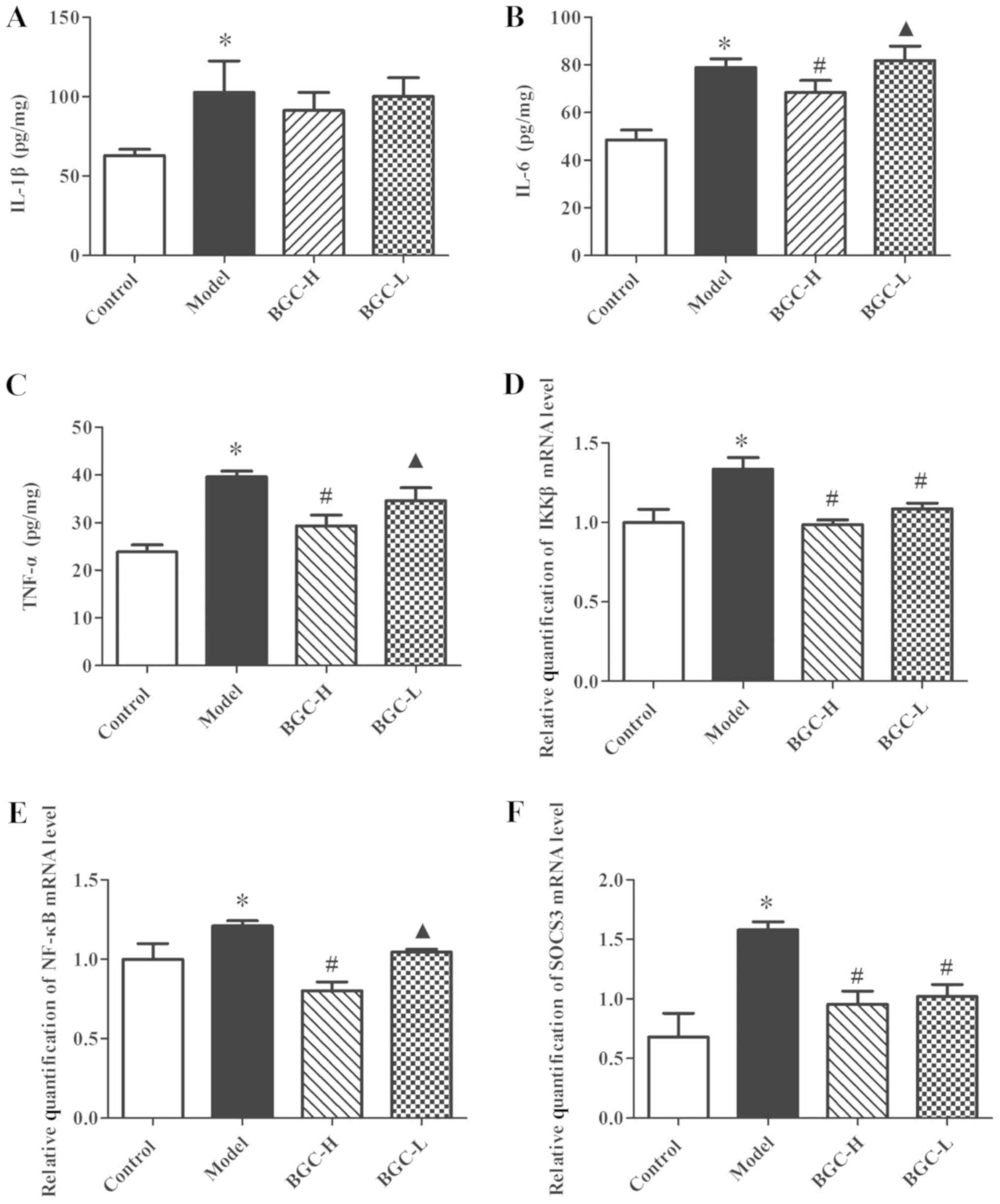 | Figure 8.Effects of BGC on protein levels of
IL-1β, IL-6 and TNF-α in the hypothalamus, and mRNA expressions of
NF-κB, IKKβ and SOCS3 in hypothalamus. Protein concentrations of
(A) IL-1β, (B) IL-6 and (C) TNF-α in hypothalamus were determined
by ELISA (n=4). (D) IKKβ, (E) NF-κB and (F) SOCS3 mRNA levels of
hypothalamus were determined by reverse transcription-quantitative
polymerase chain reaction (n=4). Data are expressed as the mean ±
standard deviation. *P<0.05 vs. Control group.
#P<0.05 vs. Model group. ▲P<0.05 vs.
BGC-H group. IL, interleukin; TNF-α, tumor necrosis factor-α; IKKβ,
nuclear factor-κB kinase subunit β; NF-κB, nuclear factor-κB;
SOCS3, suppressor of cytokine signaling 3. |
Additionally, NF-κB, IKKβ and suppressor of cytokine
signaling 3 (SOCS3) mRNA levels in the hypothalamus were examined.
NF-κB, IKKβ and SOCS3 mRNA levels in the hypothalamus were markedly
increased in the Model group compared with the Control group, and
were significantly decreased in the low dose and high dose BGC
treatment groups (P<0.05; Fig.
8D-F).
Discussion
In the present study, serum LH/FSH, T,
logT/E2, insulin and leptin concentrations were
significantly higher in the Model group compared with the Control
group. Despite the observed increase in log T/E2 in the
Model group, the level of estradiol was observed to be
significantly decreased in the Model group compared with the
Control group rats (Fig. S1). The
species difference of changes of estradiol level between human and
rat with PCOS, and the less number of rats in each group are
probably the main reason, for the experiment results above. BGC has
been used as a prescription since 2006, and is produced as a
patented medicine and widely used as PCOS medication. Clinically,
patients usually take BGC for at least three menstrual cycles
(23). As the estrous cycle of
rats is 4–5 days, BGC administration for three weeks was equivalent
to patients taking BGC for at least three menstrual cycle. In the
present study, BGC reduced LH/FSH, T, logT/E2, insulin
and leptin. Additionally, BGC markedly reduced body weight gain,
decreased the expression of P450c17α in ovaries, significantly
increased the expression of P450arom in ovaries, and the expression
of GLUT4 in uterus and muscle tissues. Furthermore, BGC effectively
reduced the level of IL-1β, IL-6 and TNF-α, and the expression of
IKKβ, NF-κB and SOCS3 in the hypothalamus of PCOS model rats.
It is established that increased androgen levels,
which appear to be the result of dysregulation of steroidogenesis
within the ovaries and adrenal glands, is the main pathological
feature of PCOS. P450c17α, which possesses 17-hydroxylase and 17,
20-lyase activities, is considered to be the rate-limiting enzyme
in the formation of androgens (25–27).
P450arom induces the conversion of androstenedione and testosterone
into estradiol and estrone in granulosa cells. P450arom-catalysed
estrogen synthesis is a key event during the final stage of ovarian
follicular development (28).
Decreased expression of P450arom or increased expression of
P450c17α induces hyperandrogenism in patients with PCOS. In the
current study, reduced expression of P450c17α and increased
expression of P450arom were observed in ovarian tissues following
BCG treatment. Thus, BGC improved the local ovarian environment of
excessive androgens by altering the expression of P450arom and
P450c17α, which may further improve the reproductive, endocrine and
metabolic disorder associated with PCOS.
The translocation of GLUT4 vesicles from
intracellular deposits to the plasma membrane, which is stimulated
by insulin or muscle contractions, has a vital role in glucose
homeostasis. In skeletal muscle and adipocytes, dysregulation of
GLUT4 translocation is closely associated with insulin resistance.
Furthermore, based on the fact that glucose uptake and utilization
have a vital role in implantation, embryonic development and
pregnancy, an increasing number of studies have that steroid
hormone-dependent regulation of GLUT4 expression may be involved in
the mechanism of PCOS-induced endometrial disorders of the
menstrual cycle and endometrial receptivity (7,8,29).
In the present study, BGC treatment significantly increased the
expression of GLUT4 in uterus and muscle tissues, which suggests
that BGC may improve insulin resistance and endometrial
receptivity.
Our previous study revealed central leptin
resistance and low-grade chronic inflammation in the hypothalamus
of PCOS rats (12). In the current
study, the protein level of IL-1β, IL-6 and TNF-α, and the mRNA
expression of IKKβ, NF-κB and SOCS3 in the hypothalamus were
significantly increased in Model group rats compared with the
Control group, which was consistent with our previous conclusions.
IKKβ/NF-κB signaling has been identified as one of the key
proinflammatory pathway that atypically mediates chronic low-grade
nutritionally-induced inflammation and causes various metabolic
dysfunctions (30–32). Recent research indicated that
overnutrition activates IKKβ/NF-κB in the hypothalamus, and
furthermore, inhibition of IKKβ/NF-κB in the hypothalamus
suppresses appetite and prevents obesity (33,34).
SOCS3 has a crucial role in mediating the effects of hypothalamic
IKKβ/NF-κB on leptin resistance (35,36).
Our previous study (12)
demonstrated that central icv injection of leptin decreased 24 h
food intake and body weight gain, and induced increasing expression
of p-STAT3 in the hypothalamus of control group rats. However,
central icv injection of leptin did not exert an effect on 24 h
food intake, body weight, and p-STAT3 expression in rats of PCOS
group, suggesting that central leptin resistance was present in the
PCOS rats induced by letrozole. Furthermore, inflammatory markers
were upregulated in the hypothalami of PCOS rats, indicating that
there was a state of chronic low-grade inflammation in the
hypothalamus, which may be the potential mechanism of central
leptin resistance in PCOS rats (12). In the present study, BGC may have
improved central leptin resistance of PCOS rats by decreasing the
protein levels of IL-6 and TNF-α, and the mRNA expression of IKKβ,
NF-κB and SOCS3 in hypothalamus of PCOS rats, which may partially
explain the therapeutic effects.
In summary, the results of the current study
demonstrate that BGC treatment may effectively improve
hyperandrogenism by decreasing the expression of P450c17α and
raising the expression of P450arom in ovarian tissues.
Additionally, BGC treatment may improve insulin resistance and
endometrial receptivity by increasing the expression of GLUT4 in
uterus and muscle tissues. Furthermore, the current study provides
the first description that BGC treatment may improve low-grade
chronic inflammation in the hypothalamus, and may improve central
leptin resistance in PCOS rats. Thus, BGC may be a promising TCM
therapy for the treatment of PCOS. Further clinical trials are
required to confirm its efficacy in the future.
Supplementary Material
Supporting Data
Acknowledgements
The authors thank Mr. Pinli Chen from Obstetrics and
Gynecology Hospital, Fudan University, Shanghai, China and Dr Xing
Tan from Department of Physiology and Center of Polar Medical
Research, Second Military Medical University, Shanghai, China for
their generous assistance in surgery and the preparation of
specimens.
Funding
The study was supported by a grant from The Science
and Technology Commission of Shanghai Municipality (grant no.
11DZ1971900).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article and/or its supplementary
materials.
Authors' contributions
WW conceived and designed the study. YL and FZ
performed the experiments. YL wrote the manuscript.
Ethics approval and consent to
participate
All experiments in the current study followed the
Criteria of the Medical Laboratory Animal Administrative Committee
of Shanghai and the Guide for Care and Use of Laboratory Animals,
and were approved by the Institutional Experimental Animals Review
Board of Shanghai Gynaecology and Obstetrics Hospital, Fudan
University (no. 20130215).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PCOS
|
polycystic ovary syndrome
|
|
GLUTs
|
glucose transporters
|
|
P450arom
|
cytochrome P450 aromatase
|
|
BGC
|
Bao Gui capsule
|
References
|
1
|
March WA, Moore VM, Willson KJ, Phillips
DI, Norman RJ and Davies MJ: The prevalence of polycystic ovary
syndrome in a community sample assessed under contrasting
diagnostic criteria. Hum Reprod. 25:544–551. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Teede HJ, Misso ML, Deeks AA, Moran LJ,
Stuckey BG, Wong JL, Norman RJ and Costello MF; Guideline
Development Groups, : Assessment and management of polycystic ovary
syndrome: Summary of an evidence-based guideline. Med J Aust.
195:S65–S112. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Moran LJ, Misso ML, Wild RA and Norman RJ:
Impaired glucose tolerance, type 2 diabetes and metabolic syndrome
in polycystic ovary syndrome: A systematic review and
meta-analysis. Hum Reprod Update. 16:347–363. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Qin KN and Rosenfield RL: Role of
cytochrome P450c17 in polycystic ovary syndrome. Mol Cell
Endocrinol. 145:111–121. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Garvey WT, Maianu L, Hancock JA,
Golichowski AM and Baron A: Gene-expression of GLUT4 in
skeletal-muscle from insulin-resistant patients with obesity, IGT,
GDM, and NIDDM. Diabetes. 41:465–475. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shepherd PR and Kahn BB: Glucose
transporters and insulin action-implications for insulin resistance
and diabetes mellitus. N Engl J Med. 341:248–257. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mioni R, Chiarelli S, Xamin N, Zuliani L,
Granzotto M, Mozzanega B, Maffei P, Martini C, Blandamura S, Sicolo
N and Vettor R: Evidence for the presence of glucose transporter 4
in the endometrium and its regulation in polycystic ovary syndrome
patients. J Clin Endocrinol Metab. 89:4089–4096. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Frolova AI and Moley KH: Glucose
transporters in the uterus: An analysis of tissue distribution and
proposed physiological roles. Reproduction. 142:211–220. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Trayhurn P and Beattie JH: Physiological
role of adipose tissue: White adipose tissue as an endocrine and
secretory organ. Proc Nutr Soc. 60:329–339. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sainz N, Gonzalez-Navarro CJ, Martinez JA
and Moreno-Aliaga MJ: Leptin signaling as a therapeutic target of
obesity. Expert Opin Ther Targets. 19:893–909. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pusalkar M, Meherji P, Gokral J,
Savardekar L, Chinnaraj S and Maitra A: Obesity and polycystic
ovary syndrome: Association with androgens, leptin and its
genotypes. Gynecol Endocrinol. 26:874–882. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lian Y, Zhao F and Wang W: Central leptin
resistance and hypothalamic inflammation are involved in
letrozole-induced polycystic ovary syndrome rats. Biochem Biophys
Res Commun. 476:306–312. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Prelevic GM, Puzigaca Z and Balint-Peric
LA: Effects of an oral contraceptive containing cyproterone acetate
(Diane-35) on the symptoms, hormone profile, and ovarian volume of
hirsute women with polycystic ovarian syndrome. Ann N Y Acad Sci.
687:255–262. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Palomba S, Falbo A, Russo T, Orio F,
Tolino A and Zullo F: Systemic and local effects of metformin
administration in patients with polycystic ovary syndrome (PCOS):
Relationship to the ovulatory response. Hum Reprod. 25:1005–1013.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Spritzer PM, Motta AB, Sir-Petermann T and
Diamanti-Kandarakis E: Novel strategies in the management of
polycystic ovary syndrome. Minerva Endocrinol. 40:195–212.
2015.PubMed/NCBI
|
|
16
|
Raja-Khan N, Stener-Victorin E, Wu X and
Legro RS: The physiological basis of complementary and alternative
medicines for polycystic ovary syndrome. Am J Physiol Endocrinol
Metab. 301:E1–E10. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhou J and Qu F: Treating gynaecological
disorders with traditional Chinese medicine: A review. Afr J Tradit
Complement Altern Med. 6:494–517. 2009.PubMed/NCBI
|
|
18
|
Zhou LR and Yu J: Clinical observation on
treatment of hyperinsulinemia and hyperandrogenism anovulatory
patient with replenishing kidney-yin drugs. Zhongguo Zhong Xi Yi
Jie He Za Zhi. 16:515–518. 1996.(In Chinese). PubMed/NCBI
|
|
19
|
Hou J, Yu J and Wei M: Study on treatment
of hyperandrogenism and hyperinsulinism in polycystic ovary
syndrome with Chinese herbal formula ‘tiangui fang’. Zhongguo Zhong
Xi Yi Jie He Za Zhi. 20:589–592. 2000.(In Chinese). PubMed/NCBI
|
|
20
|
Sun F and Yu J: Effect of tiangui recipe
on serum leptin and pituitary gonadotropin in androgen-sterilized
rats. Zhongguo Zhong Xi Yi Jie He Za Zhi. 19:350–352. 1999.(In
Chinese). PubMed/NCBI
|
|
21
|
Yu J and Cheng HY: Experimental studies on
the relation of the kidney and reproduction. Zhong Xi Yi Jie He Za
Zhi. 9548–551. (517)1989.(In Chinese). PubMed/NCBI
|
|
22
|
Kuek S, Wang WJ and Gui SQ: Efficacy of
Chinese patent medicine Tian Gui Capsule in patients with
polycystic ovary syndrome: A randomized controlled trial. Zhong Xi
Yi Jie He Xue Bao. 9:965–972. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang XJ, Chen YQ, Gui SQ, Qian QH and Guo
SX: Clinical observation on Tiangui Capsule for 110 cases of
polycystic ovary syndrome. J Trad Chin Med. 55:1835–1840. 2014.(In
Chinese).
|
|
24
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fan YS, Sasi R, Lee C, Winter JS, Waterman
MR and Lin CC: Localization of the human CYP17 gene (cytochrome
P450(17alpha) to 10q24.3 by fluorescence in situ hybridization and
simultaneous chromosome banding. Genomics. 14:1110–1111. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
McNatty KP, Makris A, DeGrazia C,
Osathanondh R and Ryan KJ: The production of progesterone,
androgens, and estrogens by granulosa cells, thecal tissue, and
stromal tissue from human ovaries in vitro. J Clin Endocrinol
Metab. 49:687–699. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Moon YS, Tsang BK, Simpson C and Armstrong
DT: 17beta-Estradiol biosynthesis in cultured granulosa and thecal
cells of human ovarian follicles: Stimulation by
follicle-stimulating hormone. J Clin Endocrinol Metab. 47:263–267.
1978. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Harlow CR, Bradshaw AC, Rae MT, Shearer KD
and Hillier SG: Oestrogen formation and connective tissue growth
factor expression in rat granulosa cells. J Endocrinol. 192:41–52.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Schulte MM, Tsai JH and Moley KH: Obesity
and PCOS: The effect of metabolic derangements on endometrial
receptivity at the time of implantation. Reprod Sci. 22:6–14. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cai D, Yuan M, Frantz DF, Melendez PA,
Hansen L, Lee J and Shoelson SE: Local and systemic insulin
resistance resulting from hepatic activation of IKK-beta and
NF-kappaB. Nat Med. 11:183–190. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cai D, Frantz JD, Tawa NE Jr, Melendez PA,
Oh BC, Lidov HG, Hasselgren PO, Frontera WR, Lee J, Glass DJ and
Shoelson SE: IKKbeta/NF-kappaB activation causes severe muscle
wasting in mice. Cell. 119:285–298. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yuan M, Konstantopoulos N, Lee J, Hansen
L, Li ZW, Karin M and Shoelson SE: Reversal of obesity- and
diet-induced insulin resistance with salicylates or targeted
disruption of IKKbeta. Science. 293:1673–1677. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang X, Zhang G, Zhang H, Karin M, Bai H
and Cai D: Hypothalamic IKKbeta/NF-kappaB and er stress link
overnutrition to energy imbalance and obesity. Cell. 135:61–73.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Benzler J, Ganjam GK, Pretz D, Oelkrug R,
Koch CE, Legler K, Stöhr S, Culmsee C, Williams LM and Tups A:
Central inhibition of IKKβ/NF-κB signaling attenuates high-fat
diet-induced obesity and glucose intolerance. Diabetes.
64:2015–2027. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mori H, Hanada R, Hanada T, Aki D, Mashima
R, Nishinakamura H, Torisu T, Chien KR, Yasukawa H and Yoshimura A:
Socs3 deficiency in the brain elevates leptin sensitivity and
confers resistance to diet-induced obesity. Nat Med. 10:739–743.
2004. View
Article : Google Scholar : PubMed/NCBI
|
|
36
|
Howard JK, Cave BJ, Oksanen LJ, Tzameli I,
Bjorbaek C and Flier JS: Enhanced leptin sensitivity and
attenuation of diet-induced obesity in mice with haploinsufficiency
of Socs3. Nat Med. 10:734–738. 2004. View
Article : Google Scholar : PubMed/NCBI
|