Introduction
Non-alcoholic fatty liver disease (NAFLD) is a
pandemic disease, and one-third of the population worldwide is
affected (1,2). Since the liver is one of the target
organs of insulin, a high prevalence of insulin resistance is seen
in patients with NAFLD (3,4). An increase in insulin resistance is
associated with the development of not only type 2 diabetes
mellitus but also life-threatening diseases such as liver
cirrhosis, hepatocellular carcinoma, and cardiovascular diseases in
patients with NAFLD (5). Thus,
improved insulin resistance is an important therapeutic target in
patients with NAFLD. Anti-diabetic agents including pioglitazone
(6), glucagon-like peptide-1
(GLP-1) analogue (7), and
sodium-glucose cotransporter 2 inhibitor (8) lead to metabolic and histologic
improvement in patients with NAFLD complicated by diabetes
mellitus. However, no effective medication has been approved yet
for patients with NAFLD.
Isomaltulose (6-0-α-D-glucopyranosyl-D-fructose) is
a naturally-occurring disaccharide found in honey (9) and is composed of glucose and
fructose, similar to sucrose (10). Both isomaltulose and sucrose are
digested into glucose and fructose by α-glucosidase in the small
intestine and contribute the same caloric value of 4 kcal/g
(11,12). However, the digestive rate of
isomaltulose is significantly slower than that of sucrose because
the structural feature of isomaltulose is that glucose and fructose
are linked by an alpha-1,6-glycosidic bond (12,13).
In addition, isomaltulose affects the secretion of gut hormones
such as glucose-dependent insulinotropic polypeptide (GIP) and
GLP-1 (14,15), leading to an improvement of insulin
resistance. Thus, isomaltulose is a low glycemic index sweetener as
well as a functional disaccharide and is currently used in various
medical food and drink applications instead of sucrose (16).
In a rat model of metabolic syndrome, isomaltulose
is reported to reduce visceral fat mass and improves glucose
intolerance, resulting in inhibition of increase in blood pressure
and progression of diabetic nephropathy (17). Furthermore, in healthy subjects,
isomaltulose ingestion inhibits an increase in insulin resistance
and blood pressure (11,18). The beneficial effects of
isomaltulose on visceral fat, insulin resistance, and blood
pressure in patients who were obese have been reported in
double-blind, placebo-controlled interventional studies (19,20).
However, the effect of isomaltulose on insulin resistance has never
been investigated in patients with NAFLD.
An increase in insulin resistance can be caused by
various factors including amino acid, fatty acid, and bile acid
metabolism (3,21,22).
Metabolomic analysis is a systematic examination of metabolites in
a given biological sample and can reveal novel pathways (23). Metabolomic analysis has recently
been applied to the identification of the pharmacological
mechanisms of berberine, an isoquinoline alkaloid, for nonalcoholic
steatohepatitis (NASH) treatment and revealed metabolic disruption
involving phospholipids and unsaturated fatty acids in a rat model
of NASH (24). However,
metabolomic analysis has not been used to identify the
pharmacological mechanisms of isomaltulose in patients with
NAFLD.
The aim of this study was to investigate effects of
isomaltulose on insulin resistance in patients with NAFLD. In
addition, using metabolomic analysis, we investigated the effect of
isomaltulose on various metabolisms in patients with NAFLD.
Subjects and methods
Study design and ethics
This was a randomized, single-blinded controlled
interventional study, and our study protocol conformed to the
ethical guidelines of the 1975 Declaration of Helsinki, as
reflected by the prior approval of the institutional review board
of The Ethic Committee of Kurume University. All experiments were
performed in accordance with relevant guidelines and regulations.
All subjects provided written informed consent to participate in
this study.
Subjects
A total of 5 male patients diagnosed with NAFLD were
enrolled in this study. The following patient inclusion criteria
were used: Patients with i) NAFLD, ii) age >20 years, and iii)
written informed consent. The exclusion criteria were as follows:
Patients with i) hemoglobin A1c >8.0%, ii) insulin or
α-glucosidase inhibitor treatment, iii) liver cirrhosis, iv) renal
failure, v) a history of cardiovascular disease, or vi)
participation in any other clinical trial.
The subjects were randomly assigned into the sucrose
(Control) or isomaltulose group. After a 14-day wash-out term, each
subject was assigned to the other group.
Diagnosis of NAFLD
NAFLD was diagnosed according to the Clinical
Practice Guidelines for NAFLD/NASH as follows (25): i) hepatic steatosis evaluated by
liver biopsy, ultrasonography, computed tomography, or magnetic
resonance imaging; ii) ethanol intake <30 g/day; and iii)
exclusion of other liver diseases, including chronic hepatitis B,
chronic hepatitis C, autoimmune hepatitis, drug-induced liver
disease, primary biliary cholangitis, primary sclerosing
cholangitis, biliary obstruction, Wilson's disease, and
hemochromatosis.
Isomaltulose or sucrose administration
and blood collection
After a 12-hour overnight fast, the subjects
consumed 20 g isomaltulose in 200 ml of water or 20 g sucrose
(Control) in 200 ml of water in 1 min at 8:30 a.m. During the
procedure, the subjects were instructed to rest on a bed and fast.
Venous blood samples were collected before and 15 min after
administration. For plasma GIP and GLP-1 measurements, blood
samples were collected into a BD™ P100 Blood Collection System
containing protein stabilizers (BD Biosciences, Franklin Lakes, NJ,
USA). Blood samples were centrifuged at 3,000 × g for 15 min at 4°C
and stored at −20°C until analysis.
Laboratory determinations
Serum levels of aspartate aminotransferase (AST),
alanine aminotransferase (ALT), lactate dehydrogenase (LDH),
γ-glutamyl transpeptidase (GGT), total bilirubin, total
cholesterol, low-density lipoprotein (LDL)-cholesterol, blood urea
nitrogen (BUN), creatinine, nonesterified fatty acid, C-peptide
immunoreactivity (CPR), and blood glucose level were measured using
standard clinical methods (SRL Inc., Tokyo, Japan) as previously
described (4,26,27).
Measurement of serum GIP and GLP-1
levels
As previously described (28), plasma GIP and GLP-1 levels were
measured by an enzyme-linked immunosorbent assay using a Human GIP
ELISA kit (YK253; Yanaihara Institute Inc., Fujimiya, Japan) and a
Human GLP1 (7–36) ELISA kit (ab184857; Abcam,
Cambridge, UK), respectively, according to each manufacturer's
instructions.
Metabolomic analysis
Metabolomic analysis was performed twice using serum
samples taken before (0 min) and 15 min after isomaltulose or
sucrose treatment.
Preparation
Serum samples taken before and 15 min after
isomaltulose or sucrose treatment from a representative subject
were applied to a metabolomic analysis. Metabolome measurements
were performed at a service facility of LSI Medience Corporation
(Tokyo, Japan). Briefly, serum (200 µl) was added to methanol (800
µl) and then mixed for 15 min with a shaker at room temperature.
After it was centrifuged by 10,000 × g for 10 min, the supernatant
was dried up with nitrogen gas, and the residue was dissolved with
10% acetonitrile aqueous solution (200 µl). After adding internal
standards, they were analyzed with both liquid chromatography mass
spectrometry (LC-MS) and capillary electrophoresis coupled to mass
spectrometry (CE-MS). Tuning and calibration were performed with a
standard solution provided by Agilent Technology, and the
resolution errors were controlled within 3 ppm. The order of
measurement was randomized to minimize the specific error in each
group. Quality control samples were prepared by pooling samples and
were analyzed every 5 samples to verify the measurement
accuracy.
LC-time-of-flight mass spectrometry
(TOFMS) analysis
LC-MS datasets were acquired on a liquid
chromatography system (Agilent HP1200; Agilent Technologies, Inc.,
Santa Clara, CA, USA) equipped with a C18 column (2 µm, 50×2.0 mm
ID, CAPCELL PAK C18 IF; Shiseido, Tokyo, Japan) and coupled with an
electrospray ionization quadrupole TOFMS (Agilent 6520; Agilent
Technologies, Inc.). Solvent A was composed of a 5 mM ammonium
acetate aqueous solution, while solvent B was acetonitrile.
Metabolites were eluted at a flow rate of 0.2 ml/min at 40°C with a
linear gradient of 10–90% solvent B over 10 min, followed by a
further 5 min hold at 100% solvent B. The mass spectrometer was
operated in positive and negative scan mode (m/z 60 to 1,200) with
a capillary voltage of 3,500 V. The nebulizing gas pressure was 40
psi, and the dry gas flow was 8 l/min at 350°C.
CE-TOFMS analysis
Ionic metabolites were measured in the positive mode
of CE-TOFMS (Agilent CE-TOFMS 6520; Agilent Technologies, Inc.,).
Metabolites were separated in a fused-silica capillary (50 µm
i.d.x100 cm total length; GL Science, Tokyo, Japan) filled with 1
mol/l formic acid aqueous solution (cation mode), or 20 mM ammonium
formate and 20 mM ammonium acetate aqueous solution (pH 10, anion
mode) as an electrolyte. The sample solution was injected at 5 kPa
for 15 sec (approximately 15 nl), and a voltage of 30 kV was
applied. The temperatures of capillary and sample trays were
maintained at room temperature and 5°C, respectively. The sheath
liquid was methanol/water (50%v/v) containing 5 mM ammonium
acetate. CE-TOFMS was operated in both positive and negative scan
mode (m/z 60 to 1,200). The capillary voltage was set at 3,500 V,
and the nitrogen gas (heater temperature 250°C) flow rate was set
at 10 l/min.
Data analysis
A data file of mass spectrometry was converted to
csv format with an Agilent csv converter. All peak positions
(retention time and m/z) and areas were calculated by
Markeranalysis (LSI Medience, Tokyo, Japan) (29). All peak areas were aligned into one
data sheet, and the errors of peak intensities were corrected by
internal standards. Noise peaks were deleted compared with the
peaks detected in blank samples. Metabolites were identified by
comparing the retention time and m/z with standard data set
established by LSI Medience Corporation.
Effects of isomaltulose on insulin
resistance, GIP, GLP-1 secretion, and metabolites
Insulin resistance was evaluated by an increment of
serum CPR as previously described (30). ΔCPR was the change of serum CPR
level from baseline to 15 min after sucrose or isomaltulose
administration. Similarly, changes in GIP and GLP-1 secretions were
evaluated by ΔGIP and ΔGLP-1, which were changes of plasma GIP and
GLP-1 levels from baseline to 15 min after sucrose or isomaltulose
administration, respectively. The effects of isomaltulose on
metabolites were also evaluated by change of each metabolite level
from baseline (0 min) to 15 min after sucrose or isomaltulose
administration (Δ each metabolite). Variable that increased or
decreased after the administration was shown as positive or
negative expression level (∆ variable or -∆ variable) (Fig. 1).
Statistical analysis
Data are expressed as numbers or means ± standard
deviations. Differences between the two groups were analyzed using
the Wilcoxon signed-rank test. In metabolome analysis, mea n
fold-change and t-test for all detected peaks were performed
between the two groups. P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline patient characteristics
The baseline patient characteristics are summarized
in Table I. No significant
difference was seen in the serum levels of AST, ALT, GGT, or total
bilirubin between the sucrose (Control) and Isomaltulose groups.
There was no significant difference in fasting blood glucose or
serum CPR levels between the 2 groups (Table I).
 | Table I.Patients' characteristics at
baseline. |
Table I.
Patients' characteristics at
baseline.
| Characteristic | Control | Isomaltulose | P-value |
|---|
| Age (yeare) |
48.6±11.8 |
48.6±11.8 | 1.0000 |
| Body mass
index |
35.1±7.0 |
35.1±7.0 | 1.0000 |
| Red blood cells
(×104/µl) |
509.6±70.6 |
514.4±59.7 | 0.9105 |
| Hemoglobin
(g/dl) |
15.5±1.8 |
15.6±1.3 | 0.9540 |
| White blood cells
(/µl) |
8,500±2,515 |
7,600±2,531 | 0.5882 |
| Platelet count
(×104/µl) |
29.5±4.1 |
28.7±4.2 | 0.7634 |
| Aspartate
aminotransferase (IU/l) |
31.2±13.2 |
30.0±14.7 | 0.8953 |
| Alanine
aminotransferase (IU/l) |
45.6±36.9 |
40.2±28.5 | 0.8024 |
| Lactate
dehydrogenase (IU/l) |
227.2±109.8 |
237.2±108.4 | 0.8884 |
| γ-glutamyl
transpeptidase (IU/l) |
55.6±39.9 |
54.4±36.0 | 0.9614 |
| Total bilirubin
(mg/dl) |
0.52±0.18 |
0.46±0.18 | 0.6130 |
| Total cholesterol
(mg/dl) |
207.0±26.4 |
197.2±21.1 | 0.5350 |
| Low-density
lipoprotein cholesterol (mg/dl) |
138.6±17.6 |
125.0±23.8 | 0.3362 |
| Triglycerides
(mg/dl) |
144.2±51.4 |
154.2±56.5 | 0.7772 |
| Blood urea nitrogen
(mg/dl) |
14.7±2.9 |
14.7±4.2 | 0.9864 |
| Creatinine
(mg/dl) |
0.85±0.16 |
0.80±0.20 | 0.6998 |
| Fasting blood
glucose (mg/dl) |
132.0±38.7 |
145.0±50.0 | 0.6586 |
| C-peptide
immunoreactivity (ng/dl) |
2.38±0.99 |
2.61±1.71 | 0.8025 |
| Nonesterified fatty
acid (µEq/l) |
675.0±316.8 |
574.4±221.0 | 0.5782 |
Effect of isomaltulose on changes in
blood glucose and serum CPR levels
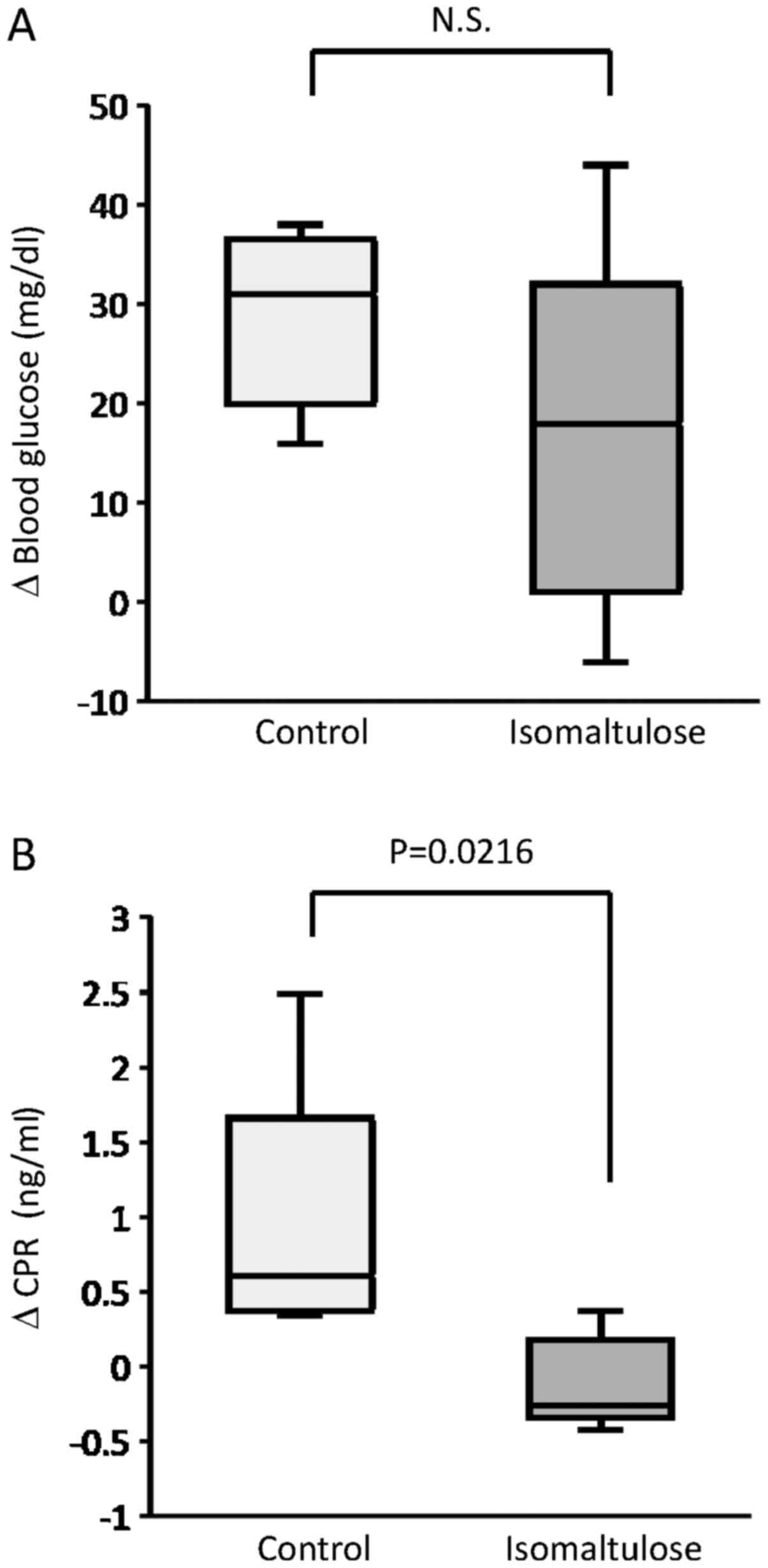
The effect of isomaltulose on blood glucose and
serum CPR levels was evaluated by changes in these variables from
baseline to 15 min after sucrose or isomaltulose administration.
Although there was no significant difference in changes of blood
glucose levels, the serum CPR level was significantly decreased in
the Isomaltulose group compared to that in the Control group
(Fig. 2).
Effect of isomaltulose on changes in
plasma GIP and GLP-1 levels
The effect of isomaltulose on plasma GIP and GLP-1
levels was evaluated by changes in these variables from baseline to
15 min after sucrose or isomaltulose administration. There was no
significant difference in changes of plasma GIP and GLP-1 levels
between the Control and Isomaltulose groups (Table II).
| Table II.Effects of isomaltulose on changes in
plasma GIP and GLP-1 levels. |
Table II.
Effects of isomaltulose on changes in
plasma GIP and GLP-1 levels.
| Level | Control | Isomaltulose | P-value |
|---|
| ∆GIP |
23.1±25.6 |
14.0±9.5 | 0.8345 |
| ∆GLP-1 |
−51.5±98.0 |
166.7±66.6 | 0.1437 |
Effect of isomaltulose on serum
metabolite levels
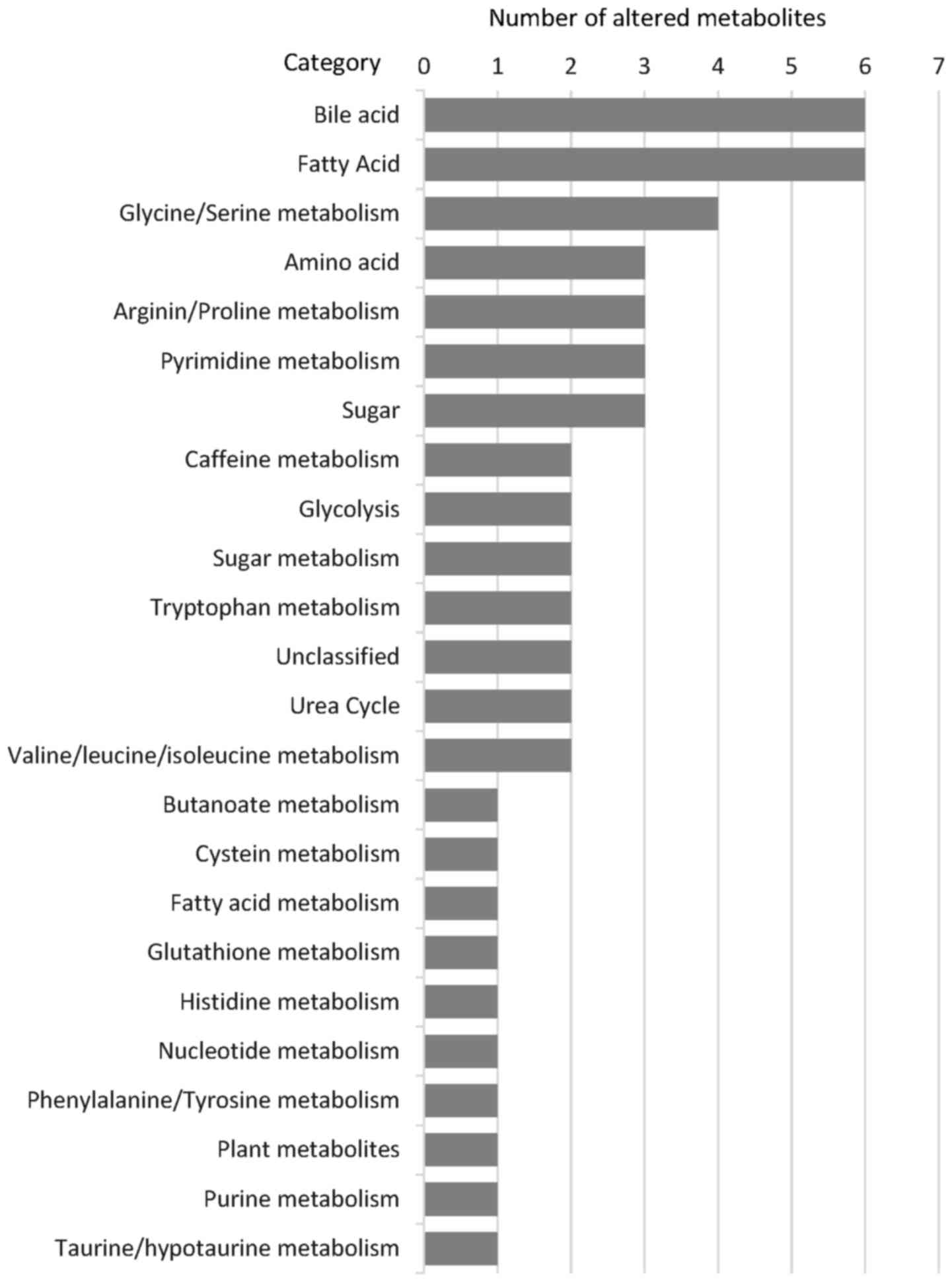
With metabolomic analysis, the effects of
isomaltulose on 201 metabolite levels were evaluated by changes in
these variables from baseline to 15 min after sucrose or
isomaltulose administration. A significant alteration was seen in
52 metabolites between the Control and Isomaltulose groups
(Table III). Many of these 52
altered metabolites were categorized as bile acid (6 metabolites),
fatty acid (6 metabolites), or glycine/serine metabolism (4
metabolites) (Fig. 3).
| Table III.Metabolites significantly altered by
isomaltulose in patients with NAFLD. |
Table III.
Metabolites significantly altered by
isomaltulose in patients with NAFLD.
|
|
|
| Control | Isomaltulose |
|
|
|---|
|
|
|
|
|
|
|
|
|---|
|
| Metabolite | Category | Mean | SD | Mean | SD | Ratio | P-value |
|---|
| 1 | L-Arginine | Amino acid | −507 | 80 | −2,570 | 180 | 5.00 | 0.0001 |
| 2 | L-Ornithine | Urea cycle | −62 | 64 | 1,390 | 137 | −25.00 | 0.0001 |
| 3 |
N-Acetylornithine | Arginin, proline
metabolism | −60 | 157 | −1,832 | 111 | 33.33 | 0.0001 |
| 4 |
Glycodeoxycholate | Bile acid | 29 | 3 | 134 | 12 | 4.55 | 0.0001 |
| 5 | Urea | Urea cycle | −79 | 12 | 115 | 23 | −1.45 | 0.0002 |
| 6 | Betaine | Glycine, serin
metabolism | −446 | 398 | 2,613 | 307 | −5.88 | 0.0005 |
| 7 | D-Xylulose | Sugar | 51 | 6 | 88 | 2 | 1.72 | 0.0006 |
| 8 | Glycocholate | Bile acid | 1,423 | 93 | 25,816 | 1,114 | 16.67 | 0.0006 |
| 9 |
6-Aminohexanoate | Fatty acid
metabolism | 14 | 3 | 42 | 5 | 2.94 | 0.0008 |
| 10 | Indole acetate | Tryptophan
metabolism | −170 | 25 | 41 | 32 | −0.24 | 0.0008 |
| 11 | Theobromine | Caffeine
metabolism | −440 | 139 | 350 | 80 | −0.79 | 0.0010 |
| 12 | Taurodeoxycholic
acid | Bile acid | 2,848 | 49 | 36,895 | 1,997 | 12.50 | 0.0011 |
| 13 | Uridine | Pyrimidine
metabolism | 416 | 135 | 1,917 | 323 | 4.55 | 0.0017 |
| 14 | L-Lactic acid | Glycolysis | 5,159 | 744 | 2,058 | 178 | 0.40 | 0.0022 |
| 15 | Eicosadienoic acid
(20:2) | Fatty acid | −18,121 | 2,263 | 2,174 | 4,642 | −0.12 | 0.0024 |
| 16 | D-Glycerate | Glycine, serin
metabolism | 3 | 11 | 239 | 60 | 100.00 | 0.0026 |
| 17 |
1-6-Anhydro-beta-d-Glucose | Sugar
metabolism | 642 | 39 | 1,409 | 202 | 2.17 | 0.0030 |
| 18 |
N-N-dimethylarginine | Arginin, proline
metabolism | −19 | 20 | 102 | 26 | −5.26 | 0.0032 |
| 19 | Tridecanoic
acid | Fatty acid | 51 | 76 | 719 | 181 | 14.29 | 0.0041 |
| 20 | Taurocholate | Bile acid | 16 | 23 | 210 | 54 | 12.50 | 0.0046 |
| 21 | Creatinine | Arginin, proline
metabolism | −994 | 580 | 1,401 | 494 | −1.41 | 0.0055 |
| 22 | Choline | Glycine, serin
metabolism | −2,423 | 443 | 1,316 | 1,183 | −0.54 | 0.0069 |
| 23 | Gramine | Tryptophan
metabolism | 15 | 20 | −136 | 47 | −9.09 | 0.0070 |
| 24 | 5-Oxoproline | Glutathione
metabolism | −77 | 41 | 523 | 213 | −6.67 | 0.0087 |
| 25 | Pseudouridine | Pyrimidine
metabolism | 51 | 37 | −59 | 20 | −1.15 | 0.0103 |
| 26 | Eicosenoic acid
(20:1) | Fatty acid | 18,075 | 4,264 | −2,476 | 6,533 | −0.14 | 0.0103 |
| 27 |
(R)-3-Hydroxybutanoate | Butanoate
metabolism | 13 | 62 | 190 | 30 | 14.29 | 0.0113 |
| 28 | Taurocyamine | Taurine and
hypotaurine metabolism | −233 | 112 | 153 | 103 | −0.66 | 0.0118 |
| 29 | Hydroxypropionic
acid | Pyrimidine
metabolism | −59 | 23 | −137 | 22 | 2.33 | 0.0131 |
| 30 |
D-Glyceraldehyde | Sugar
metabolism | 14,027 | 292 | 4,661 | 2,058 | 0.33 | 0.0143 |
| 31 | Docosapentaenoate
(n3 DPA; 22:5n3) | Fatty acid | −14,387 | 2,318 | 10,570 | 10,482 | −0.74 | 0.0158 |
| 32 |
4-Methyl-2-oxopentanoate | Valine, leucine and
isoleucine metabolism | 72 | 70 | 252 | 39 | 3.45 | 0.0178 |
| 33 |
Hyodeoxycholate | Bile acid | 332 | 83 | 128 | 37 | 0.38 | 0.0179 |
| 34 | L-Histidine | Amino acid | −41 | 49 | 215 | 104 | −5.26 | 0.0183 |
| 35 | L-Methionine
S-oxide | Cystein
metabolism | 19 | 12 | −19 | 12 | −1.02 | 0.0190 |
| 36 | Undecanoate
(11:0) | Fatty acid | −22 | 62 | 343 | 155 | −16.67 | 0.0191 |
| 37 | beta-D-Glucose | Sugar | 2,496 | 550 | 3,920 | 372 | 1.56 | 0.0206 |
| 38 | Abscisate | Plant
metabolites | −4 | 17 | 36 | 9 | −10.00 | 0.0216 |
| 39 |
N2,N2-Dimethylguanosine | Nucleotide
metabolism | −75 | 33 | 13 | 25 | −0.18 | 0.0218 |
| 40 |
1-5-anhydro-D-glucitol | Sugar | −2 | 8 | 15 | 2 | −7.69 | 0.0223 |
| 41 |
1-Methylhistidine | Histidine
metabolism | −132 | 123 | 255 | 148 | −1.92 | 0.0250 |
| 42 |
beta-hydroxyisovaleric acid | Valine, leucine and
isoleucine metabolism | −254 | 130 | 508 | 355 | −2.00 | 0.0251 |
| 43 | Arachidonate | Fatty acid | 48,499 | 15,330 | −473 | 20,184 | −0.01 | 0.0287 |
| 44 |
N,N-Dimethylglycine | Glycine, serin
metabolism | −23 | 21 | 127 | 75 | −5.56 | 0.0290 |
| 45 |
(±)-1,2-Diphenylethylenediamine | Unclassified | 26 | 18 | −53 | 37 | −2.04 | 0.0301 |
| 46 | Caffeine | Caffeine
metabolism | −1,724 | 485 | 110 | 895 | −0.06 | 0.0355 |
| 47 | α-D-Glucose
6-phosphate | Glycolysis | 2 | 43 | 122 | 52 | 50.00 | 0.0364 |
| 48 |
(S)(+)-Allantoin | Purine
metabolism | 955 | 82 | 718 | 109 | 0.75 | 0.0398 |
| 49 |
Chenodeoxycholate | Bile acid | 3,201 | 854 | 1,629 | 332 | 0.51 | 0.0411 |
| 50 | Homogentisate | Phenylalanine
tyrosine metabolism | −54 | 39 | 33 | 34 | −0.62 | 0.0424 |
| 51 | Ranitidine | Unclassified | 6 | 10 | −14 | 6 | −2.17 | 0.0432 |
| 52 | L-Tryptophan | Amino acid | −144 | 45 | 282 | 255 | −1.96 | 0.0463 |
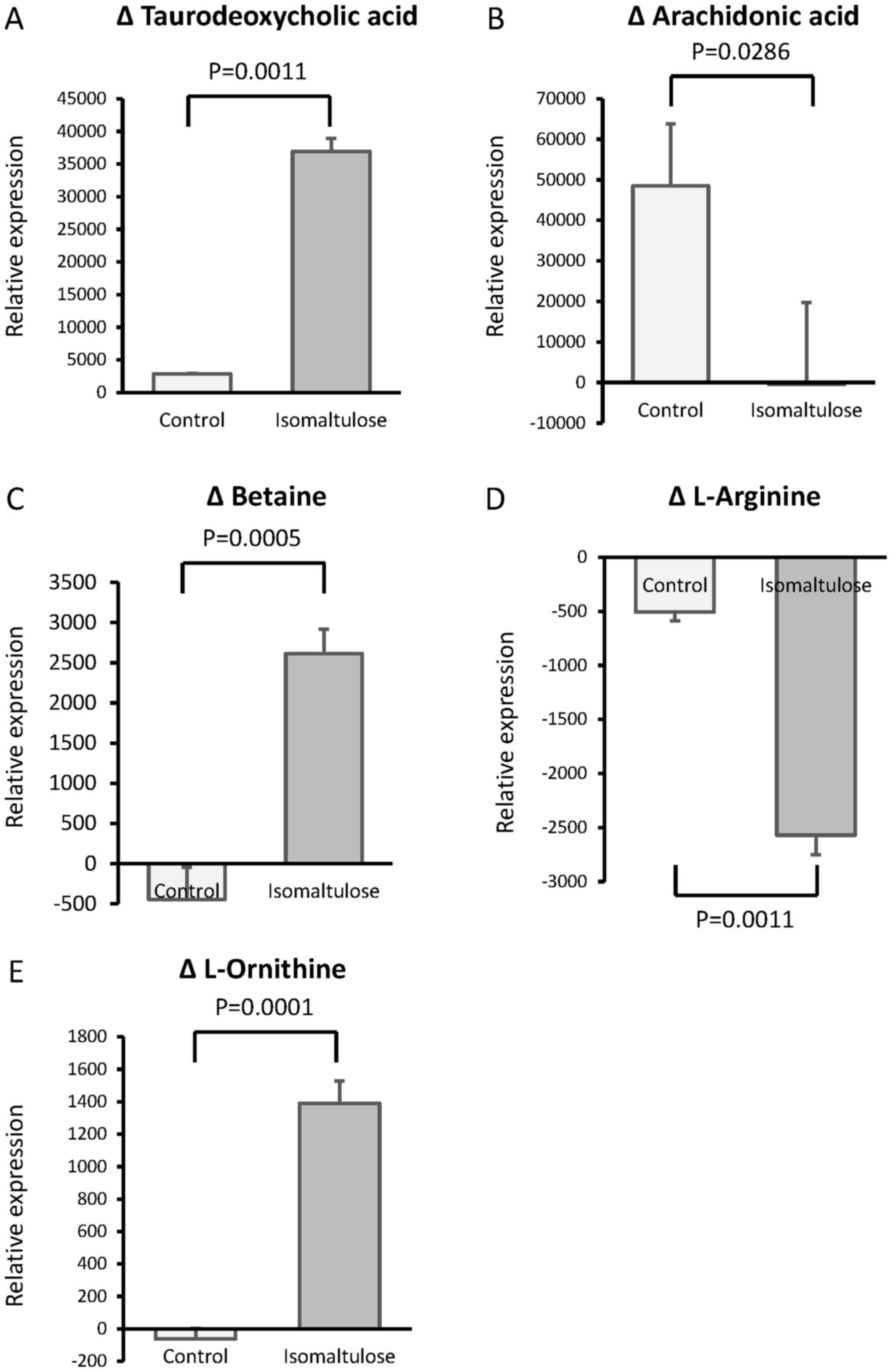
A representative change of metabolite in each
category was an increased taurodeoxycholic acid level in the bile
acid category, a decreased arachidonic acid level in the fatty acid
category, and an increased betaine level in the glycine/serine
category after isomaltulose treatment (Fig. 4A-C). In addition, a significant
decrease was seen in the serum L-arginine level in the isomaltulose
group compared to that in the Control group (Fig. 4D), while the serum L-ornithine
level was significantly increased in the isomaltulose group
compared to that in the Control group (Fig. 4E).
Discussion
In this study, we demonstrated that isomaltulose
improved insulin resistance in patients with NAFLD. Although
isomaltulose did not have a significant effect on the changes in
serum GIP and GLP-1 levels, we showed that isomaltulose
significantly affects various metabolites, in particular,
taurodeoxycholic acid, arachidonic acid, and betaine. Thus,
isomaltulose may have a beneficial effect on insulin resistance
through alterations in various metabolisms, in particular bile
acid, fatty acid, and glycine/serine metabolisms.
Isomaltulose has been reported to improve insulin
resistance in rats and in patients who are obese (19,31).
In agreement with these previous reports, the serum CPR level was
significantly decreased in the Isomaltulose group compared to that
in the Control group in this study. Thus, we demonstrated that
isomaltulose improved insulin resistance in patients with NAFLD. In
this study, serum CPR was used for evaluation of insulin resistance
instead of immunoreactive insulin (IRI). This was because DCPR is
the most significant determinant of insulin secretion increments
(30). Moreover, in patients with
chronic liver disease, the hepatic insulin degradation rate is
decreased, and CPR is more accurate than IRI for the evaluation of
insulin secretion (32).
Furthermore, the IRI level is affected by hemolysis during blood
collection (33) and is inaccurate
in the presence of an anti-insulin antibody (34).
The slow digestive rate of isomaltulose is reported
to affect secretion of GIP and GLP-1, resulting in a reduction of
insulin resistance (14,15). However, in this study, no
significant change was seen in GIP or GLP-1 levels. The reason for
the discrepancy between previous studies and our study remains
unclear, and following are possible explanations (1): The number of enrolled patients may
not have had enough power to detect significant changes or
(2) since plasma dipeptidyl
peptidase-4 activity is accelerated in patients with NAFLD
(35), degradation of GIP and
GLP-1 could be increased in patients with NAFLD.
To investigate possible mechanisms for
isomaltulose-induced suppression of insulin resistance, we
performed a metabolomic analysis and demonstrated that isomaltulose
had significant effects on various metabolites in patients with
NAFLD. A large number of altered metabolites were categorized into
bile acid, fatty acid, or glycine/serine metabolisms. A
representative change in each category was an increased
taurodeoxycholic acid level, a decreased arachidonic acid level,
and an increased betaine level in bile acid, fatty acid, and
glycine/serine metabolisms, respectively. The causal relationships
between these changes in metabolites and the improvement of insulin
resistance remain unclear. However, Qi et al reported that
taurodeoxycholic acid may reduce the increase of phospholipids,
sphingomyelins, and ceramides induced by a high-fat diet, leading
to an improvement of insulin resistance in a mouse model (36). Arachidonic acid is reported to
down-regulate the insulin-dependent glucose transporter gene,
resulting in an increase in insulin resistance (37). In addition, betaine was recently
reported to improve insulin resistance through an activation of
forkhead box O1-induced NLRP3 inflammasomes (38). These previous reports support that
isomaltulose may have improved insulin resistance potentially
through alterations in bile acid, fatty acid, and glycine/serine
metabolisms in this study.
The metabolomic analysis also revealed a significant
decrease in the serum L-arginine level and a significant increase
in the serum L-ornithine level in the isomaltulose group.
L-arginine is reported to inhibit gene expression of insulin
receptor substrate-1, phosphatidylinositol 3-kinase, and Akt in the
insulin signaling pathway, leading to an increase in insulin
resistance (39). L-ornithine is
reported to regulate growth hormone/insulin-like growth
factor-1/insulin-like growth factor-binding protein 3 complex in
muscle tissue, leading to improved insulin resistance (40). Taken together, along with
alterations in bile acid, fatty acid, and glycine/serine
metabolisms, alterations in L-arginine and L-ornithine may
contribute to improvement of insulin resistance in patients with
NAFLD.
A major limitation of this study is small sample
size, and further study is required to verify of our results. In
this study, changes in metabolisms were evaluated by a global
metabolomic analysis. Since environmental factors including outdoor
temperature are known to be associated with insulin resistance and
other metabolisms (41–43), isomaltulose or sucrose was
administered to the all subjects at the same time on the same day
by personal stuffs. Thus, sample size was limited because of the
equalization for environmental factors in this study. Another
limitation is that taste of isomaltulose is slightly different from
that of sucrose and subjects might recognize the difference between
isomaltulose and sucrose. However, taste correlates with chemical
structure (44,45), and it is impossible to have a
control disaccharide with same taste of isomaltulose. In this
study, a random assignment was performed just before the
administration and then, subjects were at rest on a bed and fast
during the procedure. Thus, the taste difference between
isomaltulose and sucrose is considered to have no influence on the
results.
In conclusion, we showed that isomaltulose improved
insulin resistance in patients with NAFLD. In addition, we revealed
that isomaltulose significantly affect various metabolites,
including taurodeoxycholic acid, arachidonic acid, and betaine.
Thus, isomaltulose may improve insulin resistance mainly through
alterations in various metabolisms in patients with NAFLD.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets analyzed in the current study available
from the corresponding author on reasonable request.
Authors' contributions
TK was involved in the conception and design of the
study, acquisition of data, analysis and interpretation of data,
drafting of the article, critical revision of the article for
important intellectual content, and gave final approval of the
version to be submitted. DN and TO were involved in acquisition of
data and drafting of the manuscript. TT was involved in acquisition
of data, revised the article critically for important intellectual
content and gave final approval of the version to be submitted.
Ethics approval and consent to
participate
The study protocol conformed to the ethical
guidelines of the 1975 Declaration of Helsinki, as reflected by the
prior approval of the institutional review board of The Ethical
Committee of Kurume University. All subjects provided written
informed consent to participate in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
NAFLD
|
non-alcoholic fatty liver disease
|
|
GLP-1
|
glucagon-like-peptide 1
|
|
GIP
|
glucose-dependent insulinotropic
polypeptide
|
|
6-0-α-D-glucopyranosyl-D-fructose
|
Isomaltulose
|
|
AST
|
aspartate aminotransferase
|
|
ALT
|
alanine aminotransferase
|
|
LDH
|
lactate dehydrogenase
|
|
GGT
|
γ-glutamyl transpeptidase
|
|
LDL
|
low-density lipoprotein
|
|
BUN
|
blood urea nitrogen
|
|
CPR
|
C-peptide immunoreactivity
|
|
LC-MS
|
liquid chromatography mass
spectrometry
|
|
CE-MS
|
capillary electrophoresis coupled to
mass spectrometry
|
|
TOFMS
|
time-of-flight mass spectrometry
|
|
IRI
|
immunoreactive insulin
|
References
|
1
|
Loomba R and Sanyal AJ: The global NAFLD
epidemic. Nat Rev Gastroenterol Hepatol. 10:686–690. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vernon G, Baranova A and Younossi ZM:
Systematic review: The epidemiology and natural history of
non-alcoholic fatty liver disease and non-alcoholic steatohepatitis
in adults. Aliment Pharmacol Ther. 34:274–285. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kawaguchi T, Izumi N, Charlton MR and Sata
M: Branched-chain amino acids as pharmacological nutrients in
chronic liver disease. Hepatology. 54:1063–1070. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kawaguchi T, Yoshida T, Harada M, Hisamoto
T, Nagao Y, Ide T, Taniguchi E, Kumemura H, Hanada S, Maeyama M, et
al: Hepatitis C virus down-regulates insulin receptor substrates 1
and 2 through up-regulation of suppressor of cytokine signaling 3.
Am J Pathol. 165:1499–1508. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Younossi Z and Henry L: Contribution of
alcoholic and nonalcoholic fatty liver disease to the burden of
liver-related morbidity and mortality. Gastroenterology.
150:1778–1785. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Belfort R, Harrison SA, Brown K, Darland
C, Finch J, Hardies J, Balas B, Gastaldelli A, Tio F, Pulcini J, et
al: A placebo-controlled trial of pioglitazone in subjects with
nonalcoholic steatohepatitis. N Engl J Med. 355:2297–2307. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Armstrong MJ, Gaunt P, Aithal GP, Barton
D, Hull D, Parker R, Hazlehurst JM and Guo K: LEAN trial team,
Abouda G, et al: Liraglutide safety and efficacy in patients
with non-alcoholic steatohepatitis (LEAN): A multicentre,
double-blind, randomised, placebo-controlled phase 2 study. Lancet.
387:679–690. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Akuta N, Watanabe C, Kawamura Y, Arase Y,
Saitoh S, Fujiyama S, Sezaki H, Hosaka T, Kobayashi M, Kobayashi M,
et al: Effects of a sodium-glucose cotransporter 2 inhibitor in
nonalcoholic fatty liver disease complicated by diabetes mellitus:
Preliminary prospective study based on serial liver biopsies.
Hepatol Commun. 1:46–52. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lina BA, Jonker D and Kozianowski G:
Isomaltulose (Palatinose): A review of biological and toxicological
studies. Food Chem Toxicol. 40:1375–1381. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dahlqvist A, Auricchio S, Semenza G and
Prader A: Human intestinal disaccharidases and hereditary
disaccharide intolerance. The hydrolysis of sucrose, isomaltose,
palatinose (isomaltulose), and a 1,6-alpha-oligosaccharide
(isomalto-oligosaccharide) preparation. J Clin Invest. 42:556–562.
1963. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Okuno M, Kim MK, Mizu M, Mori M, Mori H
and Yamori Y: Palatinose-blended sugar compared with sucrose:
Different effects on insulin sensitivity after 12 weeks
supplementation in sedentary adults. Int J Food Sci Nutr.
61:643–651. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mu W, Li W, Wang X, Zhang T and Jiang B:
Current studies on sucrose isomerase and biological isomaltulose
production using sucrose isomerase. Appl Microbiol Biotechnol.
98:6569–6582. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tonouchi H, Yamaji T, Uchida M, Koganei M,
Sasayama A, Kaneko T, Urita Y, Okuno M, Suzuki K, Kashimura J and
Sasaki H: Studies on absorption and metabolism of palatinose
(isomaltulose) in rats. Br J Nutr. 105:10–14. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Keyhani-Nejad F, Irmler M, Isken F, Wirth
EK, Beckers J, Birkenfeld AL and Pfeiffer AF: Nutritional strategy
to prevent fatty liver and insulin resistance independent of
obesity by reducing glucose-dependent insulinotropic polypeptide
responses in mice. Diabetologia. 58:374–383. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ang M and Linn T: Comparison of the
effects of slowly and rapidly absorbed carbohydrates on
postprandial glucose metabolism in type 2 diabetes mellitus
patients: A randomized trial. Am J Clin Nutr. 100:1059–1068. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Maresch CC, Petry SF, Theis S,
Bosy-Westphal A and Linn T: Low glycemic index prototype
isomaltulose-update of clinical trials. Nutrients. 9:pii: E381.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Suzuki M, Shido D, Goto K, Ohno Y,
Miyasaka K and Mizu M: Effects of a palatinose-containing diet with
exercise on progression of diabetic nephropathy and metabolic
syndrome in obese-diabetic rats. Euro J Sports Exerc Sci. 5:27–36.
2017.
|
|
18
|
Arai H, Mizuno A, Sakuma M, Fukaya M,
Matsuo K, Muto K, Sasaki H, Matsuura M, Okumura H, Yamamoto H, et
al: Effects of a palatinose-based liquid diet (Inslow) on glycemic
control and the second-meal effect in healthy men. Metabolism.
56:115–121. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
König D, Theis S, Kozianowski G and Berg
A: Postprandial substrate use in overweight subjects with the
metabolic syndrome after isomaltulose (Palatinose™) ingestion.
Nutrition. 28:651–656. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yamori Y, Mori M, Hori H, Kashimura J,
Sakuma T, Ishikawa PM, Moriguchi E and Moriguchi Y: Japanese
perspective on reduction in lifestyle disease risk in immigrant
Japanese Brazilians: A double-blind, placebo-controlled intervetion
study on palatinose. Clin Exp Pharmacol Physiol. 34:S5–S7. 2007.
View Article : Google Scholar
|
|
21
|
Postic C and Girard J: Contribution of de
novo fatty acid synthesis to hepatic steatosis and insulin
resistance: Lessons from genetically engineered mice. J Clin
Invest. 118:829–838. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
22
|
Legry V, Francque S, Haas JT, Verrijken A,
Caron S, Chávez-Talavera O, Vallez E, Vonghia L, Dirinck E,
Verhaegen A, et al: Bile acid alterations are associated with
insulin resistance, but not with NASH, in obese subjects. J Clin
Endocrinol Metab. 102:3783–3794. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Weckwerth W and Fiehn O: Can we discover
novel pathways using metabolomic analysis? Curr Opin Biotechnol.
13:156–160. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li J, Liu Z, Guo M, Xu K, Jiang M, Lu A
and Gao X: Metabolomics profiling to investigate the pharmacologic
mechanisms of berberine for the treatment of high-fat diet-induced
nonalcoholic steatohepatitis. Evid Based Complement Alternat Med.
2015:8979142015.PubMed/NCBI
|
|
25
|
Watanabe S, Hashimoto E, Ikejima K, Uto H,
Ono M, Sumida Y, Seike M, Takei Y, Takehara T, Tokushige K, et al:
Evidence-based clinical practice guidelines for nonalcoholic fatty
liver disease/nonalcoholic steatohepatitis. Hepatol Res.
45:363–377. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kawaguchi T, Ide T, Taniguchi E, Hirano E,
Itou M, Sumie S, Nagao Y, Yanagimoto C, Hanada S, Koga H and Sata
M: Clearance of HCV improves insulin resistance, beta-cell
function, and hepatic expression of insulin receptor substrate 1
and 2. Am J Gastroenterol. 102:570–576. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kawaguchi T, Kuromatsu R, Ide T, Taniguchi
E, Itou M, Sakata M, Abe M, Sumie S and Sata M: Thrombocytopenia,
an important interfering factor of antiviral therapy and
hepatocellular carcinoma treatment for chronic liver diseases.
Kurume Med J. 56:9–15. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Itou M, Kawaguchi T, Taniguchi E, Sumie S,
Oriishi T, Mitsuyama K, Tsuruta O, Ueno T and Sata M: Altered
expression of glucagon-like peptide-1 and dipeptidyl peptidase IV
in patients with HCV-related glucose intolerance. J Gastroenterol
Hepatol. 23:244–251. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tanabe K, Kitagawa K, Kojima N and Iijima
S: Multifucosylated alpha-1-acid glycoprotein as a novel marker for
hepatocellular carcinoma. J Proteome Res. 15:2935–2944. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yoshikawa A, Kozawa J, Okita K, Yoneda S,
Okauchi Y, Uno S, Iwahashi H, Ohira T, Takiuchi D, Eguchi H, et al:
Preoperative insulin secretion ability and pancreatic parenchymal
thickness as useful parameters for predicting postoperative insulin
secretion in patients undergoing pancreaticoduodenectomy. Endocr J.
59:383–392. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Arai H, Mizuno A, Matsuo K, Fukaya M,
Sasaki H, Arima H, Matsuura M, Taketani Y, Doi T and Takeda E:
Effect of a novel palatinose-based liquid balanced formula (MHN-01)
on glucose and lipid metabolism in male Sprague-Dawley rats after
short- and long-term ingestion. Metabolism. 53:977–983. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Iwasaki Y, Ohkubo A, Kajinuma H, Akanuma Y
and Kosaka K: Degradation and secretion of insulin in hepatic
cirrhosis. J Clin Endocrinol Metab. 47:774–779. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Matulevicius V, Coculescu M and
Urbanavicius V: Immunoreactive insulin in haemolyzed erythrocytes
of normal humans. Physiologie. 17:217–219. 1980.PubMed/NCBI
|
|
34
|
Sakata S, Nagai K, Imai T, Komaki T and
Miura K: A case of diabetes mellitus associated with anti-insulin
autoantibodies without previous insulin injection. J Endocrinol
Invest. 10:407–411. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zheng T, Chen B, Yang L, Hu X, Zhang X,
Liu H and Qin L: Association of plasma dipeptidyl peptidase-4
activity with non-alcoholic fatty liver disease in nondiabetic
Chinese population. Metabolism. 73:125–134. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Qi Y, Jiang C, Cheng J, Krausz KW, Li T,
Ferrell JM, Gonzalez FJ and Chiang JY: Bile acid signaling in lipid
metabolism: Metabolomic and lipidomic analysis of lipid and bile
acid markers linked to anti-obesity and anti-diabetes in mice.
Biochim Biophys Acta. 1851:19–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tebbey PW, McGowan KM, Stephens JM, Buttke
TM and Pekala PH: Arachidonic acid down-regulates the
insulin-dependent glucose transporter gene (GLUT4) in 3T3-L1
adipocytes by inhibiting transcription and enhancing mRNA turnover.
J Biol Chem. 269:639–644. 1994.PubMed/NCBI
|
|
38
|
Kim DH, Kim SM, Lee B, Lee EK, Chung KW,
Moon KM, An HJ, Kim KM, Yu BP and Chung HY: Effect of betaine on
hepatic insulin resistance through FOXO1-induced NLRP3
inflammasome. J Nutr Biochem. 45:104–114. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Liang H, Habte-Tsion HM, Ge X, Ren M, Xie
J, Miao L, Zhou Q, Lin Y and Pan W: Dietary arginine affects the
insulin signaling pathway, glucose metabolism and lipogenesis in
juvenile blunt snout bream Megalobrama amblycephala. Sci Rep.
7:78642017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zajac A, Poprzecki S, Zebrowska A,
Chalimoniuk M and Langfort J: Arginine and ornithine
supplementation increases growth hormone and insulin-like growth
factor-1 serum levels after heavy-resistance exercise in
strength-trained athletes. J Strength Cond Res. 24:1082–1090. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Betz MJ, Slawik M, Lidell ME, Osswald A,
Heglind M, Nilsson D, Lichtenauer UD, Mauracher B, Mussack T,
Beuschlein F and Enerbäck S: Presence of brown adipocytes in
retroperitoneal fat from patients with benign adrenal tumors:
Relationship with outdoor temperature. J Clin Endocrinol Metab.
98:4097–4104. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wei Q, Lee JH, Wang H, Bongmba OYN, Wu CS,
Pradhan G, Sun Z, Chew L, Bajaj M, Chan L, et al: Adiponectin is
required for maintaining normal body temperature in a cold
environment. BMC Physiol. 17:82017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Davies JW and Liljedahl SO: The effect of
environmental temperature on the metabolism and nutrition of burned
patients. Proc Nutr Soc. 30:165–172. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hamor GH: Correlation of chemical
structure and taste in the saccharin series. Science.
134:1416–1417. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Dagan-Wiener A, Nissim I, Ben Abu N,
Borgonovo G, Bassoli A and Niv MY: Bitter or not? BitterPredict, a
tool for predicting taste from chemical structure. Sci Rep.
7:120742017. View Article : Google Scholar : PubMed/NCBI
|