Introduction
The incidence of non-small cell lung cancer (NSCLC)
increases with age, with 60% of cases arising in patients over 60
years of age, and 30–40% in patients of 70 years or older (1,2). In
developed countries the median age of diagnosis for advanced
disease is 68 years (3), but this
has increased notably over the last 3 decades. Consequently, the
age of the patient is often a major factor for physicians
considering treatment options for patients with advanced NSCLC.
Elderly patients are often denied therapy, prematurely discontinued
and excluded from clinical trials because of the perception that
they are less able to tolerate cytotoxic chemotherapy than younger
patients, and are more likely to suffer toxic effects that
adversely affect their quality of life (4). Physicians may be concerned that
age-related impairment in renal or hepatic function could
exacerbate the toxic effects of chemotherapy, and that the presence
of comorbidities could reduce the capacity of their elderly
patients to tolerate such effects. While it is true that the
incidence of age-related organ dysfunction and the development of
comorbid conditions increase abruptly between 70 and 75 years of
age (5), the clinical significance
of the relationship between age and comorbid conditions is complex
in patients with cancer (6) and it
has been suggested that chronological age is not a valid criterion
on which to base treatment decisions in NSCLC (7). Clinical trials that have investigated
the effects of cytotoxic chemotherapy in unselected elderly
patients have reported modest improvements in outcomes (8–11),
while an analysis of two large, randomised trials of
adjuvant/palliative chemotherapy for NSCLC found that the age of
the patient did not influence overall survival (OS), but that the
presence of comorbid conditions was linked with poorer survival
(7).
New targeted therapies for NSCLC, such as the human
epidermal growth factor receptor (EGFR) tyrosine-kinase inhibitor,
erlotinib (Tarceva®), combine therapeutic efficacy with
a relatively benign toxicity profile compared with cytotoxic
chemotherapy, and so represent attractive new therapeutic options
for the treatment of elderly patients with NSCLC (12). Erlotinib has been demonstrated to
significantly prolong OS vs. placebo in previously-treated patients
with NSCLC (n=731) (13), with the
improvement in survival benefit being apparent in a broad range of
patient subtypes. Erlotinib is now approved in more than 80
countries for the treatment of patients who have received at least
one line of chemotherapy.
The TaRceva LUng cancer Survival Treatment (TRUST)
study was a large, open-label, phase IV study of erlotinib,
designed to allow access to erlotinib monotherapy for patients with
advanced stage IIIB/IV NSCLC who had previously failed, or were
considered unsuitable to receive, standard chemotherapy or
radiotherapy, and were ineligible for other erlotinib trials
(14). A total of 6,665 patients
were enrolled in the study, from 513 centres across 51 countries,
and recruitment ceased on 31 May, 2007. The cut-off date for the
final analysis was 17 April, 2009. The findings of the study
confirmed the favourable efficacy and safety profile of erlotinib
in a large heterogeneous population of NSCLC patients; the 1-year
survival rate was 37.7%, and median OS and progression-free
survival (PFS) were 7.9 and 3.25 months, respectively (14). The large size of the study database
made it feasible to evaluate outcomes among the large number of
older patients (≥70 years) who participated; this report describes
outcomes among elderly patients who received erlotinib as their
first line therapy.
Patients and methods
Patients
Eligible patients had histologically- or
cytologically-confirmed, unresectable, stage IIIB/IV NSCLC. This
analysis was limited to patients who had received no previous
therapies for their NSCLC (systemic chemotherapy or radiotherapy)
because they were ineligible to receive such treatment. Patients of
both Asian and non-Asian ethnicity were included in the analysis.
Patients were unsuitable for other erlotinib trials. Other
eligibility criteria included: age ≥18 years, Eastern Cooperative
Oncology Group (ECOG) performance status (PS) 0–3; adequate
haematological, renal and hepatic function; estimated life
expectancy of ≥12 weeks [full details of eligibility criteria and
other methodological details were described by Reck et
al(14)]. Key exclusion
criteria included: evidence of unstable systemic disease; prior
treatment with anti-EGFR agents; any previous malignancies within
the last 5 years (other than cervical carcinoma in situ or
skin cancer that underwent successful treatment); untreated brain
metastases (newly diagnosed or pre-existing) or spinal cord
compression; and any significant ophthalmological
abnormalities.
The study complied with the Declaration of Helsinki
and Good Clinical Practice guidelines. Informed consent was
obtained from all patients, and the protocol was approved at all
centres by appropriate ethics committees.
Study treatment
Oral erlotinib was administered once daily at a dose
of 150 mg to all patients, until unacceptable toxicity, disease
progression or death. Dose interruption or reduction (in 50 mg
decrements) was permitted in the event of treatment-related adverse
events (AEs).
Clinical assessments
Outcomes included: best response (as assessed by the
investigators); PFS; OS; safety and tolerability [including
incidence and grade of erlotinib-related rash, serious AEs (SAEs),
treatment-related SAEs and AEs leading to treatment withdrawal].
Clinical and laboratory assessments were conducted at baseline,
then every 4 weeks throughout the study. Tumour response was
assessed using Response Evaluation Criteria in Solid Tumours
(RECIST) (15), at least every 2
months. Tumour responses were confirmed by a second assessment, 4
weeks after the initial determination of response. Safety and
tolerability evaluations were assessed and graded using National
Cancer Institute Common Terminology Criteria for Adverse Events
version 3.0. Treatment-related AEs were reported if they were not
included on a list of pre-specified AEs defined in the study
protocol (i.e., rash, pruritus, dry skin, diarrhoea, nausea,
vomiting, stomatitis, abdominal pain, fatigue, dyspnea, cough,
anorexia, infection, conjunctivitis and keratoconjunctivitis
sicca).
Statistical analysis
PFS was determined from the date of erlotinib
initiation until the date of first documented progression according
to RECIST objective tumour assessment, or until the date of death
for any reason in the absence of disease progression. OS was
determined from the date of initiation of erlotinib until the date
of death from any cause.
Results
Patients
The intent-to-treat population (n=485) included all
patients ≥70 years of age who had received at least one dose of
first-line erlotinib and for whom clinical data (from submitted
case report forms) had been entered in the study database by the
cut-off date of 17 April, 2009. Demographic and disease
characteristics at baseline for the ‘first-line erlotinib/elderly’
group and for the overall TRUST population are shown in Table I. Seventy-six of the 485 ‘first-line
erlotinib/elderly’ patients (16%) were of Asian ethnicity, just
over half (54%) were male, and two-thirds (67%) were current or
former smokers. Fifty percent had adenocarcinoma and 22% had
squamous-cell carcinoma. Seventy percent had stage IV disease (a
slightly smaller percentage than in the overall TRUST population
(79%)] and 38% were ECOG PS 2/3, compared with 24% of the total
population.
 | Table IBaseline demographic and clinical
characteristics for elderly patients (≥70 years) who received
first-line erlotinib (n=485), and for the overall TRUST population
(n=6,580). |
Table I
Baseline demographic and clinical
characteristics for elderly patients (≥70 years) who received
first-line erlotinib (n=485), and for the overall TRUST population
(n=6,580).
| Characteristics | TRUST first-line
elderly population | TRUST overall
population (14) |
|---|
| Median age, years
(range) | 77 (70–91) | 63 (19–91) |
| Gender, n (%) |
| Male | 260 (54) | 3,974 (60) |
| Female | 225 (46) | 2,606 (40) |
| Ethnic origin, n
(%) |
| Caucasian/white | 399 (82) | 5057 (77) |
| Black | 2 (<1) | 29 (<1) |
| Asian | 76 (16) | 1,345 (20) |
| Other | 8 (2) | 149 (2) |
| ECOG PS, n (%) |
| 0 | 72 (15) | 1,473 (22) |
| 1 | 231 (48) | 3,504 (53) |
| 2 | 139 (29) | 1,235 (19) |
| 3 | 43 (9) | 360 (5) |
| No data | 0 (0) | 8 (<1) |
| Stage, n (%) |
| Stage IIIB | 140 (29) | 1,376 (21) |
| Stage IV | 338 (70) | 5,185 (79) |
| Other | 6 (1) | 15 (<1) |
| No data | 1 (<1) | 4 (<1) |
| Histology, n (%) |
| Adenocarcinoma | 243 (50) | 3,590 (55) |
| Bronchoalveolar
carcinoma | 61 (13) | 372 (6) |
| Large-cell
carcinoma | 20 (4) | 382 (6) |
| Squamous-cell
carcinoma | 106 (22) | 1,552 (24) |
| Other | 55 (11) | 681 (10) |
| No data | 0 (0) | 3 (<1) |
| Smoking status, n
(%) |
| Non-smoker | 158 (33) | 2,004 (30) |
| Current or former
smoker | 327 (67) | 4,567 (69) |
| No data | 0 (0) | 9 (<1) |
Response and survival
Best response data for erlotinib (Table II) were available for 356 of the
‘first-line erlotinib/elderly’ group, among whom the overall
response rate was 14%, compared with 13% for the overall TRUST
population. The disease control rate for erlotinib was 79%
(compared with 69% for the overall TRUST population; P<0.0001).
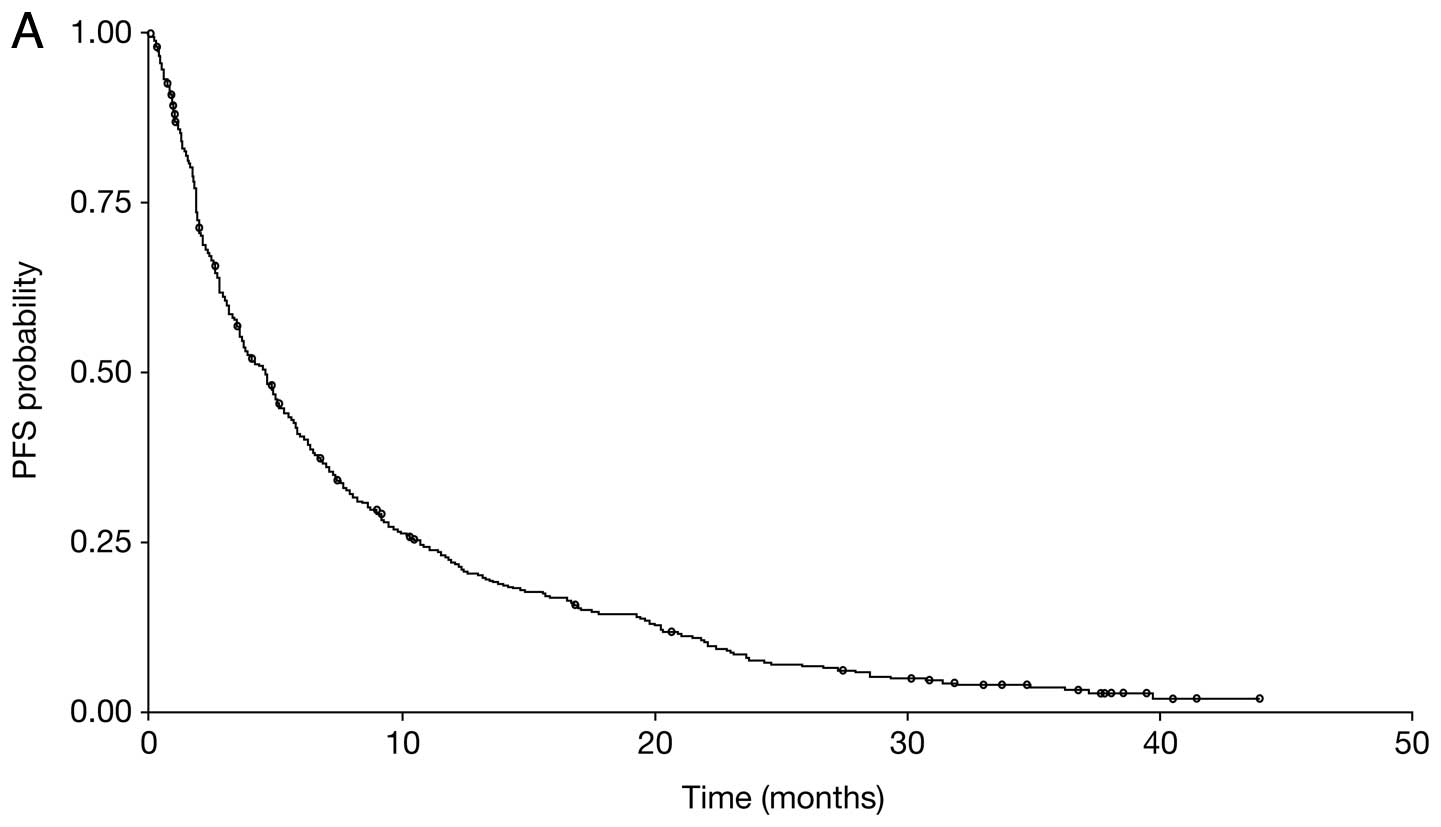
Median PFS for the ‘first-line erlotinib/elderly’ group was 4.57
months [95% confidence interval (CI), 3.68–5.22] (Fig. 1A), and median OS was 7.29 months
(95% CI, 6.27–8.67) (Fig. 1B),
while the one-year survival rate was 36.6%.
| Table IIBest response rates with erlotinib for
elderly patients (≥70 years) who received first-line erlotinib
(n=356), and for the overall TRUST population (n=5,394). |
Table II
Best response rates with erlotinib for
elderly patients (≥70 years) who received first-line erlotinib
(n=356), and for the overall TRUST population (n=5,394).
| Best response to
therapy in patients with data available, n (%) | TRUST first-line
elderly population | TRUST overall
population (14) |
|---|
| Complete
response | 3 (<1) | 45 (<1) |
| Partial response | 47 (13) | 668 (12) |
| Stable disease | 231 (65) | 2,992 (55) |
| Progressive
disease | 55 (15) | 1,483 (27) |
| Not evaluable | 20 (6) | 206 (4) |
| Overall response
ratea (%) | 14 | 13 |
| Disease control
rateb (%) | 79 | 69 |
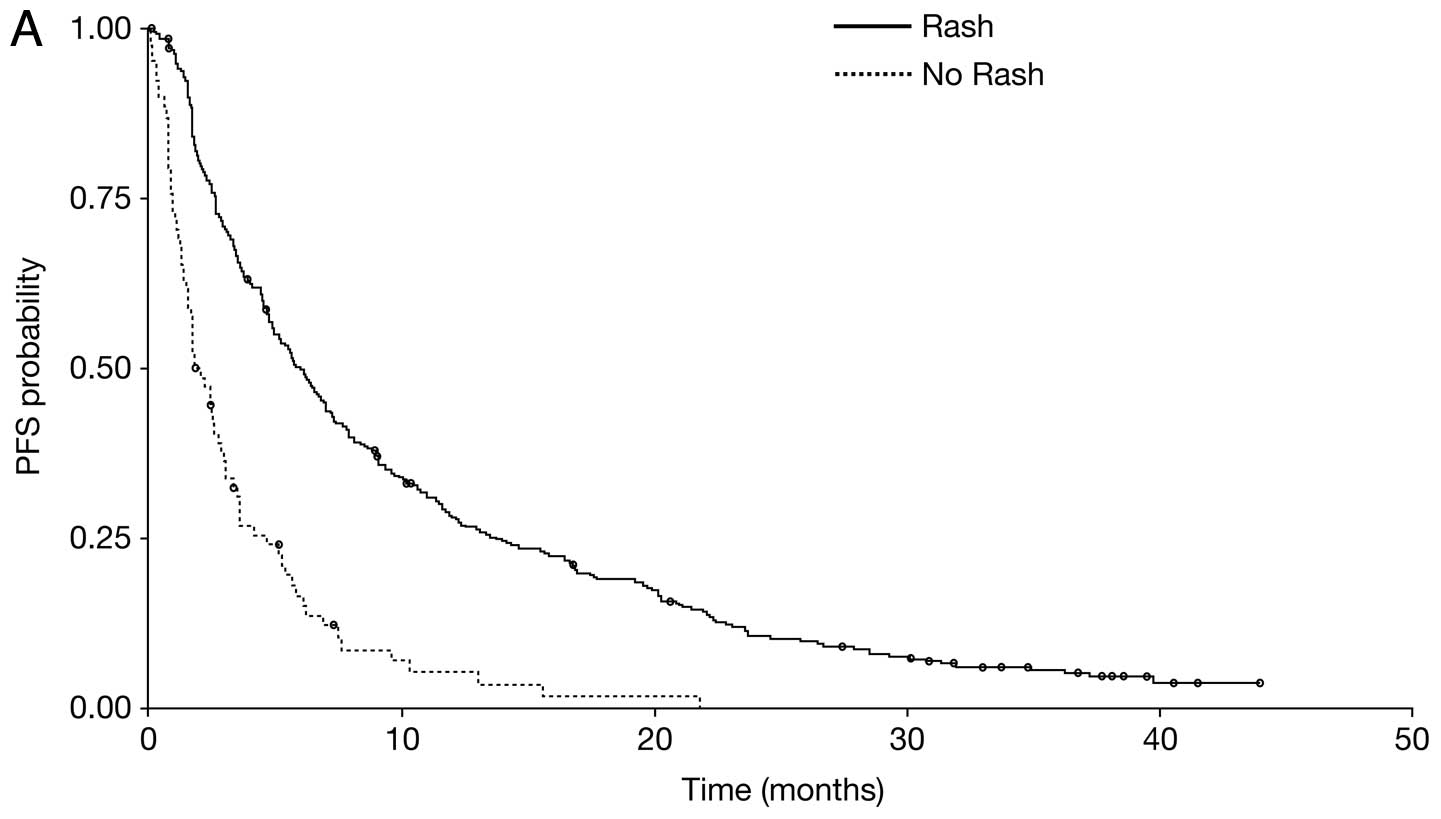
Median PFS and OS were both significantly longer for
patients who developed erlotinib-related rash (Fig. 2). For patients with rash, median PFS
was 6.08 months (95% CI, 5.03–7.10) vs. 2.04 months (95% CI,
1.64–2.92) for those without rash [hazard ratio [HR) 0.36;
P<0.001], and median OS was 10.91 months (95% CI, 9.10–13.21)
and 3.12 months (95% CI, 2.17–4.96), respectively (HR 0.30;
P<0.0001).
Survival parameters were also determined separately
for elderly patients of Asian ethnicity (n=76) and non-Asian
ethnicity (n=409) receiving first-line erlotinib. Median PFS was
4.86 months (95% CI, 3.25–9.13) for Asian patients and 4.24 months
(95% CI, 3.58–5.03) for non-Asian patients (HR 1.15; P=0.27), and
median OS was 9.69 months (95% CI, 6.44–11.89) and 7.19 months (95%
CI, 6.14–8.54), respectively (HR 1.15; P=0.31).
Elderly patients with poor PS (n=139 for PS 2 and
n=43 for PS 3) had worse survival outcomes than those with good PS
(n=303), median PFS was 5.58 months (95% CI, 4.73–6.70) for PS 0/1
vs. 3.15 months (95% CI, 2.56,4.14) for PS 2 and 1.81 months (95%
CI, 1.38–2.73) for PS 3. Similar results were seen with median OS,
those with PS 0/1 had median OS of 10.38 months (95% CI,
8.54–12.29) while those with a PS of 3 had median OS of just 2.07
months (95% CI, 1.45–3.68).
Toxicity
Safety data were available for all 485 ‘first-line
erlotinib/elderly’ patients, 325 of whom (67%) had at least one AE
(Table III). Eighty-seven
patients (18%) had an erlotinib-related AE (other than the
pre-specified AEs defined in the study protocol) and 20 patients
(4%) had a grade ≥3 erlotinib-related AE [compared with 173
patients (3%) in the overall TRUST population]. Seven percent of
patients had a treatment-related SAE, compared with 4% of the
overall TRUST population (Table
IV). Dose reductions with erlotinib occurred in 27% of the
‘first-line erlotinib/elderly’ group; most of these (97%) were
reductions to 100 mg/day. By comparison, in the overall TRUST
population, 17% of patients received a reduced dose of erlotinib,
and 96% of these were reductions to 100 mg/day. Erlotinib-related
AEs led to treatment discontinuation in 50 of the ‘first-line
erlotinib/elderly’ group (10%), while two deaths were associated
with treatment-related toxicity (<1%). In the overall TRUST
population, 337 patients (5%) discontinued treatment due to
erlotinib-related AEs and 24 deaths (<1%) were reported due to
treatment toxicity.
| Table IIITolerability of erlotinib therapy in
elderly patients (≥70 years) treated in the first-line setting
(n=485) and in the overall population in the TRUST study
(n=6,580). |
Table III
Tolerability of erlotinib therapy in
elderly patients (≥70 years) treated in the first-line setting
(n=485) and in the overall population in the TRUST study
(n=6,580).
| AEs, n (%) | TRUST first-line
elderly population | TRUST overall
population (14) |
|---|
| Patients with at
least one treatment-related AEa | 87 (18) | 799 (12) |
| Patients with at
least one treatment-related SAE | 35 (7) | 274 (4) |
| Patients who
discontinued study due to treatment-related AEs | 50 (10) | 337 (5) |
| Patients who died due
to a treatment-related AE | 2 (<1) | 24 (<1) |
| Table IVIncidence of specific SAEs in elderly
patients (≥70 years) receiving first-line erlotinib (n=485) vs. the
overall TRUST population (n=6,580). |
Table IV
Incidence of specific SAEs in elderly
patients (≥70 years) receiving first-line erlotinib (n=485) vs. the
overall TRUST population (n=6,580).
| TRUST first-line
elderly populationa | TRUST overall
population (14) |
|---|
|
|
|
|---|
| SAEs, n (%) | All | Grade ≥3 | All | Grade ≥3 |
|---|
| Patients with at
least one treatment-related SAE | 35 (7) | 29 (6) | 274 (4) | 209 (3) |
| Gastrointestinal
disorders | 15 (3) | 11 (2) | 121 (2) | 89 (1) |
| Diarrhoea | 9 (2) | 8 (2) | 67 (1) | 49 (<1) |
| Nausea | 3 (<1) | 2 (<1) | 24 (<1) | 11 (<1) |
| General disorders
and administrative site conditions | 2 (<1) | 2 (<1) | 26 (<1) | 18 (<1) |
| Hepatobiliary
disorders | 2 (<1) | 2 (<1) | 5 (<1) | 5 (<1) |
| Infections and
infestations | 2 (<1) | 2 (<1) | 22 (<1) | 16 (<1) |
| Metabolism and
nutrition disorders | 7 (1) | 4 (<1) | 27 (<1) | 18 (<1) |
| Dehydration | 4 (<1) | 2 (<1) | 15 (<1) | 10 (<1) |
| Respiratory,
thoracic and mediastinal disorders | 3 (<1) | 3 (<1) | 37 (<1) | 30 (<1) |
| Pneumonitis | 2 (<1) | 2 (<1) | 6 (<1) | 6 (<1) |
| Skin and
subcutaneous tissue disorders | 9 (2) | 7 (1) | 40 (<1) | 31 (<1) |
| Rash | 8 (2) | 7 (1) | 31 (<1) | 26 (<1) |
Biomarkers
Of the 485 patients included in this analysis,
EGFR mutation status was known for just 18 patients: 16 had
wild-type tumours and two had EGFR mutation-positive
tumours. Both patients with mutation-positive status were female
and Caucasian, with stage IV disease and an ECOG PS of 2. Patient 1
was 80 years old and was a never smoker with non-adenocarcinoma
histology; she had PFS and OS of 8.54 months. Patient 2 was a
78-year-old former/current smoker with adenocarcinoma; she had an
impressive PFS of 31.9 months and OS of 41.6 months.
Discussion
The goals of first-line chemotherapy for elderly
NSCLC patients (≥65 years old) are similar to those for younger
patients, i.e., to extend survival and relieve cancer-related
symptoms, but relatively few randomised controlled studies have
specifically investigated elderly patients with NSCLC. The first
such trial was the Elderly Lung Cancer Vinorelbine Italian Study,
in which single-agent vinorelbine was reported to improve quality
of life and survival vs. supportive care alone in patients older
than 70 years of age (median survival 27 vs. 21 weeks, P=0.04)
(16). Five of 71 patients
discontinued treatment due to severe toxic events (grade 3/4
constipation, grade 2 heart toxicity), and grade 4 leucopenia
occurred in 4 patients but did not lead to discontinuation.
In the first randomised phase III trial with taxane
monotherapy in elderly patients with advanced NSCLC, treatment with
docetaxel achieved a statistically significant improvement in PFS
(5.5 vs. 3.1 months) and response rate (22.7% vs. 9.9%) compared
with vinorelbine (17). OS favoured
docetaxel (10.3 vs. 6.4 months) but the difference was not
statistically significant (HR 0.78; P=0.65). Grade 3/4 neutropenia
occurred in more patients on docetaxel than vinorelbine (P=0.031),
but there was no difference in the incidence of grade 3/4 febrile
neutropenia and infection.
Combination chemotherapy has also been evaluated in
a small number of trials involving elderly populations. An interim
analysis of a trial comparing gemcitabine plus vinorelbine with
vinorelbine alone suggested a significant advantage for the
combination arm (median survival of 7 vs. 4.5 months, respectively)
(18). The combination regimen
resulted in grade 3/4 neutropenia and thrombocytopenia in 38 and
13% of patients, respectively, higher incidences than seen with
vinorelbine alone (28 and 8%, respectively). These findings were
challenged by the Multicenter Italian Lung Cancer in the Elderly
Study, a large, randomised phase III trial involving 698 NSCLC
patients with a median age of 74 years (8). In this trial the combination of
vinorelbine and gemcitabine was no more effective than single-agent
vinorelbine or gemcitabine (median survival was 36 weeks for
vinorelbine, 28 weeks for gemcitabine and 30 weeks for the
combination). Moreover, the combination was slightly more toxic,
although quality of life was similar across the three treatment
arms, and the authors concluded that until further studies showed a
clear benefit for combination therapy, the recommended treatment
for elderly patients with advanced NSCLC should be single-agent
chemotherapy. This was supported by another phase III study that
compared the efficacy of monotherapy vs. combination chemotherapy
in elderly patients (>65 years of age) and those with poor PS
(19). Eighty percent of patients
enrolled were >65 years of age, and the results showed that
combination chemotherapy led to a modest improvement in time to
progression (4.8 vs. 2.9 months; P=0.004) without an effect on OS
(5.5 vs. 5.1 months; P=0.65). Grade 3/4 myelosuppression was
significantly more common with combination therapy.
The results of a retrospective analysis of the ECOG
4599 trial [carboplatin, paclitaxel and bevacizumab (PCB) vs.
carboplatin and paclitaxel alone (PC)], on the basis of age have
also been reported (20).
Twenty-six percent of patients (n=224) enrolled in the trial were
>70 years of age; 113 were randomised to PC and 111 to PCB.
Compared with younger patients, the elderly group had more toxicity
with PCB (87% had grade 3 toxicity compared with 70% of the younger
group; P<0.001). Significant toxicities included grade 4
neutropenia, gastrointestinal bleed, proteinuria, muscle weakness,
neuropathy and dizziness. There was a superior response rate and a
non-significant trend towards improved PFS in the elderly group,
but no difference in OS (PCB=11.3 months; PC=12.1 months;
P=0.4).
Elderly patients are more likely than younger
patients to suffer from age-related impairments in organ function,
as well as other comorbidities and pre-existing medical conditions.
Consequently, it is essential that NSCLC treatments considered for
use in elderly patients should not induce unacceptable levels of
toxicity or impair patients' quality of life. In previously-treated
patients with NSCLC (13), it has
been reported that erlotinib monotherapy achieved improvements in
survival compared with placebo, among all patient subgroups
evaluated, including those aged ≥60 years.
The current findings demonstrate that erlotinib is
well tolerated as a first-line treatment for elderly patients with
advanced NSCLC. Efficacy outcomes for elderly patients in the
first-line setting were at least comparable to those for elderly
patients in previous erlotinib trials. The median PFS was somewhat
longer for the TRUST ‘first-line erlotinib/elderly’ group (4.57
months) than for the overall TRUST population (3.25 months). In a
phase II trial of first-line erlotinib in patients aged ≥70 years
(12), the median time to
progression was reported as 3.5 months. Although the data are not
directly comparable between the BR.21 trial and the current
analysis, because BR.21 examined the use of erlotinib in the
second-/third-line setting, PFS for elderly patients in the BR.21
study was 3 months (21). The
disease control rate for the TRUST ‘first-line erlotinib/elderly’
group (79%) was significantly higher than for the overall TRUST
population (69% P<0.0001) and the median OS for the ‘first-line
erlotinib/elderly’ patients (7.29 months) was similar to that for
the overall TRUST population (7.9 months).
Tolerability is a key consideration for medications
that are to be used for the treatment of elderly patients receiving
therapy for advanced NSCLC. It is therefore important to recognise
that in this analysis of elderly patients receiving erlotinib in
the first-line setting, no new safety signals were identified. The
most common AE seen with erlotinib is skin rash, but this is
usually mild and manageable and also has potential as a surrogate
marker of therapeutic efficacy. As reported in previous studies of
erlotinib (22), the current
analysis found that both PFS and OS were significantly longer in
patients who developed rash than in those who did not.
The incidence of erlotinib-related AEs and SAEs was
slightly higher in this subgroup population than in the overall
TRUST population, but the differences were not significant. Dose
reductions and discontinuations due to toxicity were slightly more
common in the ‘first-line erlotinib/elderly’ population than in the
overall TRUST population, but this may be because elderly patients
tend to have reduced organ function compared with younger patients,
and so may have higher exposure to erlotinib. The presence of
comorbidities may also have exacerbated any adverse reactions to
erlotinib.
Elderly patients are also more likely to have
reduced PS, which may affect response to treatment. Results
presented from the Tarceva Or Placebo In Clinically Advanced Lung
cancer (TOPICAL) study of erlotinib in NSCLC patients with poor PS
in the UK suggest that this factor may limit the benefit obtained
from erlotinib treatment in some subgroups, particularly in male
patients (23). The results of this
analysis demonstrate that PS is inversely related to survival, with
those patients who have poor PS having a significantly shorter
median PFS and OS than those with good PS. It is likely that this
difference would be observed regardless of treatment, however, as
these are the patients most likely to experience rapid progression
and deterioration before they have a chance to benefit from
treatment.
In conclusion, erlotinib was found to be effective
and well tolerated as a first-line treatment for elderly patients
involved in the TRUST study. Erlotinib should be considered for the
treatment of elderly patients with advanced NSCLC who are unable to
receive standard chemotherapy or radiotherapy.
Acknowledgements
The TRUST study was supported by funding from F.
Hoffmann-La Roche Ltd., which was involved in the study design,
collection, analysis and interpretation of the data. Support for
third party writing assistance for this manuscript was provided by
F. Hoffmann-La Roche Ltd. Ofer Merimsky has received payment for a
leadership position/advisory role from Medison and Pfizer. He has
also received honoraraia from Eli Lilly and research funding from
F. Hoffmann-La Roche. Martin Reck has received payment for
consultancy on advisory boards from F. Hoffmann-La Roche Ltd.,
Lilly, Pfizer, BMS and AstraZeneca, as well as honoraria for
lectures from F. Hoffmann-La Roche Ltd., Lilly, Merck and
AstraZeneca.
References
|
1
|
Weir HK, Thun MJ, Hankey BF, et al: Annual
report to the nation on the status of cancer, 1975–2000, featuring
the uses of surveillance data for cancer prevention and control. J
Natl Cancer Inst. 95:1276–1299. 2003.
|
|
2
|
Gridelli C, Perrone F and Monfardini S:
Lung cancer in the elderly. Eur J Cancer. 33:2313–2314. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bunn PA Jr and Lilenbaum R: Chemotherapy
for elderly patients with advanced non-small cell lung cancer. J
Natl Cancer Inst. 95:341–343. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Alam N, Shepherd FA, Winton T, et al:
Compliance with post-operative adjuvant chemotherapy in non-small
cell lung cancer: an analysis of National Cancer Institute of
Canada and intergroup trial JBR10 and a review of the literature.
Lung Cancer. 47:385–394. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Balducci L: Geriatric oncology: challenges
for the new century. Eur J Cancer. 36:1741–1754. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Balducci L: Geriatric oncology. Crit Rev
Oncol Hematol. 46:211–220. 2003. View Article : Google Scholar
|
|
7
|
Asmis TR, Ding K, Seymour L, et al;
National Cancer Institute of Canada Clinical Trials Group. Age and
comorbidity as independent prognostic factors in the treatment of
non-small cell lung cancer: a review of National Cancer Institute
of Canada Clinical Trials Group trials. J Clin Oncol. 26:54–59.
2008. View Article : Google Scholar
|
|
8
|
Gridelli C, Perrone F, Gallo C, et al:
Chemotherapy for elderly patients with advanced non-small cell lung
cancer: the Multicenter Italian Lung Cancer in the Elderly Study
(MILES) phase III randomized trial. J Natl Cancer Inst. 95:362–372.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Boukovinas I, Souglakos J, Hatzidaki D, et
al: Docetaxel plus gemcitabine as front-line chemotherapy in
elderly patients with lung adenocarcinomas: a multicenter phase II
study. Lung Cancer. 63:77–82. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gridelli C, De Maio E, Barbera S, et al:
The MILES-2G phase 2 study of single-agent gemcitabine with
prolonged constant infusion in advanced non-small cell lung cancer
elderly patients. Lung Cancer. 61:67–72. 2008. View Article : Google Scholar
|
|
11
|
Pallis AG, Polyzos A, Boukovinas I, et al:
Pooled analysis of elderly patients with non-small cell lung cancer
treated with front line docetaxel/gemcitabine regimen: the Hellenic
Oncology Research Group experience. J Thorac Oncol. 3:505–510.
2008. View Article : Google Scholar
|
|
12
|
Jackman DM, Yeap BY, Lindeman NI, et al:
Phase II clinical trial of chemotherapy-naive patients > or = 70
years of age treated with erlotinib for advanced non-small cell
lung cancer. J Clin Oncol. 25:760–766. 2007.
|
|
13
|
Shepherd FA, Rodrigues Pereira J, Ciuleanu
T, et al; National Cancer Institute of Canada Clinical Trials
Group. Erlotinib in previously treated non-small-cell lung cancer.
N Engl J Med. 353:123–132. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Reck M, van Zandwijk N, Gridelli C, et al:
Erlotinib in advanced non-small cell lung cancer: efficacy and
safety findings of the global phase IV Tarceva Lung Cancer Survival
Treatment study. J Thorac Oncol. 5:1616–1622. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Therasse P, Arbuck SG, Eisenhauer EA, et
al: New guidelines to evaluate the response to treatment in solid
tumors. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
The Elderly Lung Cancer Vinorelbine
Italian Study Group. Effects of vinorelbine on quality of life and
survival of elderly patients with advanced non-small-cell lung
cancer. J Natl Cancer Inst. 91:66–72. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kudoh S, Takeda K, Nakagawa K, et al:
Phase III study of docetaxel compared with vinorelbine in elderly
patients with advanced non-small-cell lung cancer: results of the
West Japan Thoracic Oncology Group Trial (WJTOG 9904). J Clin
Oncol. 24:3657–3663. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Frasci G, Lorusso V, Panza N, et al:
Gemcitabine plus vinorelbine yields better survival outcome than
vinorelbine alone in elderly patients with advanced non-small cell
lung cancer. A Southern Italy Cooperative Oncology Group (SICOG)
phase III trial. Lung Cancer. 34:S65–S69. 2001. View Article : Google Scholar
|
|
19
|
Hainsworth JD, Spigel DR, Farley C, et al:
Weekly docetaxel versus docetaxel/gemcitabine in the treatment of
elderly or poor performance status patients with advanced non small
cell lung cancer: a randomized phase 3 trial of the Minnie Pearl
Cancer Research Network. Cancer. 110:2027–2034. 2007. View Article : Google Scholar
|
|
20
|
Ramalingam SS, Dahlberg SE, Langer CJ, et
al: Outcomes for elderly, advanced-stage non small-cell lung cancer
patients treated with bevacizumab in combination with carboplatin
and paclitaxel: analysis of Eastern Cooperative Oncology Group
Trial 4599. J Clin Oncol. 26:60–65. 2008. View Article : Google Scholar
|
|
21
|
Wheatley-Price P, Ding K, Seymour L, et
al: Erlotinib for advanced non-small cell lung cancer in the
elderly: an analysis of the National Cancer Institute of Canada
Clinical Trials Group Study BR. 21. J Clin Oncol. 26:2350–2357.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wacker B, Nagrani T, Weinberg J, et al:
Correlation between development of rash and efficacy in patients
treated with the epidermal growth factor receptor tyrosine kinase
inhibitor erlotinib in two large phase III studies. Clin Cancer
Res. 13:3913–3921. 2007. View Article : Google Scholar
|
|
23
|
Lee S, Rudd R, Khan I, et al: TOPICAL:
randomized phase III trial of erlotinib compared with placebo in
chemotherapy-naïve patients with advanced non-small cell lung
cancer (NSCLC) and unsuitable for first-line chemotherapy. J Clin
Oncol. 28(Suppl 15): 75042010.
|