Introduction
The incidence of esophageal cancer ranks seventh in
malignant diseases worldwide; the mortality rate ranks sixth
(1). Esophageal squamous cell
carcinoma (ESCC) is the dominant pathological type. Early ESCC
clinical symptoms and signs are atypical and are frequently
overlooked, thus early diagnosis is difficult. Additionally, it is
easy for ESCC to progress to the late stage, owing to transfer to
or an invasion of the surrounding organs, namely the trachea and
aorta, which are adjacent to the esophagus; this process is
facilitated by the esophagus not having a serous layer. Clinically,
for more than half of patients with ESCC, the opportunity to have
the tumor removed at diagnosis is missed, which is a cause of
concern for the clinical doctors. The current treatment of ESCC is
the combined strategy of surgical excision, radiotherapy and
chemotherapy; however, it is largely ineffective, since the 5-year
survival rate subsequent to surgery is 20–40% (2,3).
Apoptosis is a highly regulated process, necessary
for homeostasis, as it removes excessively damaged and aging mutant
cells (4). Dysfunction in the
apoptotic process contributes to the pathogenesis of a variety of
malignant tumors, and it is considered to be the key reason for
their occurrence and development, being closely associated with
tumor drug resistance (5). In the
event that apoptosis is hindered, the mutant cells accumulate and
increase in an uncontrolled manner (6). The members of the inhibitors of
apoptosis protein (IAP) family are important negative regulators of
apoptosis (7,8). The IAP family comprises eight
members, which are the key regulators of cytokinesis, apoptosis and
signal transduction and have been demonstrated to be tightly
associated with oncogenesis. Apollon, also termed baculoviral IAP
repeat containing 6 (BIRC6), a membrane-associated protein that is
localized on the Golgi compartment and the vesicular system, is the
largest member of the IAP family (9), which was identified by Chen et
al (10) in 1999. Its gene is
located on chromosome 2p21–22, encoding a large protein (530 kDa)
that contains a single baculovirus inhibitor of apoptosis protein
repeat domain and a ubiquitin-conjugating enzyme domain. Apollon is
expressed in the brain, placenta, testes, lymphatic cells and
secretory organs (10). A previous
study indicated that Apollon was a dual regulator of cell
proliferation and cell death, with multiple functions, due to its
different functional domains and diverse binding patterns (9). It inhibits apoptosis by directly
binding to cysteine/aspartate-specific proteases (the caspase
family). Its antiapoptotic function is more marked compared with
the B-cell chronic lymphocytic leukemia/lymphoma 2 family,
primarily via a combination of diablo IAP-binding mitochondrial
protein (Smac), HtrA serine peptidase 2 (HtrA2) and the caspases
(11,12). Apollon has been identified to be
important for apoptosis resistance in various types of cancer
(10,11,13–16).
Previous studies have determined that the upregulation of Apollon
may be important for tumor generation (17–21).
However, the association between ESCC and Apollon requires further
elucidation.
The present study detected Apollon expression using
immunohistochemistry and reverse transcription-quantitative
polymerase chain reaction (RT-qPCR) in ESCC tissues, adjacent
non-cancerous tissues (ANCTs) and normal tissues. Apollon
expression and clinicopathological features of ESCC were analyzed
to highlight the association between Apollon and the occurrence,
development and prognosis of ESCC.
Materials and methods
Patients and specimens
Patients were enrolled in the present study from
Thoracic Surgery Xiangya Hospital, Central South University between
May 2010 and May 2012, who were diagnosed with ESCC by more than
two pathologists. Specimens were obtained, including 80 cases of
ESCC tissues, 80 cases of paired ANCTs (~3–7 cm from the tumor
margin) and 50 cases of normal tissues, from intraoperative radical
esophagectomy specimens (>7 cm from the tumor margin). All
specimens were immediately snap-frozen in liquid nitrogen and
stored at −80°C until RNA and total protein extraction was
performed. The patients were 69 males and 11 females, younger than
75 years of age and first-diagnosed cases, and they had not been
exposed to chemotherapy, radiotherapy or other treatments prior to
being sampled. The clinical and pathological data were complete and
reliable. Informed consent was acquired from all patients prior to
surgery. This study was approved by the Xiangya Hospital, Central
South University Ethics Committee, and the usage of the information
and specimens collected has been handled and anonymized according
to the ethical and legal standards.
Reagents and instruments
Rabbit polyclonal anti-Apollon antibodies were
purchased from Abcam (cat. nos. ab84429 and ab19609; Cambridge,
UK); the PV-6001 two-step immunohistochemistry kit (cat. no.
PV-6001) was from OriGene Technologies, Inc. (Beijing, China);
Invitrogen® TRIzol reagent (cat. no. 15596026) was from
Thermo Fisher Scientific, Inc. (Waltham, MA, USA); the GoScript
Reverse Transcription kit (cat. no. A5001) was from Promega
Corporation (Madison, WI, USA); the GoTaq RT-qPCR kit (cat. no.
A6001) was from Promega Corporation; paraffin-embedded machines,
the paraffin slicing machine and the automatic upright microscope
system (DM5000 B) were from Leica Microsystems (GmbH, Wetzlar,
Germany); the 400W UV imaging system was from Kodak (Kodak, Tokyo,
Japan); and the ABI PRISM 7500 PCR applications were purchased from
Thermo Fisher Scientific, Inc.
Immunohistochemistry
The rapid PV two-step staining method was performed
with the following specifications: The paraffin slice thickness was
5 µm, and slices were grilled at 65°C for 60 min, followed
by dewaxing, hydration and high-temperature antigen retrieval in a
microwave in 0.1 M citrate solution (pH 6.0) for 10 min.
Subsequently, the slices were incubated with 3%
H2O2 at room temperature for 20 min, followed
by an incubation with goat serum at room temperature for 20 min,
and a subsequent incubation with the Apollon antibody (1:400) at
4°C overnight. The samples were then re-warmed and incubated with
the anti-rabbit secondary antibodies in the PV-6001 two-step
immunohistochemistry kit (cat. no. PV-6001; ZSGB-Bio Co., Ltd.,
Beijing, China) at room temperature for 20 min. The slices were
stained with 3,3′-diaminobenzidine and hematoxylin and mounted,
prior to microscopic examination. Immunohistochemical staining was
scored independently by two pathologists without knowledge of the
patients' characteristics. Any discrepancy was resolved by taking
the consensus view. The score of immunoreactivity was performed by
calculating the extent and intensity of staining positivity of the
cells in a semi-quantitative manner. Interpretation of the scores
was performed as previously described (22). The standards for evaluation
included the following: Positive stain intensity (0, negative; 1,
weak positive; 2, moderate positive; 3, strong positive) and
proportion of positive areas (≤10%=1, 10–50%=2, ≥50%=3). The
staining score was the multiplication of the positive stain
intensity and the proportion of positive areas. Five high-power
fields in each specimen were selected at random, and the final
score was the average of the five scores.
RT-qPCR
Total RNA was extracted from 1 mg esophagus tissue
using TRIzol, according to the manufacturers' protocol.
Subsequently, samples were treated with a DNA-free kit (Ambion;
Thermo Fisher Scientific, Inc.) to remove the chromosomal DNA. The
complementary DNA (cDNA) was synthesized using the GoScript Reverse
Transcription kit and stored at −20°C prior to use. The mRNA
expression levels of Apollon and β-actin were determined by RT-qPCR
using the ABI PRISM 7500 sequence detector system. The primer
sequences were: Apollon, forward (F): 5′-TGACAGGGCATACATCACAG-3′,
reverse (R): 5′-GCAACAATCTCCCACTGAAG-3′; and β-actin, F:
5′-GCACCACACCTTCTACAATGAG-3′, R: 5′-GATAGCACAGCCTGGATAGCA-3′. The
mRNA expression levels of the target genes were normalized to the
β-actin signal as a housekeeping gene. All the reactions were
performed in triplicate using 20 µl samples containing 50 ng
cDNA. The reaction protocol involved heating for 10 min at 95°C,
followed by 40 cycles of amplification (15 sec at 95°C and 1 min at
60°C). The data were analyzed using the ABI PRISM 7500 Sequence
Detection software v2.0.1. The levels of Apollon expression in
unknown samples were calculated as a ratio of Apollon to β-actin.
Data were analyzed using the 2−ΔΔCq method (23) and expressed as the log2 fold-change
[−ΔΔCq (ESCC / ANCT)].
Statistical analysis
The patients were categorized into two groups
according to the level of Apollon expression (high and low). The
differences in Apollon expression with respect to the clinical
factors at diagnosis, including age, gender, drinking history
(>10 years), tumor size, differentiation grade, tumor
(T)-classification, node (N)-classification and tumor, nodes, and
metastases (TNM) stage, were analyzed. The expression levels are
presented as median values. Counted data were compared using a
one-way analysis of variance or an unpaired t-test. Qualitative
data were compared using Pearson's χ2 test or Fisher's
exact test. The variables were evaluated in a stepwise multivariate
Cox analysis. P<0.05 was considered to indicate a statistically
significant difference.
Results
Classification of the patients and their
characteristics
A total of 80 patients were enrolled in the study.
The mean age of the patients was 59.5 years (range 42–74 years).
According to the 7th edition of the International Union Against
Cancer's esophageal cancer staging (2009 edition) (24), the enrolled patients were
classified as follows: 20 cases of stage I, 25 cases of stage II
and 35 cases of stage III.
Apollon expression is upregulated in ESCC
tissues
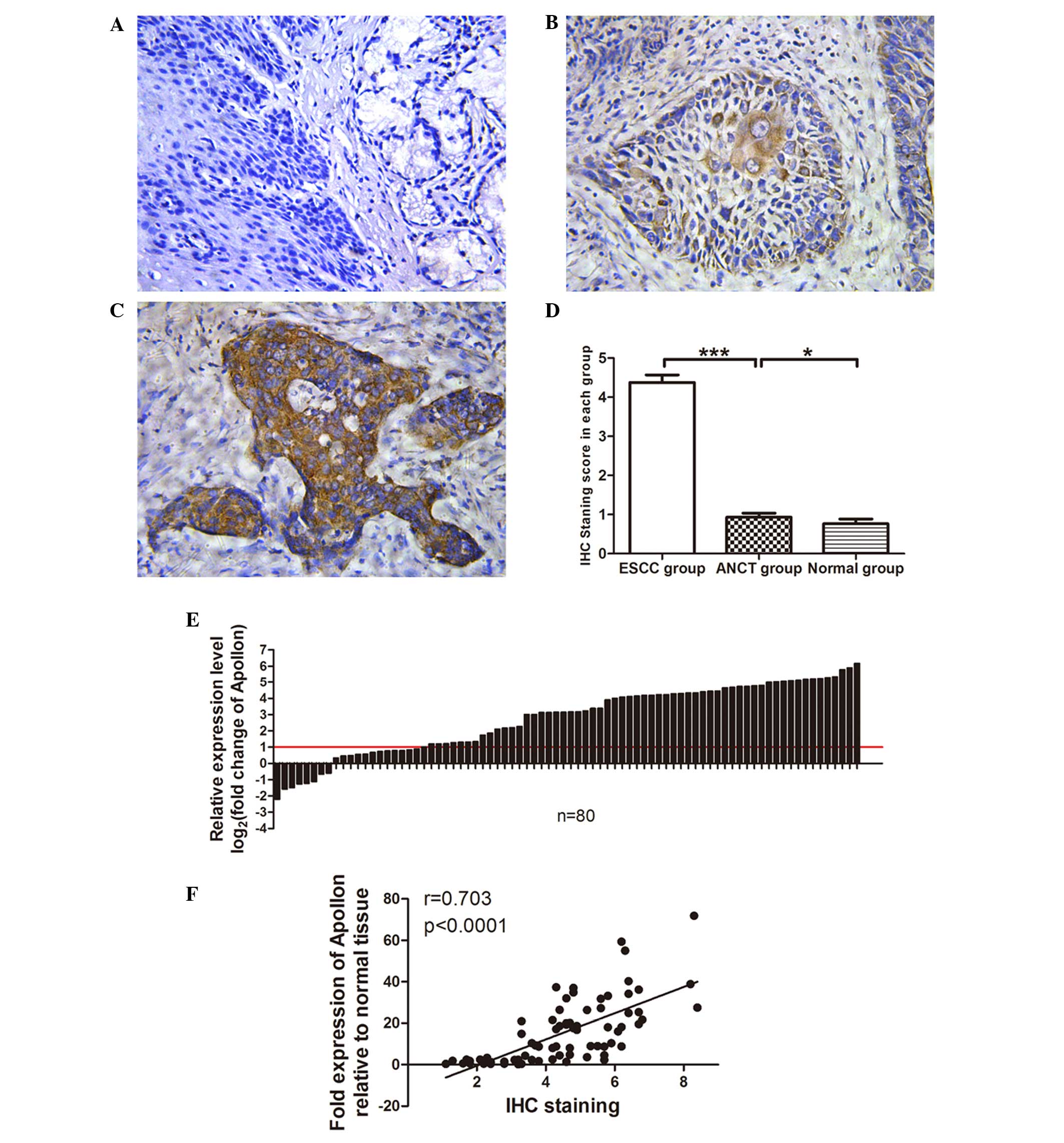
In the present study, Apollon protein was detected
by immunohistochemical staining. Apollon protein was expressed in
ESCC tissues, ANCTs and normal esophageal tissues, primarily in the
cytoplasm of carcinoma and squamous cells, or in the normal and
adjacent tissues in the underlying basal cells. In contrast with
the staining of Apollon in normal esophagus tissues, which was
mostly negative (Fig. 1A), the
positive reactants of Apollon were yellow or brown substances that
mainly existed in the cytoplasm (Fig.
1B and C). According to the standards used for evaluating the
samples (as detailed in the Materials and methods section), the
high expression level of Apollon protein was 60% (48/80) in the
tumor tissues, whereas it was 2.5% (2/80) in the ANCTs and 0%
(0/30) in the normal esophageal mucosa epithelial tissue. The
difference between the different tissue groups was statistically
significant (P<0.0001, Fig.
1D). No significant difference was identified in the Apollon
expression levels in the ANCT group compared with the normal tissue
group (P=0.132, Fig. 1D).
The mRNA expression levels of Apollon in the 80
cases of ESCCs and the paired ANCTs were subsequently analyzed by
RT-qPCR. A similar pattern of Apollon expression in terms of the
mRNA levels was identified: Compared with the paired ANCTs, a
3-fold increase in Apollon expression was noted in the ESCC tissues
(Fig. 1E). Comparative analysis of
paired ESCCs with ANCTs revealed that increased Apollon expression
(>2-fold [namely log2 (fold change)>1]) was observed in 75%
of the cases (60/80). The immunohistochemical staining score was
positively associated with the fold expression of Apollon mRNA
(Fig. 1F); therefore, the
overexpression of Apollon may be a frequent event in human
ESCC.
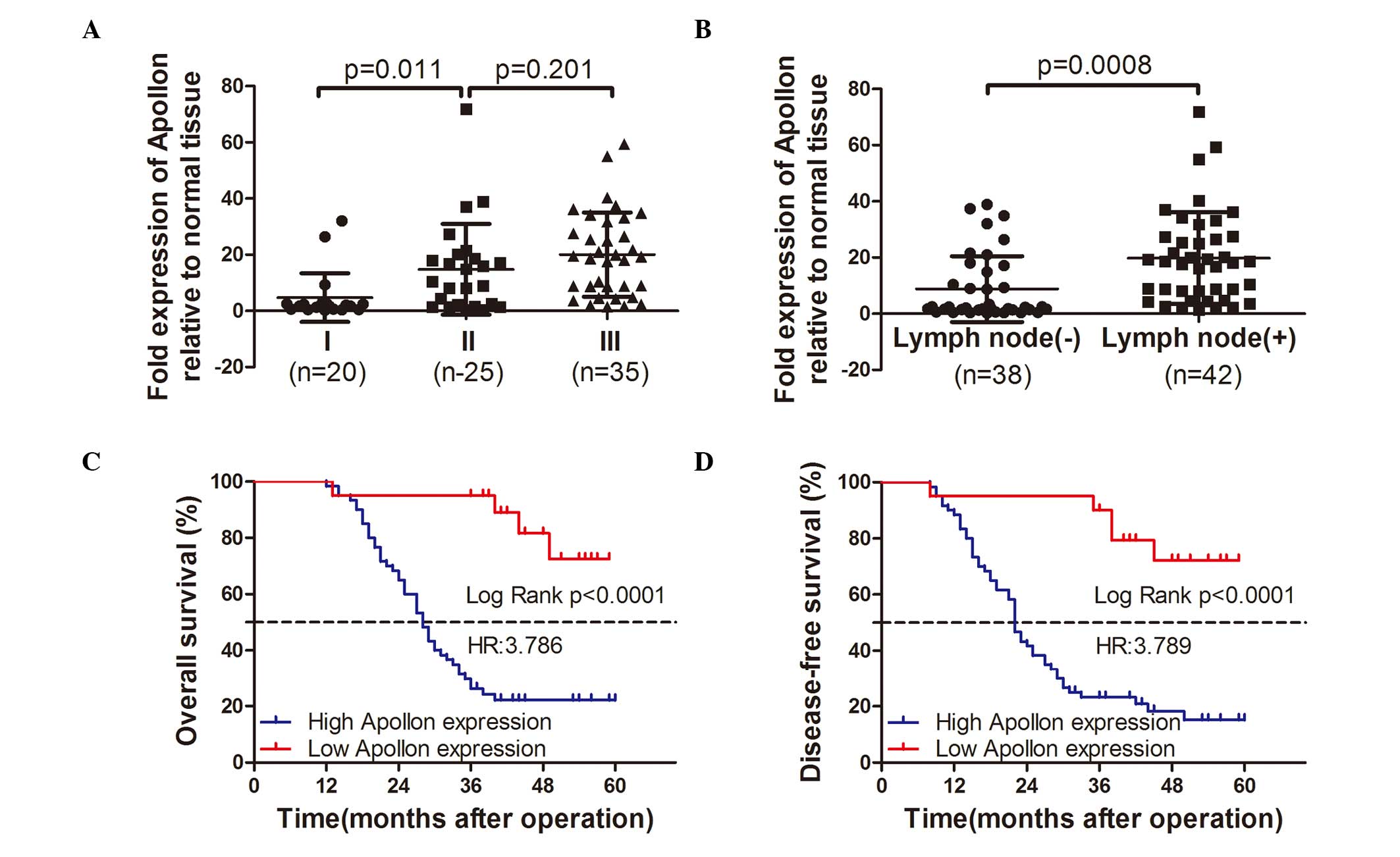
Expression levels of Apollon are
associated with the ESCC clinicopathological characteristics
The association between Apollon expression and the
clinicopathological characteristics of ESCC was determined by the
χ2 test. As summarized in Table I, the high expression of Apollon
was significantly associated with the TNM stage (P<0.001) and
lymph node (N classification) metastasis (P<0.001). However, no
significant difference was identified between Apollon expression
and age (P=1.000), gender (P=1.000), drinking history (P=0.587),
tumor differentiation (P=0.119) or tumor size (P=0.301).
 | Table ICorrelations between the Apollon
expression level and clinicopathological characteristics of 80
cases of ESCC. |
Table I
Correlations between the Apollon
expression level and clinicopathological characteristics of 80
cases of ESCC.
| Clinicopathological
variable | n | Apollon expression
| P-value |
|---|
| Low | High |
|---|
| Age (years) | | | | 1.000 |
| ≤60 | 39 | 10 | 29 | |
| >60 | 41 | 10 | 31 | |
| Gender | | | | 1.000 |
| Female | 11 | 3 | 8 | |
| Male | 69 | 17 | 52 | |
| Drinking history
(years) | | | | 0.587 |
| ≤10 | 26 | 8 | 19 | |
| >10 | 54 | 12 | 41 | |
|
Differentiation | | | | 0.123 |
| Well | 21 | 6 | 15 | |
| Moderate | 42 | 13 | 29 | |
| Poor | 17 | 1 | 16 | |
| Tumor size
(cm) | | | | 0.301 |
| ≤4 | 45 | 9 | 36 | |
| >4 | 35 | 11 | 24 | |
| T
classification | | | | 0.464 |
| T1 | 28 | 10 | 18 | |
| T2 | 12 | 2 | 10 | |
| T3 | 30 | 6 | 24 | |
| T4 | 10 | 2 | 8 | |
| N
classification | | | |
<0.001 |
| N0 | 40 | 18 | 22 | |
| N1 | 22 | 2 | 20 | |
| N2 | 18 | 0 | 18 | |
| TNM stage | | | |
<0.001 |
| I | 20 | 11 | 9 | |
| II | 25 | 6 | 19 | |
| III | 35 | 3 | 32 | |
Upregulation of Apollon expression is
associated with the prognosis of ESCC
To assess the feasibility of using Apollon
expression as an ESCC prognostic factor, the Cox proportional
hazards regression model was introduced. Multivariate survival
analysis on all parameters was performed. It was determined that
overall survival time was significantly dependent on lymph node (N
classification) metastasis (P=0.009), TNM stage (P=0.036) and
Apollon expression levels (P=0.047; Table II), which indicated that patients
with ESCC who had high levels of Apollon expression also had
shorter overall survival times (median survival time: 28 vs. >60
months, P<0.001; Fig. 2)
compared with the low Apollon expression group. Additionally, it
was determined that lymph node metastasis (P= 0.044), TNM stage (P=
0.013) and Apollon expression levels (P=0.019; Table II) indicated significant
differences for disease-free survival rates in the multivariate
survival analysis. Patients with ESCC who had high Apollon
expression also had shorter disease-free survival rates (median
survival time: 22 vs. >60 months, P<0.001; Fig. 2) compared with the low Apollon
expression group.
| Table IICox regression multivariate analysis
of overall and disease-free survival in 80 patients with ESCC. |
Table II
Cox regression multivariate analysis
of overall and disease-free survival in 80 patients with ESCC.
| Variables | n | Overall survival
| Disease-free
survival
|
|---|
| HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (years) |
| <60 | 39 | 1 | | 1 | |
| ≥60 | 41 | 0.76
(0.39–1.48) | 0.415 | 0.64
(0.34–1.23) | 0.183 |
| Gender |
| Female | 11 | 1 | | 1 | |
| Male | 69 | 1.00
(0.366–2.78) | 0.986 | 0.92
(0.32–2.61) | 0.874 |
| Drinking history
(years) |
| ≤10 | 26 | 1 | | 1 | |
| >10 | 54 | 0.91
(0.41–2.04) | 0.817 | 1.07
(0.49–2.35) | 0.86 |
|
Differentiation | | | 0.864 | | 0.59 |
| Well | 21 | 1 | | 1 | |
| Moderate | 42 | 0.99
(0.43–2.31) | 0.997 | 1.19
(0.54–2.68) | 0.659 |
| Poor | 17 | 1.23
(0.48–3.16) | 0.667 | 1.58
(0.64–3.89) | 0.318 |
| Tumor size
(cm) |
| ≤4 | 42 | 1 | | 1 | |
| >4 | 38 | 1.00
(0.49–2.03) | 0.987 | 1.29
(0.67–2.50) | 0.446 |
| T
classification | | | 0.580 | | 0.533 |
| T1 | 28 | 1 | | 1 | |
| T2 | 13 | 1.54
(0.54–4.44) | 0.419 | 1.39
(0.49–3.91) | 0.525 |
| T3 | 29 | 0.66
(0.23–1.93) | 0.451 | 0.55
(0.19–1.54) | 0.255 |
| T4 | 10 | 0.84
(0.13–5.55) | 0.856 | 0.49
(0.72–3.35) | 0.469 |
| N
classification | | | 0.009 | | 0.044 |
| N0 | 39 | 1 | | 1 | |
| N1 | 23 | 2.79
(0.80–9.69) | 0.107 | 1.98
(0.61–6.45) | 0.259 |
| N2 | 18 | 14.90
(2.3–96.39) | 0.005 | 7.70
(1.29–46.02) | 0.025 |
| TNM stage | | | 0.036 | | 0.013 |
| I | 20 | 1 | | 1 | |
| II | 25 | 18.53
(1.82–188.6) | 0.014 | 12.25
(2.29–65.71) | 0.003 |
| III | 35 | 41.72
(2.37–733.9) | 0.011 | 27.66
(2.55–300.41) | 0.006 |
| Apollon
expression | | | | | 0.019 |
| Low | 20 | 1 | | 1 | |
| High | 60 | 3.63
(1.02–12.95) | 0.047 | 4.03
(1.25–12.98) | |
Discussion
Apollon is the largest member of the IAP family
(10), and it has been associated
with various types of cancer (10,11,13–16),
including breast, colon, lung, cervical and prostate cancer,
gliomas, fibrosarcomas and osteosarcomas. However, the importance
of Apollon in ESCC has not been fully elucidated. The current study
investigated the protein and mRNA expression levels of Apollon in a
series of 80 paired ESCC specimens with intact follow-up data.
Immunohistochemical staining results revealed that
Apollon protein expression was higher in ESCC tissues compared with
ANCTs and normal esophageal tissues, as demonstrated by western
blot analysis. RT-qPCR analysis revealed high Apollon mRNA
expression in the majority of cases of ESCC (Fig. 1), which is in line with a previous
study on ESCC (25) and various
other cancer studies (13–16), indicating that Apollon may be
important for ESCC progression. Apollon contributes to oncogenesis
through its interference in the apoptotic balance. Apollon has a
prosurvival role due to its antiapoptotic function, which is
completed by its binding to the activated caspases (caspase-3,
caspase-8, caspase-9) to block the apoptotic pathway directly.
Additionally, it can ubiquitinate the IAPs antagonists, Smac and
HtrA2, and induce their proteolytic and degradative functions,
which indirectly enhances the antiapoptotic activity of IAPs
(11,12). Apollon may be able to switch on
ESCC via a different molecular mechanism; however, further studies
are required to clarify this.
From the clinical data, the expression level of
Apollon in the high and low groups was compared in terms of the
various clinicopathological factors of 80 patients with ESCC. It
was determined that the expression of Apollon was not associated
with the age, gender, drinking history, tumor size or tumor
differentiation of the patients; however, it was significantly
associated with the lymph node metastasis and TNM stage. Therefore,
it is possible that the higher expression of Apollon leads to
malignant biological characteristics, despite the tumor
differentiation, which is inconsistent with previous studies
(26–30): More Apollon expression indicated
poorer differentiation. Similar results have been published by Low
et al (16) in terms of
prostate cancer and Apollon, which indicate that increased
expression of Apollon was a late event in prostate cancer and did
not correlate with differentiation.
Previous research has revealed that a high
expression of Apollon was well correlated with lymph node
metastasis (21) and poor survival
(26,27). Lymph node metastasis may be used as
a prognostic factor for ESCC; therefore, a multivariate survival
analysis was performed on Apollon expression and the lymph node
metastasis status. The results revealed that patients with high
Apollon expression/more lymph node metastasis (N2) had shorter
overall and disease-free survival times compared with patients with
neither. Higher lymph node metastasis or Apollon overexpression
worsens the prognosis. Therefore, the evaluation of Apollon
expression in conjunction with the lymph node status may provide
novel information for the prognosis of patients, and provide an
opportunity for improved planning of appropriate treatment
strategies and management subsequent to surgery. Apollon is an
indicator for metastasis and prognosis for ESCC, which is
consistent with previous studies regarding Apollon (26–30).
Previous studies have also determined that Apollon was an
independent, unfavorable prognostic factor for overall survival and
disease-free survival rates in human epithelial ovarian cancer
(26). Notably, abundant previous
research has demonstrated that a high level of Apollon expression
is associated with poor chemotherapeutic outcomes in various
carcinomas, including colon cancer, acute leukemia, prostate cancer
and melanoma, whereas silencing Apollon may improve patient
sensitivity to chemotherapy (19,28,31,32).
Therefore, Apollon may be a novel tumor therapeutic target;
however, further investigation is required in order to elucidate
the association between ESCC and Apollon.
Previous studies revealed that a significant
overexpression of IAPs in cancer tissue, including cIAP-1, cIAP-2,
X-linked inhibitor of apoptosis and Survivin, was regarded as an
early event in esophageal cancer and did not correlate with
histological type or the stage of tumors (33–35).
However, according to the data from the current study, Apollon is
an antitype: High expression of Apollon is a late cancer event,
indicative of a poor prognosis, and, as it is distributed in the
cytoplasm and is not secreted into the extracellular space, its
value in terms of early diagnosis is limited.
In conclusion, the present study indicates, to the
best of our knowledge for the first time, that Apollon expression
is associated with the prognosis of ESCC and may be a potentially
valuable prognostic factor and novel chemotherapeutic target for
ESCC. The mechanisms of Apollon in tumorigenesis and metastasis
remain unclear, although the present study provides the first step
for future researchers to perform further investigations in
vitro and in vivo in order to clarify the regulatory
mechanisms of Apollon expression in ESCC in association with the
apoptotic signaling pathways.
Acknowledgments
This study was supported by grants from the Hunan
Provincial Natural Science Foundation of China (grant no. 14JJ7091)
and Hunan Provincial Tumor Hospital Fund (grant no. A2013-02).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mariette C, Piessen G and Triboulet JP:
Therapeutic strategies in oesophageal carcinoma: Role of surgery
and other modalities. Lancet Oncol. 8:545–553. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lerut T, Coosemans W, Decker G, De Leyn P,
Nafteux P and Van Raemdonck D: Cancer of the esophagus and
gastroesophageal junction: Potentially curative therapies. Surg
Oncol. 10:113–122. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Giancotti FG and Tarone G: Positional
control of cell fate through joint integrin/receptor protein kinase
signaling. Annu Rev Cell Dev Biol. 19:173–206. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Naito M: Molecular mechanism of apoptosis
inhibition by IAPs and its implication to cancer therapy.
Seikagaku. 78:525–528. 2006.In Japanese. PubMed/NCBI
|
|
6
|
Evan G: Cancer - a matter of life and cell
death. Int J Cancer. 71:709–711. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Srinivasula SM and Ashwell JD: IAPs:
what's in a name? Mol Cell. 30:123–135. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wong RS: Apoptosis in cancer: From
pathogenesis to treatment. J Exp Clin Cancer Res. 30:872011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hauser HP, Bardroff M, Pyrowolakis G and
Jentsch S: A giant ubiquitin-conjugating enzyme related to IAP
apoptosis inhibitors. J Cell Biol. 141:1415–1422. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chen Z, Naito M, Hori S, Mashima T, Yamori
T and Tsuruo T: A human IAP-family gene, apollon, expressed in
human brain cancer cells. Biochem Biophys Res Commun. 264:847–854.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Qiu XB and Goldberg AL: The
membrane-associated inhibitor of apoptosis protein, BRUCE/Apollon,
antagonizes both the precursor and mature forms of Smac and
caspase-9. J Biol Chem. 280:174–182. 2005. View Article : Google Scholar
|
|
12
|
Qiu XB, Markant SL, Yuan J and Goldberg
AL: Nrdp1-mediated degradation of the gigantic IAP, BRUCE, is a
novel pathway for triggering apoptosis. EMBO J. 23:800–810. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hao Y, Sekine K, Kawabata A, Nakamura H,
Ishioka T, Ohata H, Katayama R, Hashimoto C, Zhang X, Noda T, et
al: Apollon ubiquitinates SMAC and caspase-9, and has an essential
cytoprotection function. Nat Cell Biol. 6:849–860. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lamers F, Schild L, Koster J, Speleman F,
Øra I, Westerhout EM, van Sluis P, Versteeg R, Caron HN and
Molenaar JJ: Identification of BIRC6 as a novel intervention target
for neuroblastoma therapy. BMC Cancer. 12:2852012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bianchini M, Levy E, Zucchini C, Pinski V,
Macagno C, De Sanctis P, Valvassori L, Carinci P and Mordoh J:
Comparative study of gene expression by cDNA microarray in human
colorectal cancer tissues and normal mucosa. Int J Oncol. 29:83–94.
2006.PubMed/NCBI
|
|
16
|
Low CG, Luk IS, Lin D, Fazli L, Yang K, Xu
Y, Gleave M, Gout PW and Wang Y: BIRC6 protein, an inhibitor of
apoptosis: Role in survival of human prostate cancer cells. PloS
One. 8:e558372013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pohl C and Jentsch S: Final stages of
cytokinesis and midbody ring formation are controlled by BRUCE.
Cell. 132:832–845. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ren J, Shi M, Liu R, Yang QH, Johnson T,
Skarnes WC and Du C: The Birc6 (Bruce) gene regulates p53 and the
mitochondrial pathway of apoptosis and is essential for mouse
embryonic development. Proc Natl Acad Sci USA. 102:565–570. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chu L, Gu J, Sun L, Qian Q, Qian C and Liu
X: Oncolytic adenovirus-mediated shRNA against Apollon inhibits
tumor cell growth and enhances antitumor effect of 5-fluorouracil.
Gene Ther. 15:484–494. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lopergolo A, Pennati M, Gandellini P,
Orlotti NI, Poma P, Daidone MG, Folini M and Zaffaroni N: Apollon
gene silencing induces apoptosis in breast cancer cells through p53
stabilisation and caspase-3 activation. Br J Cancer. 100:739–746.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Van Houdt WJ, Emmink BL, Pham TV, Piersma
SR, Verheem A, Vries RG, Fratantoni SA, Pronk A, Clevers H, Borel
Rinkes IH, et al: Comparative proteomics of colon cancer stem cells
and differentiated tumor cells identifies BIRC6 as a potential
therapeutic target. Mol Cell Proteomics. 10:M111.0113532011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chen Y, Fu D, Xi J, Ji Z, Liu T, Ma Y,
Zhao Y, Dong L, Wang Q and Shen X: Expression and clinical
significance of UCH37 in human esophageal squamous cell carcinoma.
Dig Dis Sci. 57:2310–2317. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar
|
|
24
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM Classification of Malignant Tumors. 7th ed. Oxford:
Wiley-Blackwell; 2010
|
|
25
|
Zhang S, Tang W, Weng S, Liu X, Rao B, Gu
J, Chen S, Wang Q, Shen X, Xue R and Dong L: Apollon modulates
chemosensitivity in human esophageal squamous cell carcinoma.
Oncotarget. 5:7183–7197. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wang L, Chen YJ, Hou J, Wang YY, Tang WQ,
Shen XZ and Tu RQ: Expression and clinical significance of BIRC6 in
human epithelial ovarian cancer. Tumour Biol. 35:4891–4896. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sung KW, Choi J, Hwang YK, Lee SJ, Kim HJ,
Lee SH, Yoo KH, Jung HL and Koo HH: Overexpression of Apollon, an
anti-apoptotic protein, is associated with poor prognosis in
childhood de novo acute myeloid leukemia. Clin Cancer Res.
13:5109–5114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ismail EA, Mahmoud HM, Tawfik LM, Habashy
DM, Adly AA, El-Sherif NH and Abdelwahab MA: BIRC6/Apollon gene
expression in childhood acute leukemia: Impact on therapeutic
response and prognosis. Eur J Haematol. 88:118–127. 2012.
View Article : Google Scholar
|
|
29
|
Tang W, Xue R, Weng S, Wu J, Fang Y, Wang
Y, Ji L, Hu T, Liu T, Huang X, et al: BIRC6 promotes hepatocellular
carcinogenesis: Interaction of BIRC6 with p53 facilitating p53
degradation. Int J Cancer. 136:E475–E487. 2015. View Article : Google Scholar
|
|
30
|
Dong X, Lin D, Low C, Vucic EA, English
JC, Yee J, Murray N, Lam WL, Ling V, Lam S, et al: Elevated
expression of BIRC6 protein in non-small-cell lung cancers is
associated with cancer recurrence and chemoresistance. J Thorac
Oncol. 8:161–170. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Abe S, Yamamoto K, Hasegawa M, Inoue M,
Kurata M, Hirokawa K, Kitagawa M, Nakagawa Y and Suzuki K: Bone
marrow cells of myelodysplastic syndromes exhibit significant
expression of apollon, livin and ILP-2 with reduction after
transformation to overt leukemia. Leuk Res. 29:1095–1096. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tassi E, Zanon M, Vegetti C, Molla A,
Bersani I, Perotti V, Pennati M, Zaffaroni N, Milella M, Ferrone S,
et al: Role of Apollon in human melanoma resistance to antitumor
agents that activate the intrinsic or the extrinsic apoptosis
pathways. Clin Cancer Res. 18:3316–3327. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nemoto T, Kitagawa M, Hasegawa M, Ikeda S,
Akashi T, Takizawa T, Hirokawa K and Koike M: Expression of IAP
family proteins in esophageal cancer. Exp Mol Pathol. 76:253–259.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhou S, Ye W, Shao Q, Qi Y, Zhang M and
Liang J: Prognostic significance of XIAP and NF-κB expression in
esophageal carcinoma with postoperative radiotherapy. World J Surg
Oncol. 11:2882013. View Article : Google Scholar
|
|
35
|
Vaĭshlia NA, Zinov'eva MV, Sass AV,
Kopantsev EP, Vinogradova TV and Sverdlov ED: Increase of BIRC5
gene expression in non-small cell lung cancer and esophageal
squamous cell carcinoma does not correlate with expression of genes
SMAC/DIABLO and PML encoding its inhibitors. Mol Biol (Mosk).
42:652–661. 2008.
|